WASHINGTON — Four centrist Republicans broke with Speaker Mike Johnson on Wednesday and signed onto a Democratic-led petition that will force a House vote on extending for three years an enhanced pandemic-era subsidy that lowers health insurance costs for millions of Americans.
The stunning move comes after House Republican leaders pushed ahead with a health care bill that does not address the soaring monthly premiums that millions of people will soon endure when the tax credits for those who buy insurance through the Affordable Care Act expire at year’s end.
Democrats led by Minority Leader Hakeem Jeffries of New York needed 218 signatures to force a floor vote on their bill, which would extend the subsides for three years.
Republican Reps. Brian Fitzpatrick, Robert Bresnahan and Ryan Mackenzie, all from Pennsylvania, and Mike Lawler of New York signed on Wednesday morning, pushing it to the magic number of 218. A vote on the subsidy bill could come as soon as January under House rules.
“Unfortunately, it is House leadership themselves that have forced this outcome.” Fitzpatrick said in a statement.
Johnson told reporters Wednesday that “I have not lost control of the House” and he noted that Republicans have a razor-thin majority that allows a small number of members to employ procedures that would not usually be successful in getting around leadership.
The revolt against GOP leadership came after days of talks centered on the health care subsidies.
Johnson had discussed allowing more politically vulnerable GOP lawmakers a chance to vote on bills that would temporarily extend the subsidies while also adding changes such as income caps for beneficiaries. But after days of discussions, the leadership sided with the more conservative wing of the party’s conference, which has assailed the subsidies as propping up a failed marketplace through the ACA, which is widely known as “Obamacare.”
House Republicans pushed ahead Wednesday a 100-plus-page health care package without the subsidies, instead focusing on long-sought GOP proposals designed to expand insurance coverage options for small businesses and the self-employed.
Fitzpatrick and Lawler tried to add a temporary extension of the subsidies to the bill, but were denied.
“Our only request was a floor vote on this compromise, so that the American People’s voice could be heard on this issue. That request was rejected. Then, at the request of House leadership I, along with my colleagues, filed multiple amendments, and testified at length to those amendments,” Fitzpatrick said. “House leadership then decided to reject every single one of these amendments.
“As I’ve stated many times before, the only policy that is worse than a clean three-year extension without any reforms, is a policy of complete expiration without any bridge,” Fitzpatrick said.
Lawler, in a social media post, similarly said that “the failure of leadership” to permit a vote had left him with “no choice” but to sign the petition. He urged Johnson to bring the plan up for an immediate floor vote.
Jeffries, for several weeks, had called on Republicans to sign his discharge petition. He particularly challenged Republicans in competitive congressional districts to join the effort if they really wanted to prevent premium increases for their constituents.
“Mike Johnson needs to bring the bill to the floor today,” Jeffries said. “Our position from the very beginning was that we are standing on the right side of the American people who want to see the Affordable Care Act tax credits extended, and we’re appreciative that we now have the bipartisan coalition to get that done.”
Path ahead is uncertain
Even if the subsidy bill were to pass the House, which is far from assured, it would face an arduous climb in the Republican-led Senate.
Republicans last week voted down a three-year extension of the subsidies and proposed an alternative that also failed. But in an encouraging sign for Democrats, four Republican senators crossed party lines to support their proposal.
Senate Majority Leader John Thune, R-S.D., argued against the Democratic extension as “an attempt to disguise the real impact of Obamacare’s spiraling health care costs.”
Pediatrician Kristin Sohl has lost count of how many times parents of children with autism have asked her for a prescription for leucovorin — the drug thrust into the spotlight after President Donald Trump touted it at a White House event this fall.
Since September, despite the rising queries, Sohl has typically told her patients no.
Early clinical trials of the drug showed hints of promise in boosting communication and cognition for some children with autism. But the studies have been small, often just a few dozen participants. Normally, approval by the Food and Drug Administration comes only after years of large-scale testing. But Trump’s pledge to fast-track the drug in September, bypassing that process, has left many doctors on the front lines divided.
“It leaves me as a practicing physician with a lot of unanswered questions,” said Sohl, a professor of pediatrics at the University of Missouri School of Medicine, who has been working in the field of autism for over 20 years.
As interest in the drug surges, Facebook groups devoted to it are swelling in membership, message boards are inundated with questions, and Google searches are climbing. Physicians, who typically rely on evidence-based guidelines and clear treatment algorithms, are finding that with leucovorin they must — lacking robust scientific data — improvise. Some are cautiously moving forward with prescribing the drug, but many are still holding off.
At Children’s National Hospital in Washington, D.C., neurodevelopmental pediatrician Sinan Turnacioglu said the hospital convened a meeting of various departments — including those specializing in autism, developmental pediatrics, genetics and psychiatry, as well as primary care doctors — to come up with a systemwide policy. Their conclusion: that they would like to see more robust research before prescribing it.
Peter Crino, chair of neurology at the University of Maryland School of Medicine and who runs a clinic for neurodivergent adults, likewise said he believes the medication is not ready for prime time.
“People are asking me a lot about it, but I do not prescribe it. Gosh I hope there will be something to the drug and it will help people in the future, but the data is simply not there yet,” he said.
Limited evidence
Each conversation Sohl has with families unfolds differently, she said, shaped by a child’s history, a parent’s worry, a flicker of hope. But the script she follows is steady: she lays out what research has shown — and what it doesn’t — about the treatment, then asks what the family hopes the drug might change.
In a field with no cure and few therapies, she uses that same framework to guide discussions about the other latest supposed breakthroughs drifting across social media — broccoli extracts, CBD oil, stem cell therapy, and more. The goal isn’t to dismiss any ideas outright but to ground them in evidence, or show the lack of it, before families decide what to do next.
For leucovorin, Sohl’s main message is that “we’re not on solid science yet.” However, there are “potential suggestions of benefit.”
Leucovorin or folinic acid has a long history of use in the context of cancer for about 50 years. It’s been shown to protect healthy cells from the toxic effects of one particular chemotherapy drug and to enhance the effectiveness of another one. Side effects were very minimal but in cancer patients have included nausea and fatigue.
