The University of Pennsylvania Health System had an operating profit of $189 million in the first six months of fiscal 2026, up from $117 million in the same period a year ago, the nonprofit reported to bond investors Friday.
Operating income increased, even after Penn put $43 million put into reserves for medical malpractice claims. Two years ago, Penn had recorded charges totaling $90 million for the same purpose.
Here are more details on Penn’s results:
Revenue: Penn had $6.76 billion in total revenue, up nearly 12% even adjusting for the inclusion of Doylestown Health in fiscal 2026. Penn acquired Doylestown last April.
“We’ve had good volume growth over the prior year, particularly in our outpatient activity,” the health system’s chief financial officer, Julia Puchtler, said in an interview.
The system has also had an increase in the acuity level on the inpatient side, she said. That translated into more revenue.
Expenses: The $43 million malpractice charge boosted overall malpractice expenses through December to $125 million, from $69 million in the same period a year ago.
It’s not that Penn is seeing more claims, Puchtler said. “It’s really the average reserve per claim that we’re seeing accelerate,” she said.
Notable: Excluding Doylestown, Penn saw a 5.9% increase in patient volumes, Puchtler said. “That’s mostly outpatient,” she said. “Outpatient surgery, endoscopy, and some of our other infusion therapy are all increased over the prior year.”
Editor’s note: This article has been updated to reflect an additional medical malpractice charge in 2024, bring the total to $90 million.
In the wake of the U.S. Bicentennial, in which Philadelphia was at the center of a yearlong celebration of the country’s 200th birthday, one of the city’s contributions to public health was put on the chopping block.
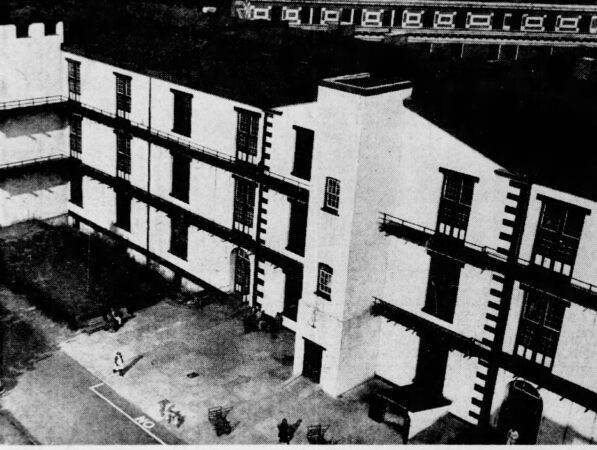
On Feb. 15, 1977, city officials confirmed that Mayor Frank Rizzo was closing Philadelphia General Hospital.
The poorhouse
Philadelphia General Hospital traced its lineage back to 1729, predating even therevered Pennsylvania Hospital, which was founded in 1751 andis generally considered the nation’s first chartered hospital.
Philadelphia General Hospital was originally established at 10th and Spruce Streetsas an almshouse, also known as an English poorhouse.
“The institution reflected the idea that communities assume some responsibility for those unable to do so themselves,” Jean Whelan, former president of the American Association for the History of Nursing, wrotein 2014.
The almshouse was used as housing for the poor and elderly, as well as a workhouse. It also provided some psychiatric and medical care.
It moved in the mid-1800s into what was then Blockley Township, atwhat is now 34th Street and Civic Center Boulevard, and began offering more traditional medical services. The Blockley Almshouse’s barrage of patients and their variety of maladies helped it naturally grow into a teaching tool for nursing and medical students.
And by turn of the 20th century, it had become a full-blown medical center, made official by its new name: Philadelphia General Hospital.
But it held onto its spirit.
Its doors were open to anyone who needed care, no matter that person’s race, ethnicity, class, or income.
Healthcare was a given. Workers saw it as a responsibility.
Even if it wasn’t always the best care.
Poor health
The hospital relied on tax dollars, and as a result was often short on staffing and low on supplies. It was a source of political corruption, scandal,and discord among its melting pot of patients.
Patients in the hallways of Philadelphia General Hospital in the 1940s.
Eventually, it collapsed under the weight of its mission.
Its facilities became outdated, its services could not keep up, and its role as educator was outsourced to colleges and universities.
Philadelphia General Hospital’s closure left a gaping hole in available services in West Philadelphia. It was no longer there to help support the uninsured.
