Amid a historic drop in violent crime, homicides have fallen to lows not seen in decades. But in what researchers say is an alarming trend, homicides related to domestic violence are on the rise.
There were 37 such killings in Philadelphia last year, up from 28 the previous year. And even as homicides have fallen sharply overall, domestic killings remain stubbornly intractable. In all, deaths related to domestic violence accounted for about one in six homicides in the city last year, records show.
To address that, the police department is adding specialized training for officers and others who deal with victims of such crimes and adding staff in its Office of Community Advocacy and Engagement. When the unit expands this spring, staffers will be trained to spot signs of domestic abuse and advocate for victims of intimate partner violence, among other crimes.
That work mirrors efforts in cities such as New York, which launched a new police unit last year dedicated to combating the surge in domestic violence as such crimes rise nationwide.
“The numbers are moving in the wrong direction,” said Marian Braccia, a professor at Temple University’s Beasley School of Law and a former prosecutor in the district attorney’s family violence and sexual assault unit. “It’s terrifying.”
In Philadelphia last year, the slaying of Kada Scott drew attention to the issue after The Inquirer reported that her accused killer, Keon King, had previously been accused of stalking and kidnapping another woman. But two criminal cases against him fell apart when the victim failed to appear in court and prosecutors withdrew the charges.
And last month, calls for awareness surrounding domestic violence were renewed when Yuan Yuan Lu, 28, was killed one day after reporting that her ex-boyfriend had sexually assaulted her in his Pennsport home. Police say 32-year-old Yujun Ren followed Lu to her Levittown home and shot her in the head, killing her.
According to prosecutors, Lu told police the day before she was killed that Ren carried a gun and she feared for her safety.
Philadelphia’s new unit would work to support victims in just such circumstances, officials said. The office launched last spring with 10 victim advocates with backgrounds in social work and behavioral health.
In March, those staffers will begin working with victims of sexual assault and domestic violence, said Ayanna Greene-Davis, executive director of the Office of Community Advocacy and Engagement.
And the unit will add 10 more members — sworn police officers with law enforcement experience — who will complete similar victim-oriented training, she said.
Ayanna Greene-Davis, 47, Executive Director for Office of Community Advocacy and Engagement, of Northwest Philadelphia, Pa., poses for a portrait at the Philadelphia Police Headquarters in Philadelphia, Pa., on Tuesday, Feb. 17, 2026. .
“We’re not going to take days and days and days” to respond to reports of domestic violence, Greene-Davis said. “In the past, that happened.”
Victims of such crimes will be able to call the office’s advocates to voice concerns about their cases as they are investigated, according to Greene-Davis. And advocates will be trained to connect them with resources such as domestic abuse shelters and provide information on ways to remove themselves from dangerous living situations.
The unit will also oversee a broader effort to train patrol officers throughout the department to better assess the dangers victims of domestic violence face and work to keep them safe.
“Every victim is going to be in a different stage, but we can talk to them,” Greene-Davis said. “We can provide a safety plan.”
“Why would you not want to study the thing that lets you study,” said Schechtman-Taylor, a senior from New York City. “The brain, that’s our entire world.”
Neuroscience has become the most popular major on the highly selective liberal arts campus on Philadelphia’s Main Line, counting nearby Bryn Mawr College students who also take classes at Haverford. And it’s only been around since 2021 when the two colleges — which have had a minor in the discipline since 2013 — decided to administer the joint major.
At Haverford, there were 24 majors the year it started; now there are 60. Bryn Mawr saw similar growth and currently has 49. Enrollment in Haverford’s neuroscience classes including both Bryn Mawr and Haverford students grew from 154 in 2014 to nearly 800 last fall.
“We knew that neuroscience was going to be popular, but we did not anticipate this growth,” said Helen White, Haverford’s provost, who noted the school recently hired another neuroscience professor to accommodate more students.
The major’s popularity is also growing at schools around the Philadelphia region — and across the country. Students and professors say neuroscience is popular because it’s interdisciplinary, involving psychology, biology, and chemistry, and can lead to a variety of careers. It can also be personal, because it involves studying diseases like Alzheimer’s and Parkinson’s, which have no cures, and the treatment of strokes and traumatic brain injuries.