For some children with autism, the immune system may produce antibodies that block the body’s ability to move folate — a vitamin essential for cell growth and DNA production — into the brain. Leucovorin, a prescription form of folate, offers a potential workaround. It crosses the blood-brain barrier by a different route, delivering the nutrient where it’s needed.
The U.S. clinical trial that got Trump’s attention is being conducted by Richard E. Frye, a pediatric neurologist who was formerly an associate professor at Arizona Children’s Hospital in Phoenix. Its design was considered the gold standard — a randomized, double-blind placebo-controlled trial — but it only had 48 children, ages 5 to 12, in it. In the trial — published in 2018 in the journal Molecular Psychiatry — the drug was well-tolerated and the parents and doctors reported improvements in communication and behavior.
Frye said in an interview that leucovorin did not work on all of his patients. But it did work for many and that children with no verbal utterances began showing meaningful word approximations, for example, and that those with phrase speech began forming full sentences.
There have been four subsequent trials in other countries, and all four of them also reported significant improvements and no serious harm. But they were also very small. A study in France with 19 patients was published in 2020, in Iran with 55 patients in 2021, in India with 40 patients in 2024, and in China with 80 patients in 2025.
The Trump administration latched onto promising research and promoted efforts to expand access to leucovorin for autism, despite the lack of large-scale clinical trials.
But since then, doctors have been proceeding cautiously. At least two influential medical societies have come out with their own interim recommendations. The American Academy of Pediatrics and the Society for Developmental & Behavioral Pediatrics both do not recommend the routine use of leucovorin for children with autism. But the AAP left an opening for doctors to prescribe it, stating that pediatric care providers “are encouraged to engage in shared decision-making with families who inquire about or request leucovorin, providing clear information about current evidence and potential risks.”
Crino said that many medical research papers — including those on leucovorin — are written in ways families can understand, and he encourages patients and their families to read the primary studies themselves. He often reviews the papers with them, he added, pointing out the limitations of the research. In the 2024 study, which was published in the European Journal of Pediatrics, for example, the authors reported that many children showed improvements in speech, but none went from nonspeaking to speaking, and the study offered no evidence about whether those changes affected daily life.
“There is a lot going on in scientific research that is getting twisted,” he said.
Turnacioglu said that some of his patients receive leucovorin from other providers. In those cases, he focuses on monitoring their progress by first establishing a baseline assessment of language and adaptive skills and then repeating the same evaluations periodically to track any changes.
In those cases, he focuses on monitoring their progress by first establishing a baseline assessment of language and adaptive skills and then repeating these evaluations periodically to track any changes.
He said the growing interest in leucovorin reflects a broader shift toward more personalized autism treatments, fueled by recent research that supports what clinicians have long observed: autism is not a uniform condition that exists along one continuous spectrum, but rather a collection of distinct conditions that have been grouped under a single label. As a result, different people may require different treatments.
“We don’t yet have enough information to use those findings to guide leucovorin treatment,” Turnacioglu said. “But it’s the kind of direction I’m excited about — figuring out which patients are going to respond to particular treatments.”
An exception
Sohl is part of a team of pediatricians who helped draft the AAP guidelines.
The patients that have approached her are all ages and across the spectrum, including adults and individuals with strong verbal skills. For months, she’d explained her reasons for holding back on leucovorin, and most families accepted them.
Then, in October, a patient sat across from her and she began to wonder if this might be an exception.
He was a teen boy she describes as minimally speaking, whom Sohl had been treating for 10 years. She was impressed by his knowledge of the research on leucovorin, his deep and realistic understanding of the potential risks and benefits, and his eagerness to document any changes both quantitatively and in narrative form. Sohl will be meeting with her patient each month to go over any changes.
“I have low expectations, his mom has low expectations, he has low expectations. But we all agreed it was worth a therapeutic trial,” Sohl said.
With the recent national attention, information about leucovorin has been spreading online far faster than through the slow, methodical channels of medical research, where studies and peer-reviewed papers can take years to emerge. She learns from the parents and patients who are often the first to encounter new ideas circulating in their communities and online.
Sohl tells families that while the drug has shown very little in the realm of side effects, this is in the context of adults with cancer, not children with autism. She said she emphasizes that she does not think this is a dangerous medicine, but there has not been enough research.
“I think it’s my duty as a doctor to say that I don’t know,” Sohl said, “and I want you to know I don’t know.”
At first, the mental health-related videos that popped up on Amy Russell’s TikTok feed made her feel seen. The tips and funny anecdotesabout living with ADHDreminded her of herself — maybe her forgetfulness wasn’t a flaw but a symptom.
After two years of learning about the condition on TikTok, she went to a doctor for an assessment. The resulting diagnosis changed her life for the better, she said, as she started taking medication and using strategies to manage daily tasks. She attributes the transformation in part to TikTok.
There’s just one problem: Now she can’t get the ADHD videos off her feed. The more she scrolls, the stranger and less trustworthy the content becomes, she said. Her efforts to see less of it — scrolling past videos and not engaging — don’t seem to help.
“You just keep finding more tunnels and it gets harder to find your way out,” Russell, 35, said.
She’s not imagining it. TikTok’s algorithm favorsmental health content over many other topics, including politics, cats, and Taylor Swift, according to a Washington Post analysis ofnearly 900 U.S. TikTok users who shared their viewing histories. The analysis found that mental health content is “stickier” than many other videos: It’s easier to spawn more of it after watching with a video, and harder to get it out of your feed afterward.
“It felt like a rabbit hole to me because you kept going down deeper and deeper,” Russell said.
TikTok uses an algorithm to select a video and gives users two main options: Watch it or skip past to something else. Along the way, the app learnswhat a user like Russell likes and dislikes, based on her watching and skipping behavior. It takes skipping past 1.3 videos, on average, to undo the effect of watching one full video about cats or politics, The Post analysis found. For mental health, it takes 2.2 skips — meaning users must work harder to get it out of their feeds.
