Philadelphia’s nonprofit Center for Advocacy for the Rights and Interests of Elders, known as CARIE, is closing next Wednesday after nearly 50 years, the organization’s board announced Tuesday in an email to supporters.
Few details were available on what led to the decision to close abruptly the day before Thanksgiving. CARIE’s new executive director, Brian Gralnick, did not reply to an email or voicemail asking for more information.
Board chair Joan Davitt, an associate professor and geriatric scholar at the University of Maryland School of Social Work who lives in the Philadelphia area, also did not respond to requests for comment.
The organization lists 26 employees on its website. Its most recent audited financial statements show that it had $2.9 million in revenue and a $177,307 operating loss in the year that ended June 30, 2024.
An unaudited financial report for the seven months that ended in January warned that CARIE “was facing financial risks, including the potential default on its line of credit.” At the end of January, CARIE only had enough cash to pay its bills for two weeks, the report obtained by The Inquirer said.
This year, CARIE lost two of its largest contracts, effective next year. Those contracts were to provide long-term care ombudsman services for the elderly in most of Philadelphia and in Montgomery County. An ombudsman’s job is to provide independent advocacy for residents of long-term care facilities and to help resolve complaints about care and living conditions.
In Philadelphia, CARIE had provided the service since 1981, four years after its founding. Philadelphia Corporation for Aging, which manages the contracts, is still finalizing the selection of the new providers.
CARIE started providing ombudsman services in Montgomery County in 2022, but the county’s Office of Aging Services is taking the service back in-house on Feb. 1.
Menio’s successor, Whitney Lingle, lasted just 19 months. She was followed by an internal acting executive director for a year. Gralnick took over in September.
It’s official. Medicare costs will eat up much of older Americans’ Social Security cost-of-living increase next year.
The standard monthly premium for Medicare Part B, which covers outpatient care, doctors’ services, durable medical equipment and preventive service, will be $202.90 in 2026, the Centers for Medicare and Medicaid Services said on Nov. 14. That’s up $17.90, or nearly 9.7%, from $185.00 in 2025.
It’s smaller than the $21.50 increase the Medicare Trustees had forecast earlier but still the second largest dollar jump in program history behind 2022’s $21.60 gain and almost 3.5 times the 2.8% Social Security raise for next year. That means seniors will probably see a drop, again, in their standard of living, experts said.
Seniors were the only ones who saw an increase in poverty in 2024. All other age groups saw a decrease or stayed the same.
“The public is likely to perceive this Part B increase as taking a significant chunk of or even most of their COLA,” said Mary Johnson, independent Social Security and Medicare policy analyst. “In other words, another continuation in relentless cost increases battering consumer finances.”
Monthly Social Security checks will rise $56, on average, starting in January because of the 2.8% COLA, the Social Security Administration said. After the $17.90 increase in Medicare Part B, the average monthly COLA increase is cut to $38.10.
Hold-harmless provision
Such a large increase in Medicare Part B will likely trigger the hold-harmless provision for Social Security recipients with a Social Security benefit of $640 or less, Johnson said.
The Medicare hold-harmless provision prevents the Part B premium increase from being larger than the Social Security COLA. If a premium increase is higher than the COLA, the rule prevents the beneficiary from paying the full increase. The portion of the increase those beneficiaries don’t pay is spread out among others who aren’t protected by the rule.
For those people with a Social Security benefit of $640 or less, the 2.8% COLA next year would mean just less than an $18 per month increase in their Social Security checks. Without the hold-harmless rule, the Part B premium increase would swallow the entire COLA.
In 2022, only about 1.5% of Medicare beneficiaries had their Part B premiums limited by the hold-harmless provision, government data showed. Part B rose $21.60 to $170.10 in 2022 while the average monthly COLA increase boosted Social Security checks by $92.
In 2017, when Medicare premiums jumped 10%, or $12.20, to $134.00 and far outpaced the 0.3%, or $5 average, monthly COLA increase, 70% of Medicare Part B enrollees paid a lower-than-standard Part B premium due to the hold-harmless provision.
Hold-harmless rule isn’t panacea for all costs
The hold-harmless provision can protect seniors from Part B premium surges, but other costs may bite, Johnson said.
“If individuals have other automatic deductions such as for Medicare Advantage or Part D premiums, increases in those premiums could reduce Social Security benefits,” Johnson said. The optional Part D covers prescription drugs.
Some Part D plans are increasing premiums by as much as $50 in 2026, the maximum allowed under a Part D Premium Stabilization Demonstration Program, according to the nonprofit, nonpartisan research organization KFF.
“To complicate things, there are fewer stand-alone Part D plans to choose from,” Johnson said. The total number of prescription drug plans has dropped by half since 2024, KFF said.
Is everyone eligible for hold harmless?
Those who aren’t eligible for the hold-harmless provision include:
New Medicare enrollees
People who aren’t receiving Social Security benefits
High-income earners
What about deductibles?
In addition to higher premiums, higher annual deductibles next year will make health insurance even more expensive for Medicare enrollees.
The annual deductible for all Medicare Part B beneficiaries before insurance covers costs will be $283 in 2026, up $26 from $257 in 2025, CMS said.