Before it officially closed in June 1977, it was considered the oldest tax-supported municipal hospital in the United States.
“There’s a common misunderstanding that PGH recently has become a poor people’s hospital,” said Lewis Polk, acting city health commissioner, in 1977. “It’s always been a poor people’s hospital. The wealthy never chose to go there.”
Its old grounds are now occupied by several top-rated facilities, including Children’s Hospital of Philadelphia and the University of Pennsylvania medical campus.
A historical marker there notes Philadelphia General Hospital’s nearly 250 years of service to the community.
Johnson & Johnson plans to spend more than $1 billion to build a cell therapy manufacturing facility in Montgomery County near Spring House, the New Jersey pharmaceutical and medical supplies giant said Wednesday.
The Lower Gwynedd Township plant, part of an effort by the company to invest $55 million in the U.S. by early 2029, is expected to employ 500 people when fully operational in 2031, J&J said.
The facility at 1201 Sumneytown Pike will add to J&J’s capacity to make cell therapy treatments for cancer, with a focus on multiple myeloma. That’s a type of cancer that attacks white blood cells in the bone marrow. Cell therapy is the use of engineered immune cells to treat disease.
“Pennsylvania’s proud manufacturing legacy, from steel to today’s medicines and medical technologies and Johnson & Johnson’s roots here for seven decades, are part of why we are investing here.” Joaquin Duato, J&J’s chairman and CEO, said.
Duato spoke during an event at the company’s Spring House research and development campus, where 2,500 scientists work in 70 laboratories. The Montgomery County site is J&J’s largest R&D center and it’s “where most of our discovery efforts start,” Duato said.
The company based in New Brunswick, N.J., employs 5,885 people at 10 Pennsylvania facilities, according to the office of Gov. Josh Shapiro. The Shapiro administration has offered $41.5 million in state support for the J&J project.
“With this investment, we are further cementing our place as a leader in life sciences,” Shapiro said. He said his administration’s efforts to cut red tape are among the reasons companies like J&J “are choosing to double down on their investments” in Pennsylvania.
Eli Lilly & Co. last month announced plans to build a $3.5 billion pharmaceutical plant in the Lehigh Valley to expand manufacturing capacity for next-generation injectable weight-loss medicines.
GSK said in September that it will build a biologics factory in Upper Merion Township, but did not specify how much it would spend there. That project is part of GSK’s plan to spend $1.2 billion on advanced manufacturing facilities.
Johnson & Johnson chairman and CEO Joaquin Duato (left), was joined by Gov. Josh Shapiro and Pa. Dept. of Community and Economic Development Secretary Rick Siger (right) on Wednesday when J&J announced it will spend $1 billion on a cell therapy plant on its campus in Lower Gwynedd Township.
Merck, another New Jersey-based drug giant, last year announced plans for a $1 billion factory and lab near Wilmington. Merck also has major operations in Montgomery County, which is among the top-ranked counties nationally for pharmaceutical manufacturing jobs.
J&J has a long legacy in the Philadelphia region. Among its major acquisitions here was the 1959 purchase of McNeil Laboratories, which later developed Tylenol. The pain reliever is still made at a plant in Fort Washington.
Other major Philadelphia-area J&J deals include the 1999 purchase of Centocor, one of the country’s first biotech companies, and the 2012 deal for Synthes Inc., a Swiss medical device maker with its North American headquarters and major operations here.
Separately from the new cell therapy manufacturing facility, J&J has two expansion projects planned for the Spring House R&D site.
One is a new cell engineering and analytical sciences facility. The other is focused on CAR-T testing and manufacturing during research and development, with the goal of creating personalized therapies more quickly and efficiently. The company did not disclose the cost of those projects.
“At the time, the industry was largely reactive and built around moments of crisis,” he said.
It now has 630,000 active members, who can choose from lightweight medical alert devices worn as a necklace or on the wrist. One of them, which looks like any other smartwatch on first glance, allows users to track health and activity stats.
The company employs more than 600 people and is approaching $250 million in annual revenue. Gross said it is poised to step in as aging-in-place becomes an urgent challenge facing families, healthcare systems, and policymakers.
“Caregiving is now widely recognized as a public health, workforce, and economic issue, not just a personal one,” Gross said. “Burnout, anxiety, and sleep deprivation are increasingly common, yet caregivers are still underserved by technology that focuses almost entirely on emergencies instead of daily reassurance and support.”