TikTok spokesperson Mahsau Cullinane criticized The Post’s methodology as incomplete and said it doesn’t “reflect the reality of how our recommendation system works.”
This finding comes amid a broader debate on the role of algorithms and influencers in Americans’ understanding of mental health. Content about mental illness and neurological differences is extremely popular across social media apps, with about as many TikTok posts using the hashtag #mentalhealth as those that mention #sports, according to data from analytics firm Sprout Social. Mental health content on TikTok deals with not just conditions like depression or anxiety, but also living with a neurological type such as ADHD or autism.
People are turning to social media for health information as Americans face a shortage of mental health professionals, barriers to accessing and paying for care, and lingering stigma. Information from social media helps underserved and underdiagnosed populations better understand themselves, many users say. What happens next, however, is rarely examined.
Over the period that The Post examined Russell’s TikTok data, about one in 11 videos on her feed were mental-health-related. Russell, who spent more than an hour watching videos on many days, said the more she scrolled, the more often she saw videos from nonprofessionals that seemed designed to get a reaction rather than educate.
Efforts to evaluate mental health content on TikTok support Russell’s impression.Anthony Yeung, a psychiatrist and University of British Columbia researcher, ran a study examining 100 top TikTok videos about ADHD and found that some were helpful, but about half were misleading. (Videos about creators’ personal experiences weren’t classified as misleading.) Other reviews of TikTok content about ADHD and autism by mental health practitioners have found similar results.
“The algorithm says, ‘Well, you like this video about ADHD, even though it’s misleading, let’s give you another video,’” Yeung said. “And it becomes this very vicious feedback loop of misinformation.”
The phenomenon is having a profound effect on real-world mental health treatment, clinicians say. Yeung said he deals with “two visions of what ADHD is”: the one discussed on social media and the one he sees among actual patients. On TikTok, ADHD content often paints with a broad brush, portraying common quirks or struggles as not just personal experiences but diagnostic criteria for the condition.
One popular ADHD account, @lifeactuator, regularly earns views in the millions with titles like “What ADHD feels like” and “Things people with ADHD do despite knowing better.”One widely watched video with the caption “if the world was made for ADHD” depicts a Costco store with ADHD shoppers being chased around by store employees to stop them from making impulse purchases.
Eric Whittington, the Arizona-based creator behind @lifeactuator, said that because of the constraints of short-form video, he’s not able to include all the information viewers might need to understand what, if anything, his videos reflect about ADHD as an actual medical condition. Taken individually, his videos probably apply to a broad swath of the population, he said — not just people with ADHD.
“When you only have a minute to work with, it’s hard to add disclaimers on the content saying, ‘Yes, everybody experiences this from time to time, but if it happens all the time, you may have ADHD,’ ” he said.
Rana Coniglio, an Arizona-based therapist who works primarily with Gen Z clients, said they often arrive at her practice already attached to a diagnosis they found on TikTok. Sometimes, that attachment makes it harder to accurately diagnose or make a treatment plan that could improve that person’s symptoms.
“I have had people come to me and say, ‘Hey, I saw this video on TikTok and it’s actually the reason that I’m seeking therapy because it made me think I actually do need help,’ and there are benefits to that,” she said. “But I think the majority of people see a diagnosis, take it and run with it.”
High volume, low quality
For Ace Bannon, a 19-year-old in Utah, the more he watched, the darker the content became.
Bannon first got curious about autism and its characteristics after learning that many of his best friends — people he’d met on a Discord server — were autistic. He started watching TikTok videos, with content about autism taking up a growing chunk of his feed. Then, TikTok served him video after video of autistic adults discussing the trauma they endured as children, Bannon said. Before long, he wanted his old algorithm back.
“Because you’re interested, it starts recommending more of those videos and it makes you fall into these rabbit holes that you just want to get out of after a while, but you can’t.”
Sometimes this experience actually exacerbates existing mental health problems, some users say. Kailey Stephen-Lane, 30, said she had to temporarily stop using the app because spending time on TikTok was worsening the symptoms of her obsessive compulsive disorder. While her real-life therapist was helping her sit with fears and insecurities without fixating, TikTok was “bombarding” her with videos about the very symptoms that made her so anxious, she said.
“The TikToks that I’ve been getting are not helpful to my recovery,” she said. “They lead me down a lot of spirals, and me just clicking ‘not interested’ doesn’t seem to work anymore.“
TikTok provides a high-level description of some of the data its algorithm uses but few details. That makes it difficult to know why mental health videos are stickier than other topics, says Stevie Chancellor, an engineering professor at the University of Minnesota who studies AI and its risks, and whose research found that the algorithm creates a “runaway train” of mental health content.
But the app’s business incentives offer some clues, Chancellor says. Maybe users who see a lot of mental health videos spend longer on the platform or are more likely to spend money down the line, she said. Maybe the effect is completely unintentional, an example of a black-box algorithm optimizing for what it thinks users want.
“Watching [mental health] content might lead to other behaviors that are valuable on the platform,” Chancellor said.
The topic may become sticky because it’s one “that a user only wants to engage with sometimes,” said Laura Edelson, a computer science professor at Northeastern University who collaborated with The Post in a parallel TikTok research effort.
Cullinane, the TikTok spokesperson, said the company is “transparent” about how its feed works.
For TikTok users, adjusting the type of content that shows up on their feeds can be hard. It’s not always clear when engaging with a certain video would spawn something undesirable: Even watching clips about romantic relationships made a user more likely to encounter mental health content, The Post’s analysis found. TikTok has gradually added options that could help users tailor their feeds, such as clicking a “not interested” button, blocking videos with certain keywords or resetting their algorithms from scratch. A new “Manage Topics” menu lets users adjust the prevalence of 12 specific topics on their For You page — but mental health isn’t one of them.
As for Russell, she is glad for the journey toward an ADHD diagnosis because of TikTok. She just wishes her favorite type of content — lighthearted cat videos — got the same treatment from the app’s algorithm.
“I want like 10-20% cute cat videos, probably even like 30%,” she said. “But those disappear really quickly.”