Could it have been worse?
The Part B premium could have been higher, CMS said.
“If the Trump Administration had not taken action to address unprecedented spending on skin substitutes, the Part B premium increase would have been about $11 more a month,” CMS said. “However, due to changes finalized in the 2026 Physician Fee Schedule Final Rule, spending on skin substitutes is expected to drop by 90% without affecting patient care.”
Skin substitutes are materials like biologic, synthetic or biosynthetic products that mimic human skin and are used to cover and treat chronic wounds, such as diabetic foot ulcers. The Trump administration reclassified these bandages so they aren’t billed separately. CMS estimates the change would reduce Medicare spending on these products by nearly 90% in calendar year 2026.
Medicare Trustees also estimated earlier this year the standard monthly Part B premium would rise $21.50 to $206.50 in 2026 from $185 in 2025. That would have been more than the $17.90 increase to $202.90 in 2026.
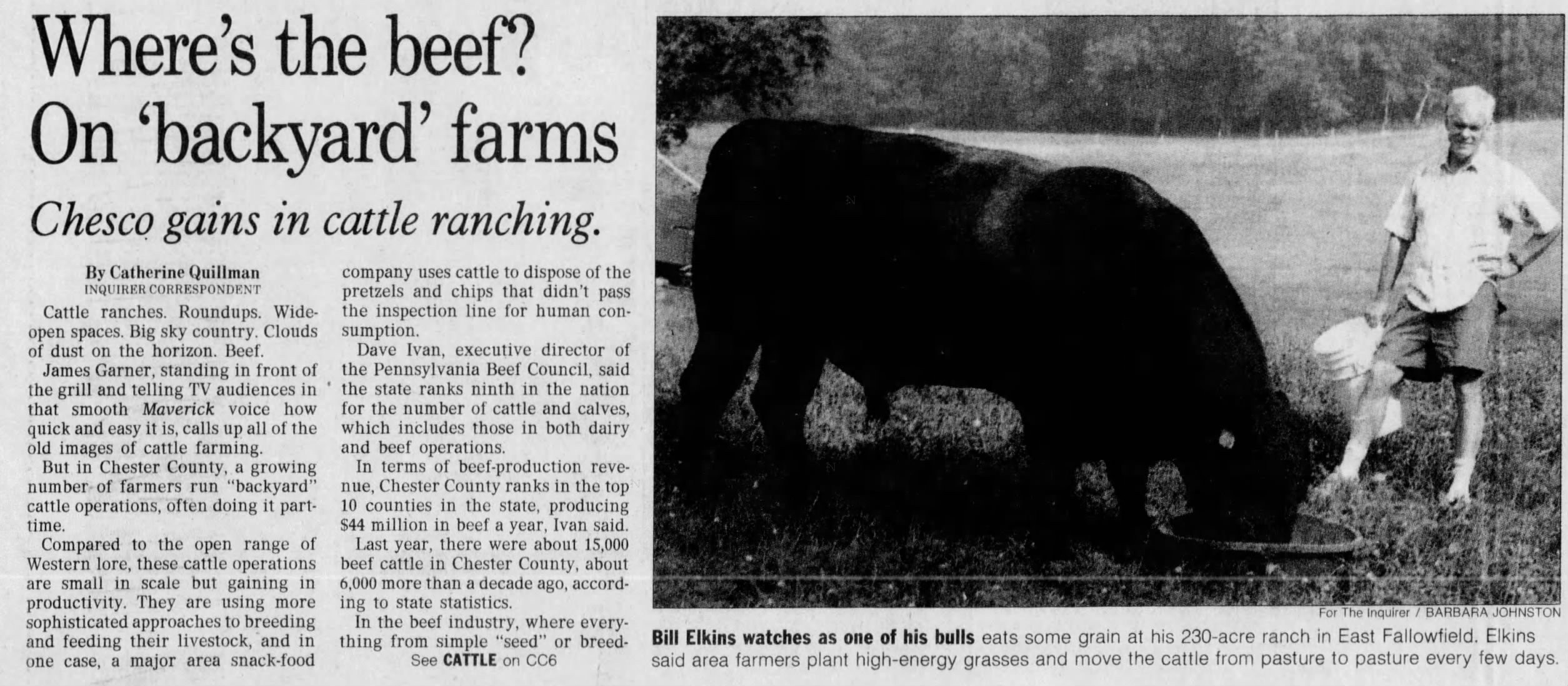
William L. Elkins, 93, of Coatesville, pioneering research immunologist at what is now the University of Pennsylvania’s Perelman School of Medicine, associate professor emeritus of pathology and laboratory medicine, innovative longtime Angus cattle rancher in Chester County, avid sailor, and veteran, died Tuesday, Nov. 11, of complications from pneumonia at Chester County Hospital.
The great-great-grandson of Philadelphia business tycoon William Lukens Elkins, Dr. Elkins fashioned his own distinguished career as a scientist, medical researcher, and professor at Penn from 1965 to 1985, and owner of the Buck Run Farm cattle ranch in Coatesville for the last 39 years.