From peace of mind to longevity
Gross founded Medical Guardian based on a “simple but deeply personal belief” that “people deserve to age with confidence, dignity, and the freedom to live life on their own terms,” he said.
That was informed by his family’s experience with Gross’ grandmother, Freda, a retired nurse who lived alone later in life and experienced frequent falls. “She was fiercely independent, but those moments created real anxiety for our family,” he said.
She became Medical Guardian’s first member.
The MGMini Lite by Medical Guardian.
“People who are older, frail, or have a disability or chronic illness” need to be able to easily, reliably contact family or emergency services, said Richard C. Wender, who chairs the Department of Family Medicine and Community Health at the University of Pennsylvania’s medical school.
He recommends choosing a system that’s affordable and delivers on promises made. These services can offer more independent options for vulnerable individuals.
“Most people want the same things as they get older, as they did before: control over their daily lives, privacy, and the ability to remain in their own homes and communities for as long as possible,” Gross said. “When done thoughtfully, connected health and safety tools can remove barriers rather than impose them.”
People often find Medical Guardian through referrals from adult children, caregivers, clinicians, and community organizations, Gross said. He noted that such decisions are “often made collaboratively, and our approach is designed to reflect that reality.”
The company also does direct-to-consumer marketing, as well as social media advertising and influencer outreach. And it works closely with health plans, providers, senior living operators, and state programs focused on helping aging adults remain safely at home.
“That blend of consumer and healthcare channels mirrors how aging and caregiving actually happen, in real homes, with real families, over time,” Gross said.
Gross says Medical Guardian members have shared feedback that their devices’ biggest impact is not a dramatic moment, but the everyday reassurance.
Medical Guardian’s MGMini device, which is worn around the neck.
“Feeling steady taking a shower, walking outside without hesitation, or knowing help is there if something feels off,” Gross said. “Those small moments of confidence shape how people experience independence.”
With that in mind, one of the company’s goals is to support people earlier — before a fall, a health scare, or a rushed decision.
“Our services often come years before in-home care or assisted living, which gives us the opportunity to build trust while people are still living independently and confidently,” he said.
Medical Guardian also has wellness advocates, many of whom have social work backgrounds, as well as emergency response specialists and care teams.
“Our platforms use data, automation, and intelligence to notice patterns and surface insights, but when something matters, a real person is always involved,” Gross said.
Philly-based medical device competes with Big Tech watches
Many of the people answering Medical Guardian’s emergency calls, building its software, supporting members, and working with health plans are doing so from Philadelphia, where the company is headquartered. More than half its employees are based in the area.
Geoff Gross, CEO of Medical Guardian, in the Technology Product Innovation Lab at the company’s Center City Philadelphia office.
“We’ve built and scaled this company in Philly, and that matters to us,” Gross said. “There’s a strong work ethic here, a deep healthcare ecosystem, and a sense of community responsibility that aligns with our mission.”
Some of Medical Guardian’s partners are based in the region — such as AmeriHealth Caritas, Independence Blue Cross, and Jefferson Health.
Some may feel that an Apple Watch can do as much as one of Medical Guardian’s devices by providing vital stats, location tracking, and communication capabilities. But Gross said Medical Guardian’s products offer a unique alternative.
“Many of our members do not want dozens of apps or daily charging. They want something reliable, intuitive, and built for real life, especially in moments when clarity and speed matter,” he said.
Gross cited that Medical Guardian can monitor location and, when appropriate, biometrics like oxygen levels or blood pressure. That’s not meant to overwhelm people with data but to create meaningful context for families and care teams.
“For many older adults,” he said, “that focus on usefulness over features is more appealing than a general-purpose smartwatch that tries to do everything.”
Jefferson Health had an operating loss of $201 million in the six months that ended Dec. 31, compared to a $55 million loss the year before, the nonprofit health system said in a notice to bondholders Friday.
The $201 million loss included a $64.7 million restructuring charge related to severance for 600 to 700 people laid off in October and other changes designed to improve efficiency in the 32-hospital system that stretches from South Jersey to Scranton.
Excluding the restructuring expenses, Jefferson’s operating loss was $136.3 million in the first half of fiscal 2026.
Jefferson said in a statement that it continues facing significant financial headwinds, like health systems nationwide, citing rising pharmaceutical costs.