“I would say about 90% of my students are coming into my lab because they have someone in their family with one of these diseases,” said Rob Fairman, a Haverford biology professor whose research focuses on neuroscience.
Haverford senior Alina Schechtman-Taylor, 21, of New York City, works as a teacher assistant in professor Laura Been’s lab.
A growing major
In 2008, 110 colleges nationally offered neuroscience majors; now, it’s about 330, said Raddy Ramos, associate professor in the Department of Biomedical Sciences at the New York Institute of Technology. Ramos, who coauthored studies on the topic, said there were more than 2,000 neuroscience graduates in 2008; in 2019, that number had grown to more than 7,200.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Pennsylvania is a hot spot, with 36 colleges having programs in 2022-23, Ramos said — more than than any other state.
Drexel University, which has had a minor since 2015, launched its undergraduate major in neuroscience in 2024.
“We have seen a 45% increase in applications over the last two years,” a university spokesperson said.
Pennsylvania State University in November announced it was launching two new undergraduate majors in neuroscience, one offered by the biology department and the other by the biobehavioral health department.
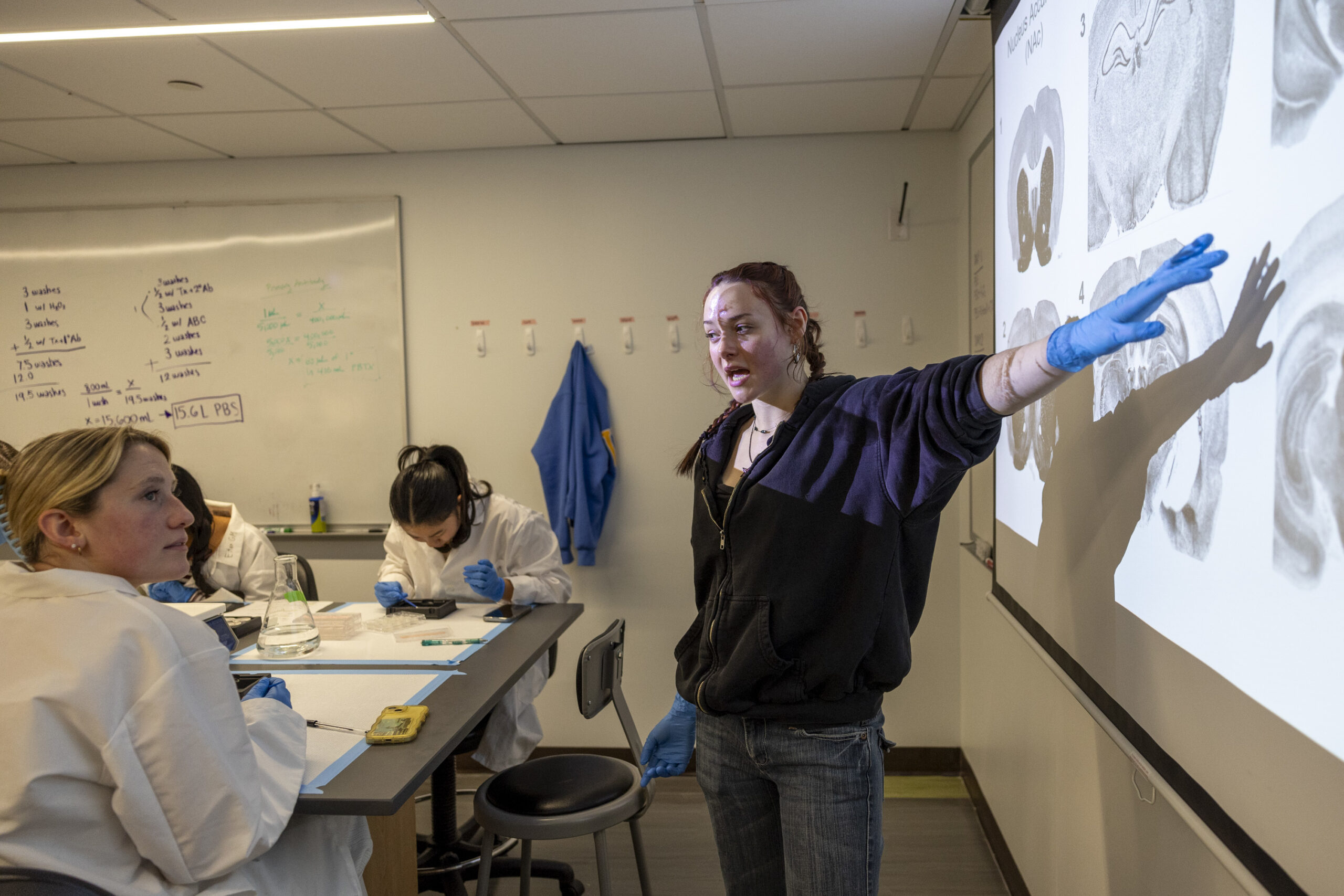
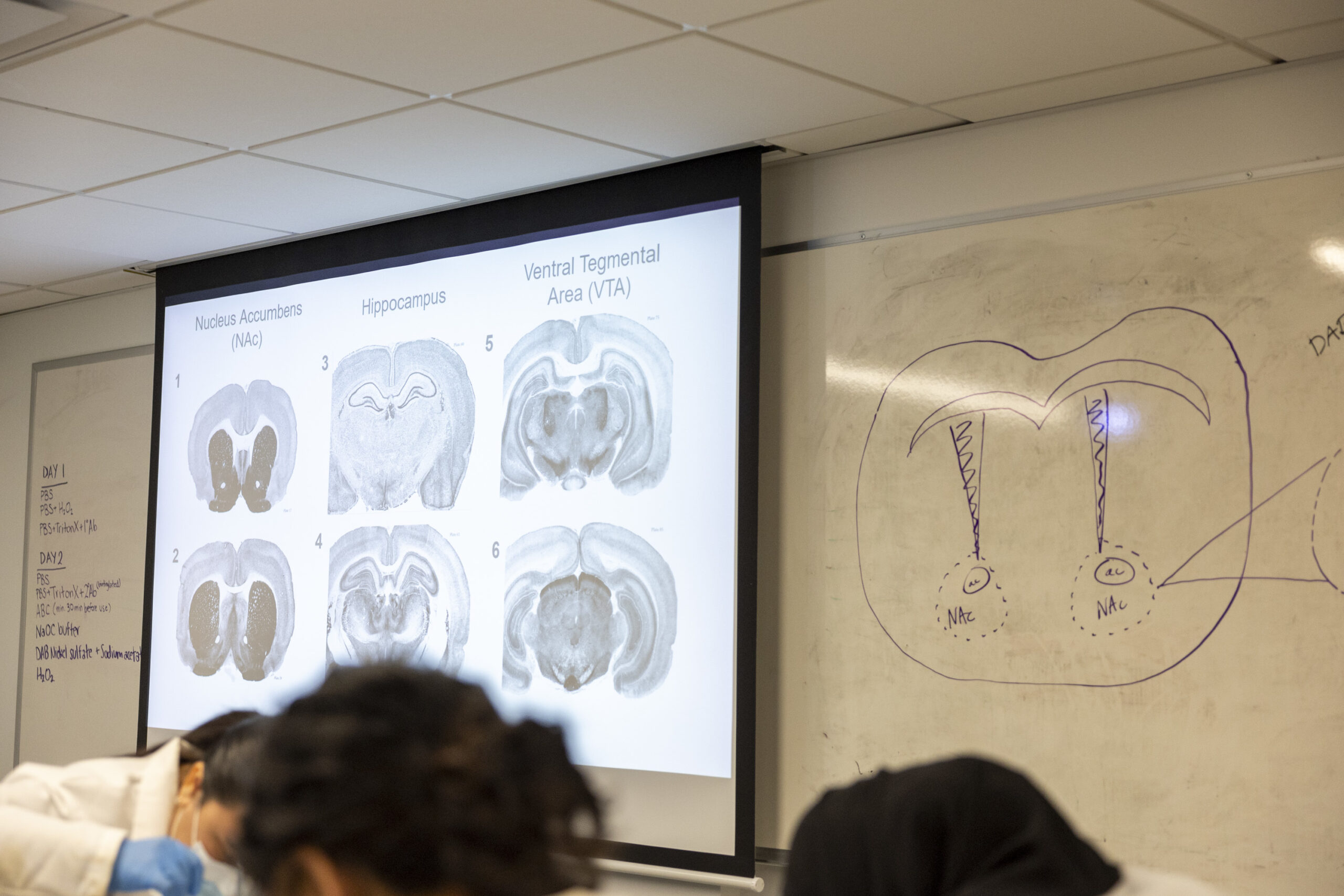
Students look for sections of rat brains that match the sections projected on the screen in a Haverford College lab.