At Penn, Dr. Elkins conducted pioneering research on how the human immune system fights infection and disease. He collaborated with colleagues in Philadelphia and elsewhere around the country to provide critical new research regarding bone marrow transplants and pediatric oncology.
His work contributed to new and more effective medical procedures at Penn, Children’s Hospital of Philadelphia, and elsewhere, and he instructed students and residents at Penn. But his lifelong love of the fields and rolling hills he roamed as a boy in Chester County never faded, he told Greet Brandywine Valley magazine in 2023.
Dr. Elkins was a lifelong outdoorsman.
“Farming is in my blood,” he said. “So even when I went to medical school and all that, the enthusiasm never left, and I wanted to go back to it.”
So he retired from medicine at 53, and he and his wife, Helen, bought nearly 300 acres of the old King Ranch on Doe Run Church Road in Coatesville. She kept the books and looked after the business. He became an expert on breeding cattle and growing the high-energy grass they eat.
Wearing floppy hats and riding a colorful ATV from field to field, Dr. Elkins worked his land for decades. He mended fences and tended daily to his 120 cows, heifers, and prize bulls.
He championed holistic regenerative farming and used new scientific systems to feed his cattle. He rejected commercial fertilizer and knew all about soil composition, grass growing, and body fat in cattle.
Dr. Elkins and his wife, Helen, married in 1966.
In a 1995 Inquirer story, he said: “Cattle are just like anyone else. If you just turn a few cattle out in a great big field, they will wander around, eat the grass they like best, and leave what they don’t want. That means the less desirable grasses tend to predominate.”
He traveled the country to confer with other cattlemen and helped found the Southeast Regional Cattlemen’s Association in 1994. He sold his beefsteaks, patties, jerky sticks, and kielbasa grillers to private customers online and to butchers and restaurants.
At least one local chef featured an item on the menu called Dr. Elkins’ Angusburger. Lots of folks called him Doc.
He earned his medical degree at Harvard University in 1958 and served two years in the Navy at the hospital in Bethesda, Md. He was a surgical intern in New York and discovered that he preferred the research lab. Before Penn, he worked at the Wistar Institute of biomedical research.
Dr. Elkins graduated from St. Mark’s School in Massachusetts in 1950.
Away from the lab, Dr. Elkins was an ocean sailor, expert navigator, and former boat club commodore. He was active with the Brandywine Conservancy, Natural Lands, and other groups, and was lauded by national organizations for his wide-ranging conservation and wildlife efforts.
He made his farm a haven again for the bobolink grassland songbird and other migratory birds and butterflies that had dwindled. “Buck Run Farm is more about growing grass and trees than beef,” he told Greet Brandywine Valley. “We’re blessed by the land.”
William Lukens Elkins was born Aug. 2, 1932, in Boston. He lived on the family dairy farm in Pocopson, Chester County, when he was young, went to boarding school in Massachusetts for four years, and earned a bachelor’s degree in biology at Princeton University.
He met Helen MacLeod at a party in Washington, and they married in 1966 and had a daughter, Sheila, and a son, Jake. They lived in Center City, Society Hill, and Villanova before moving to the farm. “He was easy to be with,” his wife said.
Dr. Elkins enjoyed sailing and fishing.
Dr. Elkins loved nature, fishing, and baseball, and he followed the Phillies, the Flyers, and other sports teams. “He had a wonderful bedside manner,” his daughter said. “He was a great listener. He really knew how to support people.”
His son said: “He was unassuming and direct. He spoke his mind. He connected with so many different people. He was curious about the world around him.”
His wife said: “He was thoughtful and always concerned about people. He had good humor. He was fun.”
In addition to his wife and children, Dr. Elkins is survived by five grandchildren and other relatives. A sister died earlier.
This article about Dr. Elkins and his ranch appeared in The Inquirer in 1995.
Tower Health’s preliminary financial report in August for fiscal 2025 showed a $5.9 million operating profit, a gain that came thanks for the sale of a shuttered hospital in Chester County.
But that apparent annual profit, the Berks County nonprofit’s first since 2017, turned into a $20.6 million loss when Tower released its annual audit.
Auditors from KPMG decided that Tower should boost medical malpractice reserves and give up on collecting millions owed by patients, Tower said in a statement.
“As part of our standard accounting process, the audited financials for the full year reflect increased malpractice insurance reserves and final adjustments to accounts receivable,” Tower said.
Most of the $26 million swing to a loss came from medical malpractice, but Tower also reduced what is called patient accounts receivable, representing unpaid bills, to $236.6 million from $251.6 million in August’s preliminary results, according to Tower’s audited financial statements that were published Friday.
Separately, Tower reported a $15.9 million operating loss for the three months that ended Sept. 30. That loss was a bit bigger than the $14.2 million loss in the same period last year. Tower’s revenue for the quarter was $501 million, up 4% from $479.8 million last year.
The results for the first quarter of 2026 did not include expenses for Tower’s layoff of 350 employees, or about 3% of its workforce, earlier this month. The cuts hit Pottstown Hospital particularly hard. Tower is eliminating 131 jobs there and eliminating some services.
The closures include the combined intensive care/critical care unit, the Pottstown location of the McGlinn Cancer Institute, and the hospital’s endoscopy center.
