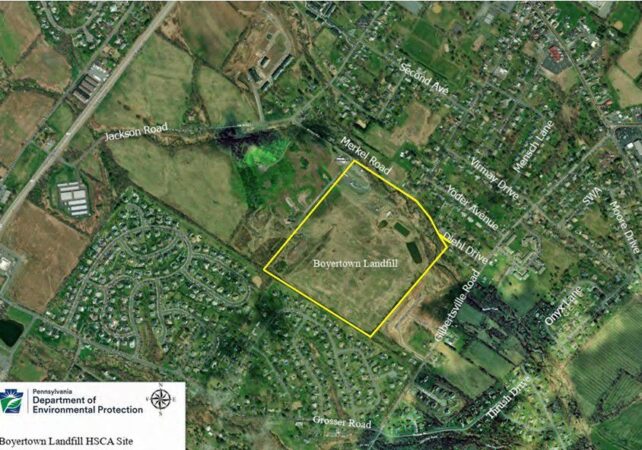
Residential waste, construction and demolition debris, as well as sewage treatment plant sludge, were dumped for decades at the 30-acre Boyertown Sanitary Landfill in northern Montgomery County until it was capped in 1987.
As state and federal officials mull whether to add the landfill to the national Superfund list, a well used by nearby Gilbertsville Elementary School has tested positive for human-made polyfluoroalkyl substances, known as PFAS.
The school is about 3,000 feet from the landfill property border and is within the Boyertown Area School District. Minister Creek passes through the property, and two residential neighborhoods are nearby.
Scott Davidheiser, the district’s superintendent, sent a letter to staff and students’ families Monday alerting them to the test results, which were made known during a Pennsylvania Department of Environmental Protection (DEP) public information session on the landfill on Dec. 10.
Gilbertsville Elementary tested at an annual average of 6.7 parts per trillion (ppt) for PFAS. That falls under acceptable limits by current state standards of 14 ppt.
However, it would exceed federal maximum contaminant level standards of 4 ppt set to go into effect in 2031 if not addressed.
Davidheiser’s letter said the district “remains committed to safety in all areas, including water safety.” The district has hired Suburban Water Technology Inc. to develop a water safety plan to lower annual average PFAS levels to within federal standards.
District officials plan in January to discuss a plan to lower the levels.
<iframe title="Boyertown Sanitary Landfill and PFAS contamination" aria-label="Locator map" id="datawrapper-chart-1kgam" src="https://datawrapper.dwcdn.net/1kgam/1/" scrolling="no" frameborder="0" style="width: 0; min-width: 100% !important; border: none;" height="581" data-window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
What are PFAS?
PFAS are a group of chemicals manufactured by industry for use in consumer products since the 1940s. There are thousands of different PFAS, some of which have been more widely used and studied than others.
Exposure to them has been shown to impact the health of humans and lab animals, but the extent is still being studied.
Standards for maximum acceptable levels of the compounds in drinking water have created confusion in recent years.
The EPA was slow to set standards, so states began setting their own. Pennsylvania set different levels to start in 2024 for various types of PFAS: 14 ppt for perfluorooctanoic acid (PFOA) and 18 ppt for perfluorooctane sulfonic acid (PFOS).
However, the EPA, under the Biden administration, then set the first federal standards, which would supersede state standards. The rule said that PFOA and PFOS can’t exceed 4 ppt. And, it set standards for other compounds within the PFAS family. The regulations were set to go into effect in 2027.
However, the EPA, under the Trump administration, rolled back some provisions by announcing it would keep the standards for PFOA and PFOS, but delay enforcement until 2031. And, it said it would reconsider the limits on the other compounds.
As a result, the PFAS level at Gilbertsville Elementary School’s current level would exceed the federal level if not brought down by 2031.
What’s the Boyertown Landfill?
Officials with the state Department of Environmental Protection and U.S. Environmental Protection Agency have been deciding since 2023 whether the Boyertown Landfill, in Douglass Township, should be named a Superfund site after test samples showed PFAS in nearby private wells.
The landfill and surrounding property are owned by the Boyertown Sanitary Disposal Co. It is set on a wider 60-acre parcel at 300 Merkel Road in Gilbertsville. The property contains raw and pretreated leachate storage lagoons, buildings housing leachate pretreatment facilities, and stormwater management basins and swales.
The unlined landfill stopped accepting solid waste in 1985. It had accepted municipal waste, office trash, and construction debris. It took in significant amounts of municipal sewage treatment plant sludge and industrial waste.
In last week’s informational session, the DEP said water sampling around the area of the landfill in 2024 and 2025 showed multiple locations containing various PFAS compounds.
State officials said they have installed carbon-activated filtration systems in residential wells within a half-mile of the landfill that tested above 4 ppt, according to an account of the meeting in Pottstown’s local newspaper, The Mercury.
The newspaper reported that the DEP, however, will not provide similar assistance to Gilbertsville Elementary School because it is part of a small public water system and is required to remediate contamination.