Methodology
Hundreds of TikTok users in the United States sent their watch history data to The Washington Post. We downloaded the collective 14.8 million videos they’d been shown and then sorted them into topics, based on keywords in the transcripts and on-screen text. The Post calculated the stickiness of each topic by computing the difference between the number of topical mental health videos each user had been shown in the previous 50 videos and how many they saw in the next 50. We averaged this for all videos, aggregated by whether the user watched at least 90% of the video, or skipped it.
Capstan Therapeutics’ sale this year for $2.1 billion, the highest price paid for a private early-stage biotech company since 2022, was a triumph for its founders at the University of Pennsylvania.
Unfortunately for Philadelphia, the company is based in San Diego. Investors wanted an executive who lives there to be CEO.
Capstan was a miss for Philadelphia, said Jeffrey Marrazzo, who cofounded a high-profile regional biotech company, Spark Therapeutics, and is now an industry investor and consultant.
If Philadelphia had a bigger talent pool of biotech CEOs, “it would have and should have been here,” he said.
The Philadelphia region has lagged behind other biotech centers in landing companies and jobs, but industry experts are working to close the gap and better compete with Boston, the San Francisco Bay Area, and San Diego.
According to Marrazzo and others, the Philadelphia region’s relatively shallow pool of top biotech management is a key challenge.
Big investors go to managers who have proven ability to deliver big investment returns, said Fred Vogt, interim CEO of Iovance Biotherapeutics, a California company with a manufacturing facility in the Navy Yard.
“They want the company to perform. They’ll put it in Antarctica, if that was where the performance would come from,” he said.
The Lilly announcement last month also reflects Philadelphia’s national biotech stature. It’s the fourth U.S. city to get a Lilly Gateway Lab, behind Boston, the San Francisco Bay Area, and San Diego.
Those places have far outpaced Philadelphia in the creation of biotech research and development jobs, even as the sector’s growth has slowed.
From 2014 through last year, the Boston area added four biotech research and development jobs for every one job added here, according to an Inquirer analysis of federal employment data.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Penn’s role in Philadelphia biotech
Philadelphia’s reputation as an innovation center — boosters like to call the region “Cellicon Valley” — starts with the University of Pennsylvania, which has long been a top recipient of National Institutes of Health grants to advance scientific discovery.
Research at Penn has contributed to the creation of 45 FDA-approved treatments since 2013, according to the university.
“Penn discoveries help spark new biotech companies, but we can’t build the whole ecosystem in this area alone,” said John Swartley, Penn’s chief innovation officer. “Great science is just one ingredient. We also need capital, experienced leadership, real estate and manufacturing infrastructure, and strong city and state support.”
Penn was one of two Philadelphia institutions receiving more than $100 million in NIH funding in the year that ended Sept. 30. The otherwas the Children’s Hospital of Philadelphia.
Katalin Karikó and Drew Weissman spoke at a University of Pennsylvania news conference after they were named winners of a 2023 Nobel Prize in medicine. Their work was instrumental to modifying mRNA for therapeutic uses, such as the rapid development of lifesaving vaccines during the COVID-19 pandemic.
By contrast, the Boston area was home to 10 institutions with at least $100 million in NIH grants, generating more spinoffs and jobs.
The Philadelphia region has a healthy number of biotech spinouts, but the biggest markets have more from a larger number of research institutions, said Robert Adelson, founder Osage University Partners, a venture capital firm in Bala Cynwyd.
That concentration of jobs and companies in the Boston area — where nearly 60,000 people worked in biotech R&D last year — makes it easier to attract people. By comparison, there were 13,800 such jobs in Philadelphia and Montgomery County, home to the bulk of the regional sector.
If a startup fails, which happens commonly in biotech, “there’ll be another startup or another company for me to go to” in a place like Boston, said Matt Cohen, a managing partner for life science at Osage.
Another challenge for Philadelphia: It specializes in cell and gene therapy, a relatively small segment of the biotech industry, whose allure to investors has faded in the last few years.
Such market forces shaped the trajectory of Spark, a 2013 Children’s Hospital of Philadelphia spinout that developed Luxterna, the first FDA-approved gene therapy, used to treat an inherited form of blindness. The promise of Spark’s gene therapy work for a form of hemophilia spurred its 2019 acquisition by Swiss pharmaceutical titan Roche for $4.8 billion.
The company still employs about 300 in the city, a spokesperson said, and work continues on its $575 million Gene Therapy Innovation Center at 30th and Chestnut Streets in University City.
The long arc of biotech
A handful of companies dominated the early days of U.S. biotech. Boston had Biogen and Genzyme, San Francisco had Genentech, San Diego had Hybritech, and Philadelphia had Centocor. All of them started between 1976 and 1981.
Centocor started in the University City Science Center because one of its founders, virologist Hilary Koprowski, was the longtime director of the Wistar Institute. Centocor’s first CEO, Hubert Schoemaker, moved here from the Boston area, where he had gotten his doctorate at the Massachusetts Institute of Technology.
Another drug still under development at the time of the sale, Stelara, went on to become J&J’s top-selling drug as recently as 2023 with $10.9 billion in revenue. Stelara, approved to treat several autoimmune disorders, remains a testament to Centocor’s legacy.
Despite its product success, Centocor didn’t have the same flywheel effect of creating new companies and a pipeline of CEOs as peer companies did in regions outside of Philadelphia.
The University of Pennsylvania’s Smilow Center for Translational Research, shown in 2020, is one of the school’s major laboratory buildings.
“There are a lot of alums of Centocor that are really impressive, but they seem to have wound up elsewhere,” said Bill Holodnak, CEO and founder of Occam Global, a New York life science executive recruitment firm.
Among the Centocor executives who left the region was Harvey Berger, Centocor’s head of research and development from 1986 to 1991. He started a new company in Cambridge, Mass.
At the time, the Philadelphia area didn’t have the infrastructure, range of scientists, or management talent needed for biotech startups, he said.
Since then, he thinks the regional market has matured.
“Now, there’s nothing holding the Philadelphia ecosystem back. The universities, obviously Penn, and others have figured this out,” Berger said.