Two unions that represent Pottstown employees, the Pennsylvania Association of Staff Nurses and Allied Professionals and SEIU Healthcare Pennsylvania have decried the cuts and called on management to engage in discussions on how to preserve jobs and services.
Pennsylvania’s new budget has $5 million in supplemental payments for the two Delaware County Hospitals that have seen significant increases in patient volumes since Crozer-Chester Medical Center and Taylor Hospital closed in the spring.
Main Line Health’s Riddle Hospital, near Media, is getting $3 million. The amount for Trinity Health Mid-Atlantic’s Mercy Fitzgerald Hospital, in Darby, is $2 million, according to budget documents.
The $5 million will be doubled by a federal match, said Democratic State Sen. Tim Kearney, who represents part of Delaware County. The $5 million is from a fund used to help hospitals the serve a large number of patients with Medicaid and used to go to Crozer Health, Kearney said Friday.
“Since Crozer’s shutdown in April, Riddle’s Emergency Department has experienced an unprecedented surge — 46% more patients than the same period last year, an increase of nearly 4,000 overall,“ the nonprofit said.
Main Line, which also owns Lankenau Medical Center, Bryn Mawr Hospital, and Paoli Hospital, said it has seen 55,000 patients from the Crozer market — a 15% increase over the same time period last year. That figure includes 8,000 patients who went to a Main Line facility for the first time, the health system said.
Trinity Health did not respond to a request for comment.
Shuttered hospitals in limbo
While Riddle and Mercy Fitzgerald have scrambled to accommodate patients who used to rely on Crozer Health, efforts are underway to bring healthcare services back to at least Taylor Hospital in Ridley.
A group from New Jersey called Chariot Allaire Partners LLC has agreed to pay $10 million for the former Crozer-Chester Medical Center in Upland but has not disclosed its plans. That facility served as a key safety provider for a low-income area of Delaware County.
A partnership of Restorative Health Foundation and Syan Investments won an auction for Springfield Hospital for $3 million, but it does not have support from township officials.
Delaware County legislators also obtained $1 million from the state to buy emergency department equipment if one of the closed hospitals, such as Taylor, reopens, Kearney said.
Editor’s note: This story has been updated with additional detail on the funding.
This suburban content is produced with support from the Leslie Miller and Richard Worley Foundation and The Lenfest Institute for Journalism. Editorial content is created independently of the project donors. Gifts to support The Inquirer’s high-impact journalism can be made at inquirer.com/donate. A list of Lenfest Institute donors can be found at lenfestinstitute.org/supporters.
Jefferson Health says it will terminate Lehigh Valley Health Network’s contracts with UnitedHealthcare next year, stating United, the nation’s largest health insurer, is paying less than their negotiated rates, Jefferson said Monday.
The contracts will remain in effect until Jan. 26 for Medicare Advantage patients and until April 25 for patients with commercial insurance through their employer. In the last 18 months, Lehigh Valley Health facilities treated 70,000 people with United insurance, Jefferson said.
“Like all health systems, we are facing significant headwinds as costs rise faster than reimbursement,” Mark Whalen, Jefferson’s chief strategy and transformation officer, said in an email.
“When reimbursement falls substantially below negotiated levels, it threatens our ability to fulfill our mission of providing exceptional care to all patients.”
Whalen said Jefferson will continue working to secure a better deal with United, as it has for more than two years.
United said in a statement that its most recent proposal went to Lehigh Valley in April. “We have yet to receive a counter proposal from the health system, whose last proposal was provided in December 2024 and included a near 30% price hike in the first year of our contract,” the statement said.
Jefferson countered with a statement saying that its dealings with United are not part of a normal contract renegotiation. “This ongoing dispute is caused by United Healthcare’s implementation of a multiyear 30% price decrease that was not agreed to, not accepted and is not sustainable, Whalen said.
The timing of the United announcement is noteworthy. Medicare Advantage open enrollment is underway until Dec. 7 for plans that take effect Jan. 1.
The potential termination of United’s Medicare plans on Jan. 26 puts United’s customers who depend on Lehigh Valley for health services in a quandary. Should they stick with United or switch to another plan, such as those offered by Jefferson’s insurance arm?
United said Jefferson’s decision to make its announcement during open enrollment looked like “a negotiating tactic.”
The Minnesota company has about 27,500 Medicare Advantage enrollees in the main counties served by Lehigh Valley Health doctors, according to federal data from September.
The impasse does not affect Philadelphia-area Jefferson patients with insurance from UnitedHealthcare.
Insurance regulations require notice to patients before contracts end.
In March, Jefferson went out-of-network with Cigna Health for a few weeks during a similar impasse in negotiations. Jefferson and Cigna quickly reached a deal after the termination.
The worst of the coronavirus pandemic that started nearly six years ago is well in the past, but Philadelphia’s biggest nonprofit health systems are still contending with the financial disruption unleashed by the virus that led to thousands of deaths in the area.
Operating conditions for hospitals started improving in 2023, but “the slope of the recovery is a bit more shallow than a lot of health systems had planned for,” said Mark Pascaris, a senior director at Fitch Ratings, one of three major credit ratings agencies.