Neuroscience has become especially popular among pre-med majors, school officials say. Otherpotential career paths include biotechnology, pharmacology, psychology, and neuroengineering, while somestudents go on to law school, business, or public policy.
“There’s a lot more awareness that mental health conditions are due to changes in the brain, and people want to understand that,” said Lisa Briand, associate professor and program director for Temple University’s neuroscience program.
At Temple, neuroscience has become the fourth largest of 30 majors in liberal arts, Briand said. The psychology department a few years ago changed its name to psychology and neuroscience, she said.
At the University of Pennsylvania a decade ago, 100 to 120 neuroscience majors graduated annually, said Lori Flanagan-Cato, associate professor of psychology and codirector of the undergraduate neuroscience program.
“Twice in the past 3 years we have had over 150,” she said.
Swarthmore College, a highly selective small liberal arts college, graduated 10 to 12 neuroscience majors a year about a decade ago, said Frank Durgin, professor of psychology who oversees the program.
“This year, we anticipate graduating 24 majors,” he said. “Next year, it’s 30.”
The college has added two professors in the last two years to accommodate growth, he said.
Why students study neuroscience
In a lab at Haverford one afternoon last month, 16 students in white lab coats poked with paintbrush tips at thin slices of rat brain in preservative fluid, preparing to stain them to look for which neurons were activated. Some of the rats received the drug Ritalin, commonly used for attention deficit disorder, while others did not. Students were trying to discern differences in their brains when they performed certain tasks, said Laura Been, associate professor of psychology and director of the bi-college neuroscience program.
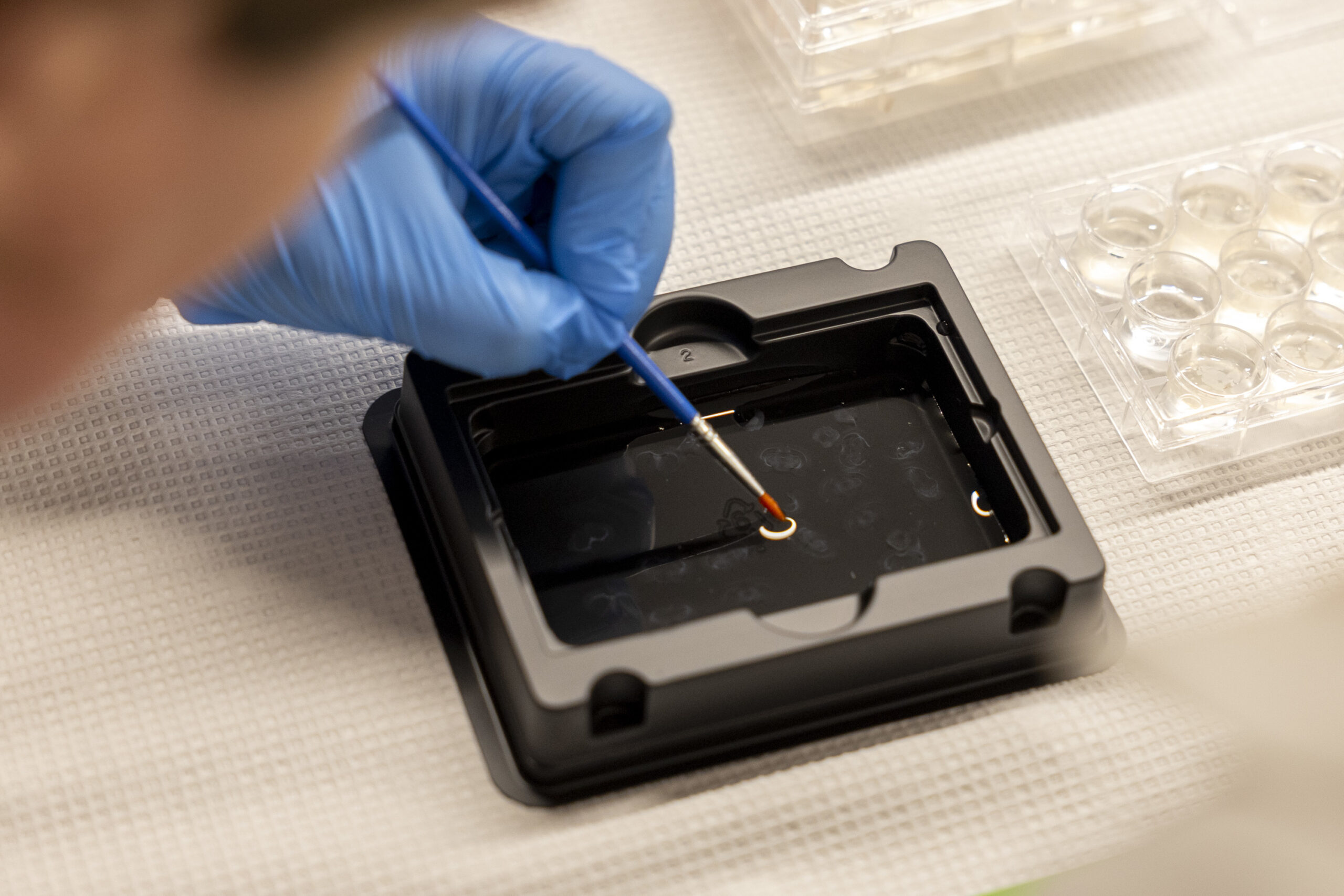
A neuroscience student works with sections of rats’ brains in a lab at Haverford College.
“We can … try to learn something more about how this sort of drug treatment impacts the brain,” said Been, whose area of interest is behavioral neuroendocrinology, which looks at the relationship between hormones, the brain, and behavior.
Students in Been’s class had varied reasons for studying neuroscience.
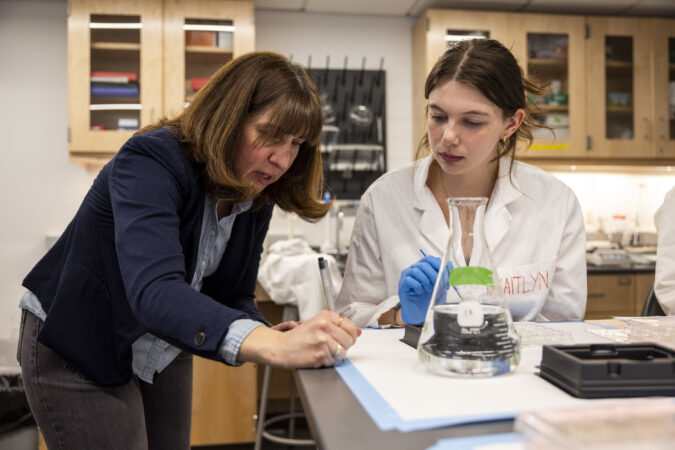
Emily Black, visiting assistant professor of neuroscience at Haverford College, helps Savannah Shaw, 22, of Downingtown, during neuroscience lab work. “I really like the variety of the classes we can take in the major,” said Shaw, a senior who plans to go to medical school, possibly to become a neurologist. “You can go more the psychology route or go more biology.”
Sophia Lipari, 21, a junior from Jacksonville, Fla., whose father is a reproductive endocrinologist, is interested in hormones and the field of fertility.
Riley Fass, 20, a junior from Claremont, Calif., wants to be a special-education teacher. She already sees the connection between neuroscience and her job as a teacher’s assistant at a school where children have traumatic brain injuries and cerebral palsy.