Conditions have changed
Penn’s strategy for helping faculty members commercialize their inventions has evolved significantly over the last 15 years.
It previously licensed the rights to develop its research to companies outside of the area, such as Jim Wilson’s gene therapy discoveries and biochemist Katalin Karikó and immunologist Drew Weissman’s mRNA patents. Now it takes a more active role in creating companies.
Among Penn’s latest spinouts is Dispatch Bio, which came out of stealth mode earlier this year after raising $216 million from investors led by Chicago-based Arch Venture Partners and San Francisco-based Parker Institute for Cancer Immunotherapy.
Dispatch, chaired by Marrazzo, is developing a cell therapy approach that uses a virus to attach what it calls a “flare” onto the cells it wants the immune system to attack.
Marrazzo said in July that he wasn’t going to be involved in Dispatch if it wasn’t based largely in Philadelphia. As of July, 75% of its 60 employees were working in Philadelphia. Still, Dispatch’s CEO is in the San Francisco Bay Area.
The Philadelphia region is increasingly well-positioned for the current biotech era, said Audrey Greenberg, who played a key role in launching King of Prussia’s Center for Breakthrough Medicines about five years ago. The center is a contract developer and manufacturer for cell and gene therapies.
“You no longer need to move to Kendall Square to get a company funded,” she said, referring to Cambridge’s biotech epicenter. “You need good data, a credible translational plan, experienced advisers, and access to patient capital, all of which can increasingly be built here.”
Greenberg now works as a venture partner for the Mayo Clinic, with the goal of commercializing research discoveries within the health system’s network of hospitals in Minnesota, Arizona, and Florida.
She plans to bring that biotech business to the Philadelphia region.
“I’m going to be starting my companies all here in Philadelphia, because that’s where I am. And I know everybody here, and everybody I’m going to hire in these startups that are going to be based here,” she said.
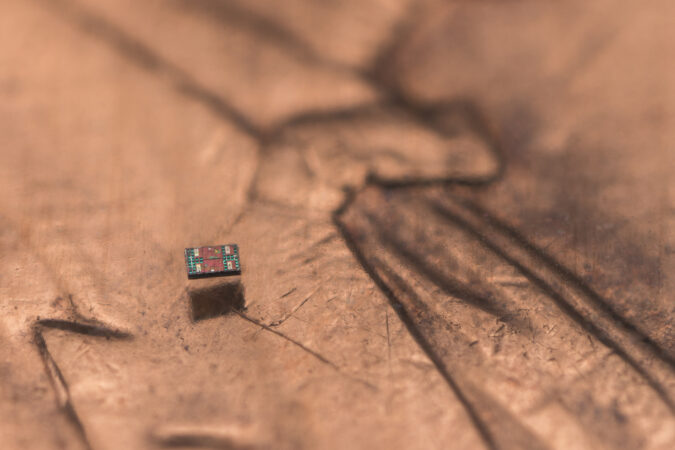
Solving a technical challenge that has stymied science for 40 years, researchers have built a robot with an onboard computer, sensors, and a motor, the whole assembly less than1 millimeter in size — smaller than a grain of salt.
The feat, accomplished by a partnership of researchers at University of Pennsylvania and University of Michigan, advances medicine toward a future that might see tiny robots sent into the human body to rewire damaged nerves, deliver medicines to precise areas, and determine the health of a patient’s cells without surgery.
“It’s the first tiny robot to be able to sense, think, and act,” said Marc Miskin, assistant professor of electrical and systems engineering at University of Pennsylvania, and an author of a paper describing the work published this week in the journal Science Robotics.
The device, billed as the world’s smallest robot able to make decisions for itself, represents a major step toward a goal once rooted in science fiction. In the 1960s, the story and movie Fantastic Voyage imagined a medical team placed aboard a submarine and shrunk to the size of a microbe. The microscopic medical crew was then injected into the body of a dying man in order to destroy an inoperable blood clot.
“In the future, let’s say 100 years, anything a surgeon does today, we’d love to do with a robot,” said David Gracias, a professor in the department of chemical and biomolecular engineering at Johns Hopkins University who was not involved in the study. “We are not there yet.”
In 1989, two decades after Fantastic Voyage, Rodney A. Brooks and Anita M. Flynn, scientists at the Massachusetts Institute of Technology, wrote a paper called, “Fast, Cheap, and Out of Control: A Robot Invasion of the Solar System,” that described a robot they’d built measuring just 1¼ cubic inches, dubbed Squirt.
Sawyer Fuller, an associate professor of mechanical engineering at the University of Washington, said that when “Fast, Cheap, and Out of Control,” was published, “people thought microrobotics was coming any minute now. … Turns out it has taken a little longer than expected to put all these things together.”
Fuller, who was not involved in building the new microrobot, called it “the vanguard of a new class of device.”
Miskin said the microrobot built by the Michigan and Pennsylvania teams is about 1/100th the size of MIT’s Squirt but isn’t ready for biomedical use.
“It would not surprise me if in 10 years, we would have real uses for this type of robot,” said David Blaauw, a co-author of the paper in Science Robotics and professor of electrical engineering and computer science at University of Michigan.
For decades scientists have dreamed of buildinga microrobot less than 1 millimeter in size, a barrier that corresponds to the smallest units of our biology, Miskin said. “Every living thing is basically a giant composite of 100-micron robots, and if you think about that it’s quite profound that nature has singled out this one size as being how it wanted to organize life.”
For comparison, a human hair has a diameter of about 70 microns, while human cells are about 20 to 40 microns across.
Although scientists and engineers have been miniaturizing circuits for the last half-century, the challenge has been to shrink all of the parts needed for a computer-guided microrobot, then assemble themwithout damaging the parts or causing them to interfere with one another. The robot needs an energy source of sufficient power to operate the computer and move the robot.
Five years ago, Miskin, whose specialty has been building microrobots, met Blaauw when the two gave back-to-back talks. Blaauw’s lab then held ― and still holds ― the distinction of having built the world’s smallest computer.
“Even in the presentations we were like, ‘Oh, we need to talk to each other,’” Blaauw recalled.