Patients have returned, but the pandemic led to a resetting of expensesfor labor and supplies at a higher level, Pascaris said. “That’s been the challenge over the last two or three or four years now, trying to manage through a very challenging expense situation,” he said.
To show how the financial landscape has changed, The Inquirer compiled financial data for the region’s six biggest health systems that have fiscal years ending June 30 each year. The analysis compared average operating profits in three years before the pandemic (fiscal years 2017-19) to the results in most recent three years (fiscal years 2023-25).
All six systems showed a substantial drop in a measure of earnings that excludes certain accounting expenses and interest costs. This slice of financial results is known as earnings before interest, depreciation, and amortization. Abbreviated as EBIDA, it’s a primary indicator watched by influential credit ratings agencies.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
The experience of Children’s Hospital of Philadelphia clearly illustrates what has happened: The organization’s aggregate revenue in the most recent three fiscal years was 58% higher than it was in the three years that ended June 30, 2019, but its EBIDA climbed only by half a percentage point.
“Hospitals and healthcare systems across the country continue to face significant headwinds, driven by reimbursement challenges, increased supply and labor costs, uncertain governmental pressures, and the continued ripple effect of the pandemic,” CHOP said in a statement.
Officials at ChristianaCare, Main Line Health, and Temple University Health System echoed CHOP’s remark.
“Margins were far better prior to the pandemic, largely due to lower supply and labor costs,” Main Line’s chief financial officer Leigh Ehrlich said. “Those costs rose sharply during the pandemic and continue to rise.”
ChristianaCare’s CFO Rob McMurray noted: Not only have Medicare and Medicaid rates not kept up with inflation, but more people have those government forms of insurance for people 65 and older and for low-income people.
The nonprofit is expanding from its base in northern Delaware to Southeastern Pennsylvania and is expanding alternative formats, such as hospital-care-at-home and micro hospitals, to reduce costs, McMurray said.
A significant worry for Temple University Health System is the impact of the 2025 budget reconciliation bill, sometimes called the One Big Beautiful Bill Act. The North Philadelphia nonprofit estimates that Medicaid cuts in that law will cost it $519 million over the next 10 years, said Jerry Oetzel, the system’s CFO.
Millions of Americans are already seeing their health insurance costs soar for 2026 as Congress remains deadlocked over extending covid-era subsidies for premiums.
The bitter fight sparked a government shutdown at the start of October. Democrats refuse to vote on government-funding legislation unless it extends the subsidies, while Republicans insist on separate negotiations after reopening the government. Now lawmakers face greater pressure to act as Americans who buy insurance through the Affordable Care Act are seeing, or about to see, the consequences of enhanced subsidies expiring at the end of the year.
Healthcare.gov — the federal website used by 28 states — is expected to post plan offerings early next week ahead of the start of open enrollment in November. But window shopping has already begun in most of the 22 states that run their own marketplaces, offering a preview of the sticker shock to come.
Premiums nationwide are set to rise by 18 percent on average, according to an analysis of preliminary rate filings by the nonpartisan health policy group KFF. That, combined with the loss of extra subsidies, have left Americans with the worst year-over-year price hikes in the 12 years since the marketplaces launched.
Nationally, the average marketplace consumer will pay $1,904 in annual premiums next year, up from $888 in 2025, according to KFF.
The situation is particularly acute in Georgia, which recorded the second-highest enrollment of any state-run marketplace this year and posted prices for 2026 earlier in October. About 96 percent of marketplace enrollees in Georgia received subsidies this year, according to the Center on Budget and Policy Priorities, a liberal think tank that supports extending the subsidies.
Now Georgians browsing the state website are seeing estimated monthly costs double or even triple, depending on their incomes, as lower subsidy thresholds resume.
“We have people saying they will have to choose between their monthly premiums and mortgage,” said Natasha Taylor, deputy director of Georgia Watch, a consumer advocacy group.
For example, a family of four earning $82,000 a year in Georgia could see their annual premium double to around $7,000 for a plan with midrange coverage, according to a CBPP analysis. If that family earned at least $130,000, they would have to pay the full cost of the annual premium, about $24,000 instead of $11,000.
It’s a similar story in other states, where people in higher income tiers will see especially big premium increases as they become ineligible for subsidies. A 60-year-old couple earning $85,000 may have to pay $31,000 for a plan in Kentucky, $28,000 for a plan in Oregon and $44,000 for a plan in Vermont, according to CBPP.
If Congress doesn’t extend the extra subsidies, Georgia could lose around 340,000 people from its 1.5 million-person marketplace, according to an estimate by nonpartisan advocacy group Georgians for a Healthy Future.
The enhanced subsidies had fully covered monthly premiums for millions of lower-income people in the marketplaces. Many of them will have to start kicking in some of their own money starting Jan. 1, while people with higher incomes will see their monthly subsidies shrink. People earning more than 400 percent of the federal poverty line will no longer be eligible for subsidies at all.
The political fallout in Georgia has already begun to reverberate. Rep. Marjorie Taylor Greene (R-Georgia) broke with her party to demand an extension of subsidies, noting her adult children’s premiums are set to double. Greene’s office didn’t respond to a request for comment.