“We remain focused on driving efficiency, advocating for reimbursement rates that better reflect the true cost of care in Pennsylvania, and advancing the long-term stability of our academic health system,” the health system’s chief financial officer Michael Harrington said.
Here are some details:
Revenue: Patient revenue reached nearly $6 billion in the first half of fiscal 2026. The figure for the previous year is not comparable because it does not include Lehigh Valley Health Network for the full six months. Jefferson acquired the system on Aug. 1, 2024.
Jefferson’s total revenue of $8.6 billion included $145.9 million of investment income that directly boosted operating income. Competitors who use heath-system reporting rules do not include investment income in revenue. Jefferson, by contrast, follows rules for higher-education reporting.
Insurance business: Jefferson noted improvement in its health insurance arm. Jefferson Health Plans’ loss in the six months ended Dec. 31 was $90.7 million, compared to a $118.5 million loss in the same period the year before. The number of people insured in the plans climbed to 371,005 from 359,662. Medicaid recipients account for most of that enrollment.
Notable: Both Moody’s Ratings and Standard & Poor’s Ratings Service in December and January revised their outlooks on Jefferson to negative, which means the agencies could downgrade the organization’s credit rating if Jefferson’s finances don’t improve over the next two years.
“The negative outlook reflects the magnitude of current operating losses as well as anticipated difficulties in returning to or near operating profitability for several years,” Standard & Poor’s said.
A Philadelphia jury ordered pharmaceutical and cosmetics giant Johnson & Johnson to pay $250,000 to the family of a York County woman after finding the company’s baby powder product led her to develop cancer.
Gayle Emerson sued Johnson & Johnson in 2019 as part of a nationwide wave of litigation accusing the company’s talc-based baby powder of causing ovarian cancer. Emerson, who was diagnosed with cancer in 2015, died at age 68, months after filing the complaint.
The complaint accused the New Jersey-based company of selling a defective product and failing to warn about its risks.
After a three-week trial, which Common Pleas Judge Sean F. Kennedy presided over,the jury began deliberating Tuesday afternoon and reached its verdict Friday around 2 p.m. During deliberations, jurors asked the judge questions that suggested they grappled with how strongly the evidence showed that external use of baby powder could allow a cancer-causing substance to reach the ovaries.
The verdict was comprised of $50,000 in compensatory damages and $200,000 in punitive damages.
“This token verdict reflects the jury’s appreciation that the claims were meritless and divorced from the science,” Erik Haas, Johnson & Johnson’s worldwide vice president of litigation, said in a statement.
The company plans to appeal the verdict, Haas said.
Johnson & Johnson specifically advertised the product for women, the suit says, stating on the bottle: “For you, use every day to help feel soft, fresh, and comfortable.”
Studies haveconnected talc to ovarian cancer since the early 1970s, according to the complaint. The mineral is excavated from the mines that also contain asbestos, riskingcontamination from the cancer-causing substance.
The Federal Drug Administration asked condom manufacturers in the 1990s to stop dusting their product with talc because of the risk to women.
The company was aware of the research about the increased risk of cancer for women who use the powder on their genital area, the suit says, based on internal documents and public statements.
“Gayle Emerson trusted Johnson & Johnson, and Johnson & Johnson betrayed that trust,” Leigh O’Dell, a Beasley Allen attorney representing Emerson’s family, said in her opening statement.
Attorneys in Pennsylvania aren’t allowed to advise jurors on how much to award in damages, but O’Dell noted in her closing argument that Johnson & Johnson’s net worth is $72.3 billion and a verdict should be “enough” to get the attention of the company’s boardroom.
During the trial, attorneys for Johnson & Johnson said the baby powder, which Emerson used externally, wasn’t responsible for the cancer. Other parts of her feminine care routine, such as douching, are also associated with increased risk of ovarian cancer, the attorneys said, and Emerson had other risk factors such as family history, obesity, and age.
Emerson’s attorneys ignored those risk factors because they have “talc blinders” on, Shaila Diwan, a Kirkland Ellis attorney representing the company, said to the jurors at the outset of the trial.
“Ms. Emerson would have still developed cancer if she never used Johnson’s baby powder,” Diwan said in closing.
It’s important that the jury found that Johnson & Johnson was directly responsibe for Emerson’s cancer but the award is “significantly less than the amount necessary to punish J&J,” O’Dell said in a statement.