“The topics we discuss — an injury here will result in this — I can actually see it in my students,” she said.
Iris Goxhaj (left), 21, of Northeast Philadelphia, and Riley Fass, 20, of Claremont, Calif., work with sections of rats’ brains in a lab at Haverford College.
Deeya Abrol’s interest was stoked when she worked with a child on the autism spectrum as a swim instructor. Abrol, 22, a senior from Los Gatos, Calif., plans to go to medical school.
Schechtman-Taylor meanwhile wants to pursue biomedical engineering and specifically developing medicines for the treatment of neurodegenerative disorders.
“I want to work on the treatment side,” she said.
Fairman, the Haverford biology professor, said a recent graduate’s mother had died of Huntington’s disease, meaning she has a 50% chance of getting it, he said. She worked in his lab and wanted to be involved in hisresearchon protein clumping in the brain and its effect on diseases such as Parkinson’s and Alzheimer’s.
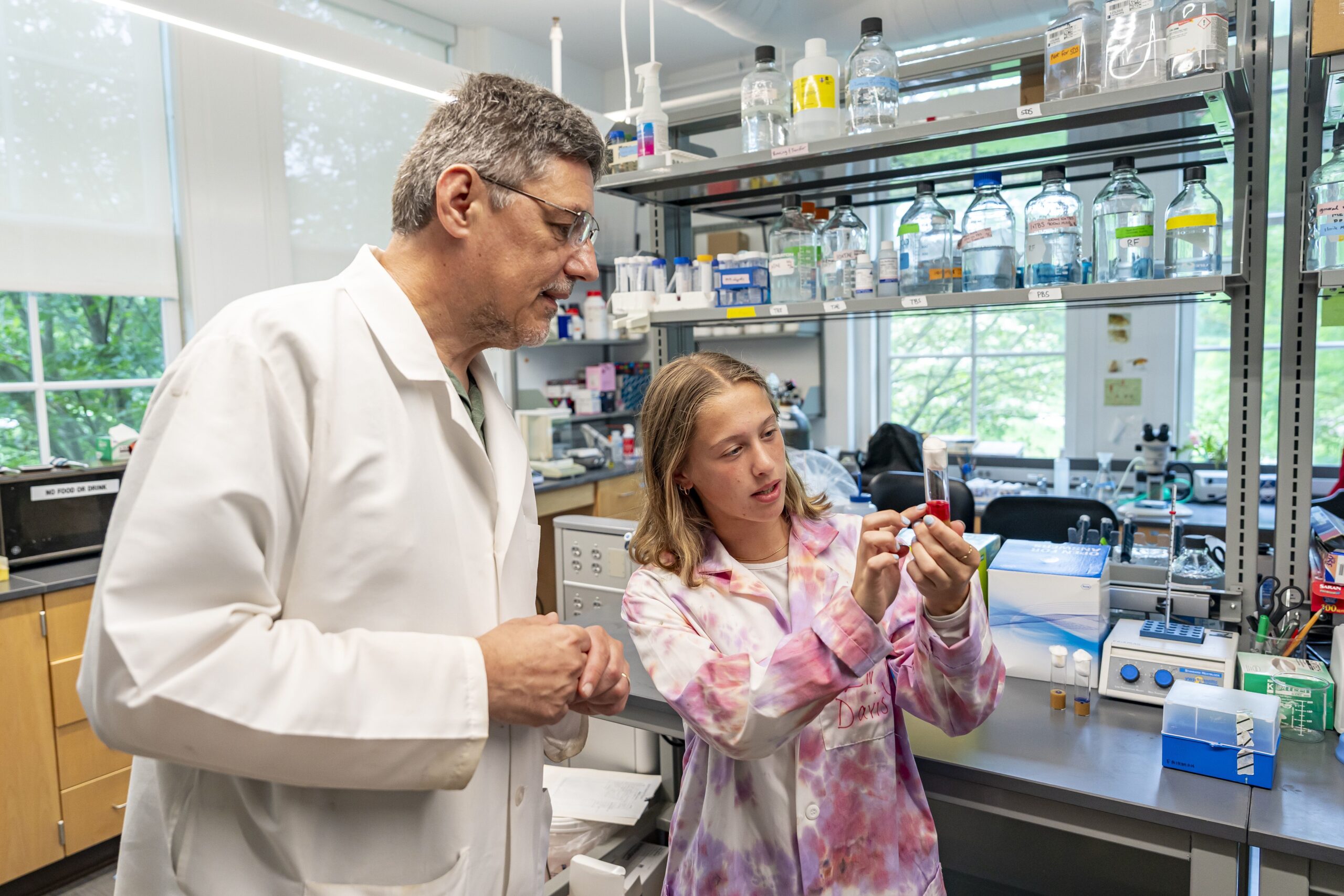
Rob Fairman, a professor of biology at Haverford College, and student Liv Davis are testing the effects of natural products on animal models with neurodegenerative diseases.