Sen. Jon Ossoff, considered the most vulnerable Democratic incumbent in next year’s midterms, has seized on the issue of rising premiums. An Ossoff spokesman said the senator wants the subsidies extended, pointing to polling showing a majority of Georgians feel the same.
Republican Gov. Brian Kemp, who championed the state’s marketplace, didn’t respond to a request for comment.
Atlanta resident Jody Fieulleteau, 31, said she has been paying $160 a month for a subsidized plan on Georgia’s marketplace. She makes about $40,000 a year styling hair and providing behavioral therapy. She has yet to complete an application to see quotes for plans next year, but her monthly premium is likely to nearly double based on her age, income and Zip code.
Fieulleteau said she rushed to schedule a surgery next week for a problem related to menstruation because she’s concerned about having insurance.
“I’m feeling like I need to get everything done this year because I don’t know what next year is going to look like,” she said in a phone interview.
Taylor, of Georgia Watch, said she finds that consumers often don’t understand that their plans are subsidized, which makes it difficult to explain that the pricey plans they see now could become cheaper if Congress votes to extend the subsidies.
“For your average consumer, they look at the bottom line. What’s my out-of-pocket max,” Taylor said. “I don’t think they’re looking at the minutiae of why their premium is what it is.”
The rising insurance costshighlight the political difficulties faced by Washington lawmakers.
The Congressional Budget Office, the legislature’s nonpartisan bookkeeper, has estimated nearly 4 million fewer people will have marketplace plans a decade from now if the extra subsidies expire.
Republicans say the premium assistance — intended to help people be insuredduring the coronavirus pandemic — are just a Band-Aid for a failure of the Affordable Care Act to rein in the costs of plans. They also say the subsidies were so generous they incentivized fraud, pointing to a CBO estimate that 2.3 million enrollees improperly claimed a subsidy this year.
But 13 House Republicans who face competitive reelection campaigns next year wrote to House Speaker Mike Johnson (R-Louisiana)on Tuesday asking him to consider extending premium assistance.
“Millions of Americans are facing drastic premium increases due to shortsighted Democratic policymaking,” they wrote. “While we did not create this crisis, we now have both the responsibility and the opportunity to address it.”
Sen. Patty Murray (D-Washington) said in a news conference that she heard from families whose premiums are doubling as window shopping started in her state Tuesday. She said she heard similar stories from Idaho and Montana, noting most people who rely on premium assistance live in red states.
“Families are logging on, looking for health coverage for next year, and coming face to face with massive price hikes because Republicans downright refuse to work with us to do something about it,” Murray said.
Insurers have partially blamed the premium hikes on the expiration of the subsidies, saying they’ll cause healthy people to drop coverage, leaving a sicker, more expensive pool of customersbehind. Insurers have also cited higher drug and hospital prices, expensive weight-loss drugs and medical inflation as reasons for raising premiums.
But if Congress acts to extend the subsidies, even after open enrollment begins Nov. 1, some plans may be willing to lower premiums, said David Merritt, senior vice president of external affairs at the Blue Cross Blue Shield Association, whose memberplans are sold in all marketplaces. Adjusting rates lower would get more complicated after Dec. 31, he said.
Even if Congress does extend the subsidies, consumer advocates saydamage has already been done.
Many people will visit theinsurance marketplaces and decide to forgo coverage after seeing pricey 2026 plans, they said, and not revisit their decision even if subsidies are restored.
Amid persistently higher costs, three Philadelphia-area health systems have cut expenses over the last two years by changing how they account for investments in facilities and equipment. The change significantly boosted operating income in all three cases.
ChristianaCare and Main Line Health are now spreading the cost of buildings and building improvements over as many as 80 years, they said in their fiscal 2025 audited financial statements. That is double the maximum number of years they previously used to calculate what accountants call depreciation expense. Thomas Jefferson University made a similar change last year.
All three health systems use PricewaterhouseCoopers LLP as their auditor. The firm, which did not respond to a request for comment, also has Philadelphia health-system clients that have not extended their depreciation schedules.
The term depreciation expense refers to the way hospitals and other businesses allocate the cost of a building, a piece of equipment such as an MRI machine, or even software to manage patient records across the number of years the asset is likely to be used.
It’s a noncash expense because the money used to make the purchase is recorded elsewhere in the financial statements. Several financial and accounting experts said the change could be seen as cosmetic.
“It’s not affecting operations. It’s not increasing their revenues. It’s not decreasing their cash expenditures. It is purely a bookkeeping entry,” said Steven Balsam, a professor of accounting at Temple University’s Fox School of Business.
Main Line Health
At Main Line, the extended depreciation schedule reduced the expense by an estimated $37.5 million. That helped the system achieve a small, $4 million operating profit for the first time since fiscal 2021, when federal COVID-19 aid buoyed hospitals.
Without the depreciation savings, Main Line would have had an operating loss of $33.5 million in the year that ended June 30, compared to a $61 million operating loss in fiscal 2024.
Asked for comment, Main Line’s chief financial officer Leigh Ehrlich noted that the system’s financial performance had improved, thanks to “increased patient volumes and continued focus on expense management.”