The device they built uses tiny solar cells that convert light into energy. Some of that energy powers the computer, and some propels the robot as it swims through liquid. The computer runs at about one-thousandth the speed of today’s laptops and has far less memory.
In the lab, the scientists shone an LED light down into the lab dish that contained the robot in a solution. The robot is made of the same kinds of materials found in a microchip: silicon, platinum, and titanium.
To protect it from the effects of fluids, the microrobot is encased in a thick layer of what is essentially glass, Miskin said. There are a few holes in the glass that are filled in with the metal platinum, forming the electrodes that provide electrical access.
At Johns Hopkins, Gracias stressed that scientists need to ensure that the materials they use for microrobots can be safely used inside a human body.
Sensors on the robot allow it to respond to different temperatures in liquid. To move, the device uses energy from the solar panels to charge two metal electrodes on either side of it. The electrodes attract oppositely charged particles in the water, generating a flow that pulls the robot along.
As it swims, the robot communicates with the person operating it.
“We can send messages down to it telling it what we want it to do,” using a laptop, Miskin said, “and it can send messages back up to us to tell us what it saw and what it was doing.”
The robot communicates using movements inspired by the waggle dance honeybees use to communicate.
During the summer, the scientists invited a group of high school students to come in and test the new microrobots. The students were able to track the movements of the robots using a special low-cost microscope.
“They loved it,” said Miskin. “It was definitely a little bit challenging at first, just getting oriented to working with something that small. But that’s part of the appeal. Once they got the hang of it, they were all in.” Miskin said the version of the robot the students used cost only about $10.
Researchers are working now to develop the microrobot so that it can work in saltwater, on land, and in other environments.
The long-term vision, Blaauw said, is to design tiny computers that can not only talk back and forth to their operators.
“So the next holy grail really is for them to communicate with each other,” he said.
The 10-year-old boy who was severely burned in the Northeast Philadelphia plane crashwas headed home on Tuesday after spending nearly a year in the hospital, his grandmother, Alberta “Amira” Brown said.
“It’s the best thing ever that he’ll be home for the holidays,” Brown said in the morning as the boy prepared to leaveWeisman Children’s rehabilitation hospital in South Jersey. “He is truly happy to be coming home.”
Ramesses Vazquez Viana, then 9, suffered burns to 90% of his body on Jan. 31 whena Learjet medical transport crashed on Cottman Avenue near the Roosevelt Mall, killing allsix people on board.
Ramesses had been riding in a car with his father, Steven Dreuitt Jr., and Dreuitt’s fiancée, Dominique Goods Burke. Dreuitt, 37, died in the blaze. Goods Burke, 34, died in April from her injuries after spending nearly three months at Thomas Jefferson University Hospital.
A bystander saw Ramesses after he escaped from the car; the boy’s back was on fire, and his shirt was burned away.
Police took Ramesses to St. Christopher’s Hospital for Children, and he was later airlifted to Shriners Children’s hospital in Boston. He underwent more than 40 surgeries, including multiple skin grafts. He spent months in physical therapy relearning how to get out of bed, walk and climb stairs, according family interviews with CBS News.
His classmates from Smedley Elementary School in the Philadelphia’s Frankford neighborhood cheered him on from afar, writing him cards and sending videos.
Ramesses celebrated his 10th birthday in October at the Boston hospital.
A few weeks ago, Ramesses was moved closer to his Philadelphia home to Weisman Children’s in Marlton, N.J.
During a phone interview with The Inquirer, Brown said her grandson “has a long road ahead of him” and would need additional surgeries.
During a visit with him Saturday, he kicked a soccer ball around with her.
Brown confirmed a CBS report that Ramesses was being released from Weisman sometime Tuesday, but declined to provide specifics.
Brown said her grandson has chilling memoriesfrom that night: He was in the car’s backseat texting with Brown at about 6 p.m. when the plane exploded in a giant fireball, and he heard loud booms.
As flames engulfed the car, Ramesses tried to help his father, who couldn’t move his legs. The child heard his father yell to get out, and that he loved him. Ramesses told his father he loved him back. He could hear Goods Burke screaming.
Steven Dreuitt Jr. and Goods Burke shared a teenage son, Dominick Goods, who is now a junior at Imhotep Institute Charter High School. Brown said her older grandson is “really struggling” with his parents’ deaths.
The sixpassengers killedon the medical transport jet were Mexican nationals. They included the pilot and copilot, two medical personnel, an 11-year-old girl, and her mother. The girl was headed home to Mexico after undergoing treatment for a spinal condition at Shriners Children’s Philadelphia.
Investigators with the National Transportation Safety Board haven’t yet determined why the plane crashed. A preliminary report, released earlier this year, found the cockpit voice recorder “had likely not been recording audio for several years.” No distress calls were made by the pilot or copilot.
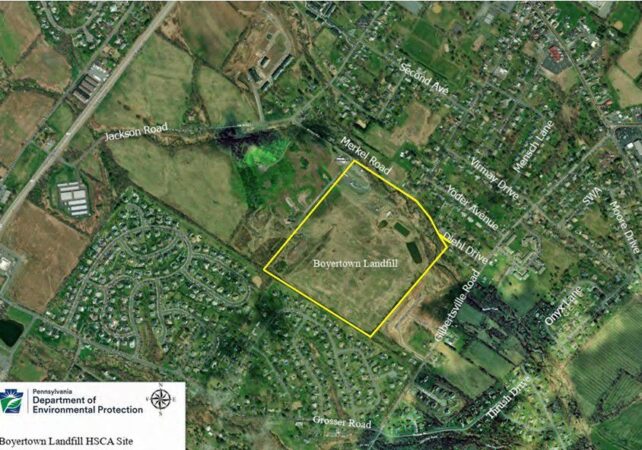
Residential waste, construction and demolition debris, as well as sewage treatment plant sludge, were dumped for decades at the 30-acre Boyertown Sanitary Landfill in northern Montgomery County until it was capped in 1987.