While the Philadelphia trial was proceeding, a three-judge panel of a New Jersey appeals court disqualified Beasley Allen from the baby powder litigation in the state for ethical violations. The Alabama-based firm has been accused of receiving privileged information from an attorney who previously represented Johnson & Johnson. The firm said it would appeal the decision.
It’s unclear if the ruling will impact the Pennsylvania verdict, or future Beasley Allen cases outside New Jersey.
Emerson’s is the second talc-related lawsuit to reach a verdict in Philadelphia, after a 2021 trial concluded with the jury siding with Johnson & Johnson.
There are 176 lawsuits similar to Emerson’s pending in the Philadelphia court, and thousands across the nation. Another trial against Johnson & Johnson in a City Hall courtroom is scheduled for April.
Tower Health had an operating loss of $16 million in the first six month of fiscal 2026, according to its report to bondholders Friday. In the same period a year ago, the Berks County nonprofit’s loss was $16.1 million.
Here are some details:
Revenue: Revenue from patient care rose less than 1% to $889.3 million, while total revenue climbed 4.3% to $1.03 billion, thanks to a 34% increase in other revenue.
Cash reserves: Tower reported $244 million in cash reserves on Dec. 31. That translates into enough money to keep operating for 44 days without any new revenue. Both of those figures were at their highest levels since 2022.
The quarterly low was in March 2024, when Tower reported $153 million in cash. That amounted to 30 days of cash on hand. Financially strong systems often have 200 days in reserve.
Family Practice & Counseling Services Network won a $3.4 million federal health center grant that will allow the nonprofit to continue providing medical and mental healthcare in Southwest Philadelphia and other low-income Philadelphia neighborhoods, officials confirmed this week.
The clinic had been part of Resources for Human Development, a Philadelphia human services agency that a fast-growing Reading nonprofit called Inperium Inc. acquired in late 2024. As a federally qualified health clinic since 1992, the clinic had received an annual federal grant, higher Medicaid rates, and other benefits.
Federal rules prohibited the clinic from continuing to retain that status and those benefits under a parent company. That meant Family Practice & Counseling Network had two options: close or spin out into a new entity that would reapply to be a federally qualified clinic.
With financial and operational help from the University of Pennsylvania Health System, Family Practice & Counseling formed a new legal entity last July and reapplied for the grant. Last week, the organization’s CEO Emily Nichols learned that the federal agency that oversees federal health centers awarded it the grant.
A new sign with orange letters outside a former Rite Aid in Germantown announces the arrival of a primary care model new to the Philadelphia region.
ArchWell Health recently opened its first three of eight planned primary care centers here for people with Medicare Advantage, promising convenient and personalized care in neighborhoods with a relative lack of doctors.
Two others have opened on North Broad Street, near Stenton and Susquehanna Avenues, also in former Rite Aid stores.
A privately held company based in Nashville, Tenn., ArchWell says it can offer patients greater access to healthcare throughlower patient-provider ratios.
Itplans to limit each of itsphysicians to no more than 500 patients — about a fifth of the patient load for typical primary care doctors. Nurse practitioners working under the doctors will manage a maximum of 250 patients,officials said.
The approach is built around a financial model that differentiates ArchWell from Medicare-focused competitors already in Philadelphia like Oak Street Health and ChenMed’s Dedicated Senior Medical Centers. ArchWell only accepts patients who have private Medicare or are willing to switch to it. Oak Street and ChenMed also accept traditional Medicare.
Privately run Medicare Advantage plans are increasingly popular among people ages 65 and older who qualify for government-funded Medicare coverage. Advantage plans appeal to people bycovering services, such as dental and vision care, left out of traditional Medicare, but have come under scrutiny for exaggerating how sick patients are to rack up more revenue.
ArchWell sees exclusively working with Medicare Advantage plans as helping doctors to focus solely on the best outcomes for patients, rather than on providing more services to bring in more revenue, a criticism of traditional Medicare, said Doron Schneider, its medical director for the Philadelphia market.
Melissa A. Herd, community relations specialist for ArchWell Health in Philadelphia, is shown outside the company’s Germantown location, which is in a former Rite Aid building.
“You have different incentives, you have different care models, you have different case management models, you have different ways to treat one person versus the other,” Schneider said.