Excluding noncash depreciation and amortization in each of the last two years, Main Line’s operating income improved to $127.8 million from $96.7 million.
ChristianaCare
ChristianaCare reviewed the depreciation schedules of fixed assets “as part of our ongoing commitment to maintain accurate and reliable financial reporting,” the nonprofit’s chief financial officer Rob McMurray said in an email. The result was a $24.4 million reduction in depreciation expense.
The review also resulted in a $9 million write-off of unspecified assets, which meant that in fiscal 2025 the benefit to operating income was $15 million, McMurray said.
ChristianaCare’s operating income in the year that ended June 30 was $35.5 million, or $20.5 million without the accounting change. The organization had $126.2 million in operating income in fiscal 2024.
Thomas Jefferson University
Last year, Thomas Jefferson University opened its $762 million Honickman Center in Philadelphia. Normally, taking a building like that into service would increase depreciation expense.
Instead, Jefferson’s depreciation expense fell by $68 million, according to its audited financial statement for the year that ended June 30, 2024. The decline happened after Jefferson opted to spread the cost of all buildings and building improvements over as many as 70 years, according to the depreciation schedule in its financial statement.
Even with the depreciation change, Jefferson’s operating income in fiscal 2024 was extremely narrow, at $1.34 million on nearly $10 billion in revenue that year.
The benefit of lower depreciation expense continued in fiscal 2025, as it will in future years for ChristianaCare and Main Line.
Depreciation expense at other local systems
Most Philadelphia-area health systems use a schedule for depreciating buildings and building improvements that maxes out at 40 years, an Inquirer review of financial statements found.
“You’re constantly modernizing your facilities to allow for the delivery of medicine based on current times,” Temple University Health System chief financial officer Jerry Oetzel said in an interview. “Who knows 15 years from now? We don’t have clear insight, but it’s probably going to be more home care.”
That’s why Temple hasn’t adopted a longer depreciation schedule. “It’s just a savings in operating expenses without the benefit of any cash behind it,” Oetzel said.
Editor’s note: This article has been updated to remove a reference to American Hospital Association guidelines.
The University of Pennsylvania Health System, the Philadelphia region’s biggest provider of cancer care and a national leader in developing new treatments, is spending more than $500 million on two new cancer facilities in Philadelphia and central New Jersey to keep growing.
“What we’ve seen pretty consistently is that demand is there to meet any capacity increases,” Julia Puchtler, the health system’s chief financial officer, said in an interview about fiscal 2025 financial results.
Penn is not alone in its push to expand cancer services. Jefferson’s Sidney Kimmel Cancer Center, Temple’s Fox Chase Cancer Center, and the MD Anderson Cancer Center at Cooper are pushing into the suburbs to reach more patients.
The same thing is happening nationally as financially pressured health systems are looking for ways to increase revenue in a growing and lucrative market for cancer care.
Penn stands out locally for the scale of its investment in a strategy to deliver cancer care seamlessly across its seven hospitals and a growing network of outpatient clinics, with the expectation that patients will keep coming back for their ongoing health needs.
Penn sees an opportunity to expand its market share even more, as cancer diagnoses rise. The U.S. is expected to see a nearly 40% increase in cancer diagnoses between 2025 and 2050, according to the Philadelphia-based American Association of Cancer Research.
Experts attribute the rise to a wide variety of factors, from better early detection, to longer life spans, and to environmental exposures that are poorly understood.
Much of Penn’s investment is in outpatient facilities, including a $270 million center being built in Montgomeryville that will have radiation oncology and an infusion center. “More and more patients want to receive care closer to home,” according to Lisa Martin, a senior vice president at Moody’s Rating. “All of that is really what’s behind all of this investment.”
Cancer treatment overall is profitable. At Penn, cancer services account for up to 60% of the system’s operating margin by one simple measure that subtracts direct costs from direct revenue and excludes back-office expenses and other centralized costs.
Puchtler attributed the profitability of cancer care to the prevalence of drugs, such as chemotherapy, that Penn can buy at a discount, while getting the full price from insurers, and the higher percentage of younger cancer patients with better-paying private insurance than is typical for many healthcare services.
The expansion efforts are expensive in an industry where the consumers both benefit from advances and pay ever-rising healthcare costs. Proton therapy, in particular, costs more, but has not yet been proven to have better outcomes across a wide range of cancers.
The intensifying competitive landscape
Penn treats about one-third of adults with cancer in its market area, which stretches from central New Jersey to the Susquehanna, according to Robert Vonderheide, who is director of Penn’s Abramson Cancer Center and leads all of Penn’s efforts in oncology treatment and research.
Penn counted 47,053 new cancer patients in the 12 months that ended June 30, up 40% from five years ago, according to Penn. The system has 14 locations where patients can receive chemotherapy and even more radiation oncology sites.
Competitors are also trying to expand their reach, and Temple’s Fox Chase Cancer Center is succeeding.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Fox Chase had 21,442 new patients in fiscal 2025, up 148% from 2020, the nonprofit said. Fox Chase has added suburban offices in Voorhees and Buckingham, Bucks County, and is expanding its infusion capacity at its main campus on Cottman Avenue. Fox Chase has a significantly smaller footprint than Penn, with six locations for infusions and four for radiation.