As state and federal officials mull whether to add the landfill to the national Superfund list, a well used by nearby Gilbertsville Elementary School has tested positive for human-made polyfluoroalkyl substances, known as PFAS.
The school is about 3,000 feet from the landfill property border and is within the Boyertown Area School District. Minister Creek passes through the property, and two residential neighborhoods are nearby.
Scott Davidheiser, the district’s superintendent, sent a letter to staff and students’ families Monday alerting them to the test results, which were made known during a Pennsylvania Department of Environmental Protection (DEP) public information session on the landfill on Dec. 10.
Gilbertsville Elementary tested at an annual average of 6.7 parts per trillion (ppt) for PFAS. That falls under acceptable limits by current state standards of 14 ppt.
However, it would exceed federal maximum contaminant level standards of 4 ppt set to go into effect in 2031 if not addressed.
Davidheiser’s letter said the district “remains committed to safety in all areas, including water safety.” The districthas hired Suburban Water Technology Inc. to develop a water safety planto lower annual average PFAS levels to within federal standards.
District officials plan in January to discuss a plan to lower the levels.
<iframe title="Boyertown Sanitary Landfill and PFAS contamination" aria-label="Locator map" id="datawrapper-chart-1kgam" src="https://datawrapper.dwcdn.net/1kgam/1/" scrolling="no" frameborder="0" style="width: 0; min-width: 100% !important; border: none;" height="581" data-window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
What are PFAS?
PFAS are a group of chemicals manufactured by industry for use in consumer products since the 1940s. There are thousands of different PFAS, some of which have been more widely used and studied than others.
Exposure to them hasbeen shown to impact the health of humans and lab animals, but the extent is still being studied.
Standards for maximum acceptable levels of the compounds in drinking water have created confusion in recent years.
The EPA was slow to set standards, so states began setting their own. Pennsylvania set different levels to start in 2024 for various types of PFAS:14 ppt forperfluorooctanoic acid (PFOA) and 18 ppt for perfluorooctane sulfonic acid (PFOS).
However, the EPA, under the Biden administration, then set the first federal standards, which would supersede state standards. The rule said that PFOA and PFOS can’t exceed 4 ppt. And, it set standards for other compounds within the PFAS family. The regulations were set to go into effect in 2027.
However, the EPA, under the Trump administration, rolled back some provisions by announcing it would keep the standards for PFOA and PFOS, but delay enforcement until 2031. And, it said it would reconsider the limits on the other compounds.
As a result, the PFAS level at Gilbertsville Elementary School’s current level would exceed the federal level if not brought down by 2031.
What’s the Boyertown Landfill?
Officials with the state Department of Environmental Protection and U.S. Environmental Protection Agency have been deciding since 2023 whether the Boyertown Landfill, in Douglass Township, should be named a Superfund site after test samples showed PFAS in nearby private wells.
The landfill and surrounding property are owned by the Boyertown Sanitary Disposal Co. It is set on a wider 60-acre parcel at 300 Merkel Roadin Gilbertsville. The property contains raw and pretreated leachate storage lagoons, buildings housing leachate pretreatment facilities, and stormwater management basins and swales.
The unlined landfill stopped accepting solid waste in 1985. It had accepted municipal waste, office trash, and construction debris. It took in significant amounts of municipal sewage treatment plant sludge and industrial waste.
In last week’s informational session, the DEP said water sampling around the area of the landfill in 2024 and 2025 showed multiple locations containing various PFAS compounds.
State officials said they have installed carbon-activated filtration systems in residential wells within a half-mile of the landfill that tested above 4 ppt, according to an account of the meeting in Pottstown’s local newspaper, The Mercury.
The newspaper reported that the DEP, however, will not provide similar assistance to Gilbertsville Elementary School because it is part of a small public water system and is required to remediate contamination.
Once considered the loudest hospital in the Philadelphia area, Riddle Hospital in Media has significantly reduced its nighttime noise levels, newly released federal data shows.
At the Main Line Health Riddle hospital, only 12% of patients from the most recent survey rated the area around their room at night as “sometimes” or “never” quiet — down from 26% of patients surveyed between July 2022 and June 2023.
Across the Philadelphia region, 52% of patients said their hospital room was “always” quiet at night. That’s slightly worse than nationally, where patients said hospitals were quiet throughout their stay 57% of the time.
Virtua Mount Holly Hospital in New Jersey is now rated the loudest by patients.
Nazareth Hospital in Northeast Philadelphia, owned by Trinity Health, was ranked the second loudest in the region.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Quieter hospitals have benefits for both patients and staff, helping to lower anxiety levels, improve sleep quality, and ease the flow of communication.
Riddle Hospital’s improvement follows construction of a new 230,000-square-foot patient pavilion that had temporarily increased noise at its Delaware County campus.
“With the pavilion’s 2023 completion, as well as the resulting addition of more private rooms, noise is significantly reduced,” spokesperson Larry Hanover said.
Reducing noise is also priority for Penn Medicine, whose Hospital of the University of Pennsylvania (HUP) was rated the quietest hospital among the 25,000 patients surveyed in the Philly-area.
Chester County Hospital, also owned by Penn Medicine, was ranked the second quietest.
The health system has made big investments in recent years to address noise levels at its hospitals, according to the university’s website. The Pavilion, which opened at HUP in Center City in 2021, was designed to reduce noise levels and nightly disruptions by separating nonclinical work from patient care areas.
Each floor of the $1.6 billion building centers around an “offstage” area for staff to hold conversations and calls away from patient rooms that line the perimeter. The design of the rooms also allows care teams to check vitals and refill medications from the hallway, reducing nighttime disruptions.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
The University of Pennsylvania launched a fund backed by $10 million from the university to make seed investments in companies founded by Penn researchers, officials announced Monday.
The fund, called StartUP, will invest up to $250,000 in companies founded by Penn researchers and based on innovations created at the university. Any profits will be put back into the fund, Penn said.
“This new fund addresses the critical need for seed investment capital at the earliest stages of company formation and will further accelerate innovation across the university,” Penn’s vice provost for research, David Meaney, said in a statement. Meaney is on the faculty at Penn’s School of Engineering and Applied Science.