Before starting at ArchWell in late 2024, Schneider worked at Tandigm Health, an Independence Health Group company founded in 2014 with the goal of helping primary care doctors manage costs and improve care for their patients. He learned there how hard it is for doctors to work with different types of insurers and the varied incentives that go with them.
How ArchWell conducts business
ArchWell, which opened its first clinic in 2021 in Birmingham, Ala., operates under contracts with Medicare Advantage plans. The plans give ArchWell a portion of the monthly payment they get from Medicare for each patient. That money is supposed to cover all of the person’s medical costs.
Aetna, UnitedHealthcare, and Devoted Health have contracts with ArchWell to cover the Philadelphia market. ArchWell is close to getting contracts with HealthSpring and Humana, Schneider said. Those five companies had more than 90,000 people in their plans in December, according to federal data.
Aetna and UnitedHealthcare said they work with clinics like ArchWell’s around the country to improve health outcomes and leave patients more satisfied with their experience.
“We are pleased that they are now an option for Aetna Medicare Advantage members in the Philadelphia area,” Aetna said in a statement.
ArchWell declined to provide financial details, such as annual revenue from the more than 80 clinics it had in a dozen states before coming to Philadelphia or how much it spends to open each center. ArchWell representatives also did not disclose who its owners are.
The interior of Archwell Health’s Germantown primary care clinic has Philadelphia-centric images painted on the walls.
Company founder Carl Whitmer worked at Clayton, Dubilier & Rice, a global private equity firm, before founding ArchWell.
“We have partners that are focused on our sustainability and growth,” said Christina Cober, ArchWell’s vice president of marketing.
But companies focused on primary care for seniors haven’t always been as successful as anticipated.
Oak Street, founded in Chicago in 2012, grew rapidly and now services 450,000 patients at 230 centers across the country. It declined to say how many patients it has in Philadelphia. Oak Street arrived here in 2018.
CVS Health bought Oak Street in 2023 for $10.6 billion, anticipating that it would expand to more than 300 centers by this year. Last fall, CVS announced it was closing 16 centers and taking a $5.7 billion write-down on its health-services business, largely because of slower anticipated growth at Oak Street.
ArchWell says itslowerpatient-provider ratios allow more frequent interactions with patients. If a patient is diagnosed with high blood pressure, Schneider said, the message to the patient is: “We’ll see you back in a week. We’ll see you back in two weeks.”
The repeat visits happen with no cost to the member and no extra revenue to ArchWell because all care is supposed to be covered by a monthly payment per member.
ArchWell expects to add about 300 patients per year at each center, said Cober. Staffing at the centers starts out with a physician, a nurse-practitioner, two care navigators, two medical assistants, and a center manager.
Among the early patients at ArchWell’s center on Germantown Avenue is Marcella James, 69, who lives across the street from the clinic and watched as the building was transformed from a shuttered Rite Aid.
“I walked over there one day just to see what it was like and what they offer, and I signed up right away,” James said. James likes her doctor at Temple Health, but ArchWell was irresistibly convenient.
“If I can get the same help or better help from ArchWell is to be seen because I just started with them,” she said.
AmeriHealth Caritas, one of the nation’s largest Medicaid insurers, is closing its in-house pharmacy benefits manager, PerformRx, by the end of this year, the Newtown Square company said in an announcement to employees Wednesday.
Health insurers effectively subcontract with pharmacy benefit managers to oversee drug benefits. They have become increasingly powerful cogs in healthcare and face new restrictions under a law signed by President Donald Trump this month.
OptumRx, a unit of UnitedHealth Group Inc. and one of the three largest PBMs, is scheduled to take over for PerformRx on Jan. 1. OptumRx already provides PBM services to the majority owner of AmeriHealth Caritas, Independence Health Group. Independence is best known for its Independence Blue Cross business.
“This decision reflects evolving market and regulatory landscape, not the performance or dedication of our PerformRx leadership or associates,” the AmeriHealth Caritas announcement to staff said.
Caritas said in a statement to The Inquirer that it expected a “limited impact on jobs, with many functions remaining in-house to support the same high-quality experience for members and providers.”
The company did not elaborate on the market and regulatory changes that precipitated the decision to close PerformRx, which Caritas formed in 1999. PerformRx has contracts in 13 states, including Pennsylvania and Delaware, according to the Caritas website.