The MD Anderson Cancer Center at Cooper said it had 4,326 new patients last year, up 27% over the last five years. Cooper has taken the MD Anderson Cancer Center brand to the former Cape Regional Medical Center, which it acquired last year and which used to be part of the Penn Cancer Network. Cooper also offers cancer services at its new Moorestown location.
Jefferson Health’s Sidney Kimmel Cancer Center did not respond to requests for patient data, but has in recent years opened cancer center locations at its Torresdale and Bucks County Hospitals. Jefferson’s cancer center also attained the highest designation from the National Cancer Institute last year — the Philadelphia region’s third comprehensive cancer center, matching Penn and Fox Chase.
Lancaster County resident Susan Reese, 56, said she experienced smooth cooperation between her doctor at Penn’s Lancaster General Hospital and the team at HUP during her treatment for non-Hodgkin lymphoma.
“I never had any question in my mind that one doctor didn’t know what the other doctor was doing,” said Reese, who received CAR-T therapy at HUP in September 2022. Penn has since started offering CAR-T at Lancaster General.
After she relapsed in early 2023, she came back to HUP for a stem cell transplant. She could have gone to Penn State Health’s Hershey Medical Center for that. It’s significantly closer to her home in Willow Street, but she wanted to stay within the Penn system.
Reese’s experience of integration of services at HUP and Lancaster General is what Penn is aiming for in a territory that stretches from central New Jersey to central Pennsylvania.
Oncologist Robert Vonderheide, director of Penn Medicine’s Abramson Cancer Center, oversees all Penn’s cancer services and research.
Electronic medical records help with the integration needed to ensure the thousands of cancer patients Penn physicians treat annually get the most advanced care possible, according to Vonderheide, whose research focuses on cellular immunotherapies.
“We treat patients’ cancers now in a very precise way; the precise mutation, the precise type of chemotherapy, the precise dose” are the focus for doctors, Vonderheide said. “This is no longer appropriate for the telephone game. This has to be data-driven.”
Reese’s decision to stay within Penn is part of a broader trend of patients tending to receive all their care within one health system, according to Rick Gundling, a healthcare expert at the Healthcare Financial Management Association in Washington, D.C.
That’s particularly important in oncology, which typically involves multiple specialties, such as medical oncology, radiation oncology, and surgical oncology, he said.
“Seamless coordination across all those disciplines really makes it a better patient experience and clinical experience because it reduces delay, improves access,” Gundling said.
Taking advanced treatments from HUP to the network
Part of Penn’s strategy is to begin offering advanced services at locations beyond HUP. That’s where Penn pioneered CAR-T cell therapy, which harnesses the immune system to attack cancer, and for years that was the only place Penn offered it.
HUP still performed the bulk of the CAR-T treatments for blood cancers, 123 inpatient cases and 14 outpatient cases last year, but now CAR-T is also available at Lancaster General and at Penn’s Pennsylvania Hospital in Center City.
Fox Chase was the next biggest center in the region for the relatively new treatment that Penn scientist Carl June and his research teams helped develop. For the fiscal year that ended June 30, 2025, Fox Chase had 21 inpatient cases and 67 outpatient cases, the center said.
In the Penn system, certain kinds of bone marrow transplants also used to be available only at HUP. “Now we do them at HUP and Pennsylvania Hospital,” Vonderheide said.
Even the most complicated pancreatic surgeries are going to be done at Princeton, in conjunction with experts at HUP, Vonderheide said. Penn held a ceremonial groundbreaking Monday for the hospital’s $295 million cancer center.
Remaining only at HUP are bone marrow transplants that use another person’s cells to treat blood cancers, Vonderheide said. HUP performed 118 of those so-called allogeneic bone marrow transplants on the top floor of its $1.6 billion patient pavilion, now known as the Clifton Center.
Pennsylvania’s next-biggest provider of the treatment was Hershey Medical Center, near Harrisburg, with 71, according to state data.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Penn started offering proton therapy at HUP in 2010, and expanded its availability in the last three years to Lancaster General and Voorhees, through a joint venture with Virtua Health. Those two centers only have one proton machine each, compared to five at HUP.
It’s a type of radiation that is designed to precisely target tumors and do less damage to surrounding tissues. That makes the treatment, which costs more, particularly helpful for children, and it is proving beneficial for treating certain neck and throat cancers.The use of proton therapy for the more common prostate cancer has been more controversial.
Penn’s fourth proton center, with two machines, is under construction and is expected to open at Presbyterian in late 2027. When that $224 million center opens, Penn will have more proton treatment rooms than the entire West Coast, said Jim Metz, chair of radiation oncology at Penn.
Currently about 10% of Penn’s roughly 10,000 annual radiation oncology patients are treated with protons, though it’s a higher percentage at locations with proton machines, Penn said.
Penn officials have noted that some cancer patients come to Penn for proton therapy. Even when it’s not appropriate for them, they tend to stay within Penn. “We have seen, when we build protons, our market share increases, ” Metz said.
Editor’s note: This article has been updated with more recent Fox Chase data.