The university’s Office of the Chief Innovation Officer will manage the fund. The innovation office will evaluate applicants with the help of external advisers. Factors in investment decisions include overall feasibility and commercial potential.
The new investment fund builds on efforts already underway at the Penn Center for Innovation, the Wharton School, and Penn Medicine, which in 2018 started a fund to invest $50 million in biotech companies.
Penn has led the nation recently in licensing revenue from faculty inventions, thanks largely to revenue from COVID-19 vaccines that were based on mRNA technology developed 20 years ago by Penn researchers Drew Weissman and Katalin Karikó.
The human brain hasfour distinct turning points where its structure changes, according to a study published in the journal Nature Communications, demonstrating that brain development is not as linear as you might think.
“It’s easy to fall into this belief that there’s a ‘good’ or ‘bad’ way for a brain to be structured,” said lead study author Alexa Mousley at the University of Cambridge. “And that’s not really the case. What this study is emphasizing is the brain is expected to be doing something different at different ages.”
In the new study, Mousley and colleagues looked at around 4,000 scans from healthy people ages 0 to 90 and analyzed their brains. They found four major times when the brain underwent developmental changes, around ages 9, 32, 66, and 83, dividing the life span into five distinct phases.
“It’s yet another very nice example of how the brain and its global interactions change across the life span,” said Seth Grant, a neuroscientist at The University of Edinburgh who wasn’t involved in the new research. “The message is, there is continuous change from birth until old age. It’s not as if you suddenly build a brain and it stays the same and then just drops off at old age. It’s always changing.”
Mousley and her co-authors identified five epochs during which the brain is wired in different ways.
1. Childhood
From infancy to 9 years old, the brain is busy. There is a lot of consolidation of neural connections happening, competitive elimination of synapses, and rapid increases in gray and white matter. But interestingly the brain is becoming less efficient during this time — so it takes longer for information to get from one region of the brain to another. The researchers don’t fully understand why this would be the pattern, but they have some theories.
“We know that in very early life, the brain makes more connections than it needs, and then it prunes them away,” Mousley said. “It’s unclear if that is kind of what’s happening here, but it is potentially what’s happening.”
Whatever the reason for the brain becoming less efficient during childhood, it is a time when a lot of learning happens — language, motor skills, speech — and there is likely a reason that the brain is structured the way that it is during this period.
“It could be that this decreasing efficiency is potentially related to this incredible moment of learning,” Mousley said.
2. Adolescence
There is a dramatic turning point that the researchers saw occurring around the age of 9 on average — a time when many children begin to enter puberty. The brain switches gears and starts rewiring to become more efficient.
The adolescence phase the researchers identified lasts for two decades, into the early 30s on average. This is when people are most vulnerable to developing a mental health disorder, but it’s also a critical time for braindevelopment.
“It is really important to think about adolescence as this protracted window,” said Katie Insel, a psychologist at Northwestern University who studies how the brain changes over the course of adolescence. She said that while in our society we may think of 18- or 21-year-olds as adults, this research adds to a growing body of work suggesting that the brain isn’t fully developed or stable until our late 20s or even early 30s.
“Something that sets us apart as humans from other animals is how slowly we develop,” Mousley said. “A giraffe can stand up very soon after being born, but human babies just take a very long time to learn to walk, to eat.”
Mousley suggested that this slower development might give humans the opportunity to develop more complex brain connections, and could be related to the things that humans can do that other animals can’t.
3. Adulthood
Adulthood is the longest phase — lasting for more than three decades from around 32 years old until around 66 years old.
“It does seem to be this kind of period of relative stability,” Mousley said. “It’s consistent for a very long period of time.”
That doesn’t mean that the brain isn’t changing during this period, but the changes are less dramatic than during other phases. This is also a period of stability in terms of intelligence, behavior, and personality.
“If you just think about what an adult is compared to a teenager, you kind of assume there’s kind of a level of stability there in terms of how people are behaving. And that’s aligning with this three-decade period of consistent brain rewiring from our study,” Mousley said.
4. Early aging
Around 66 years old on average, the researchers saw another turning point. This is a time when the brain seems to become more vulnerable to age-related diseases — but the news isn’t all bad for the aging brain.
“There’s an expected and healthy, typical way for the brain to shift,” Mousley said.
Insel noted that in addition to some of the negative changes people might associate with aging, like memory loss, there are also positive changes. Older adults tend to be wiser and better at emotional regulation.
“There are pros and cons to every developmental stage,” Insel said. “I think with every phase of life, there are trade-offs where some types of cognition and behavior are privileged because of how the brain is responding to the environment.”
5. Late aging
From 83 onward, the researchers identified a “late aging” phase.
“What we’re seeing during that late aging phase is something called ‘increasing centrality,’” Mousley said. Particular regions of the brain become more important than others during this time. There is reduced connectivity, but there seems to be a pattern to that change.
The metaphor Mousley used was that of changing bus routes. If you had a direct bus to work, but one day it stopped running and you had to take two buses, the transfer station would suddenly become very important. She theorized that the brain might be prioritizing important connections if other connections drop off.
What it means
The word “development” is often associated with childhood or the teenage years — but what this new research demonstrates is that the brain develops continually throughout our lives.
“We often ascribe certain brain changes to negative outcomes in adulthood or later life,” Insel said. “But actually there’s certain cognitive features that can be really helpful and useful in aging.” By zooming out and looking at how the brain changes over the course of our lifetimes, Insel hopes that we can have a better understanding of what to expect at these different ages, and why our brains might be more vulnerable to certain disorders in adolescence or older age respectively.
Yaakov Stern, a neuroscientist at Columbia University, noted that a good next step would be to try to understand exactly how these measures of the brain might be related to cognitive processes — essentially connecting the dots between this research and other work that has looked at the way our brains function throughout our lives.
He added that many of the things that affect brain development are within our control — such as diet, exercise and social connection.
“The brain changes with aging. We know that,” Stern said. “What interests me, is there are exposures that seem to be associated with more successful aging.”