Junior Liv Davis, 21, wanted to help find a cure for Parkinson’s, which struck her grandmother in 2020.
“She’s had two falls in the last year and a half because it’s progressed pretty quickly,” said Davis, of Lanoka Harbor, N.J. “It’s hard to see someone you love so much live with it, but it makes it all the more rewarding to work toward fixing it.”
Davis, who has worked in Fairman’s lab since her freshman year, tried to get into an introduction to neuroscience class early on. But there wasn’t room. She ended up majoring in biology, which she thinks probably would have happened anyway.
About half the students working in Fairman’s lab are neuroscience majors, he said.
Davis is currently studying the effect of a chemical on sleeping fruit flies that have been genetically modified to carry the protein associated with Parkinson’s.
Last summer, she received an inaugural research fellowship funded by Shamir Khan, a Haverford alumnus and psychologist who was diagnosed with early-onset Parkinson’s.
Her grandmother was glad she could continue the research, said Davis, who plans to become a doctor.
“She always jokes with me,” Davis said. “‘Give me a spoonful of that chemical, whatever it is. If you need a test subject, you let me know.’”
At AMS Surgery Center in suburban Montgomery County, patients can park right in front of the entrance, walk through just a few doors, and undergo cardiac procedures in a sterile operating room with equipment as high-tech as in any hospital procedure room.
In the year and a half since its first patient underwent a cardiac catheterization, the center has performed more than 1,000 cardiac procedures that previously required patients to go to full-service hospitals.
The Horsham center showcases a new front as sophisticated healthcare procedures move to freestanding outpatient medical facilities, promising to save patients money. The shift also adds to the financial pressures facing the region’s hospital-centered health systems.
Four centers have opened or are in the final stages of approvals in Southeastern Pennsylvania. Their arrival comes after state lawmakers in 2022 broadly expandedthe types of procedures allowed outside hospitals to include cardiac catheterizations, pacemaker implants, and other treatments that until then had to be done in a hospital.
Pennsylvania is the first Northeastern state to allow the minimally invasive procedures in freestanding surgery centers, but Southern states like Florida, Louisiana, and Texas have permitted the practice for decades, experts said. Research has found surgery centers generally are as safe as outpatient departments in hospitals.
An independent physicians group, Bryn Mawr Medical Specialists Association, opened Heart & Vascular Center of the Main Line — the Philadelphia region’s first such center — in late 2022. in Bryn Mawr. AMS Surgery Center in Horsham performed its first procedure in the fall of 2024, initially treating only Medicare patients. Itadded patients with private insurance last summer.
The market has continued torapidly expand:ReVaMP Heart & Vascular Surgery Center in Center City started treating Medicare patients last fall. The Ambulatory Cardiovascular Center of Pennsylvania, near King of Prussia, expects to perform its first procedures on patients next month.
Medicare pays the centers about a third less than hospital outpatient departments for the same procedures, but the centers have significantly lower costs, allowing them to be profitable. Medicare pays physicians the same wherever procedures are done.
Independent cardiology groups traditionally have performed interventional procedures, such as implanting stents and pacemakers, in hospitals. Some are jumping at the opportunity to expand through the surgery centers, where they can have a financial stake in the entire operation.
“We’ve always been very fiercely independent, fiercely entrepreneurial, and patient-centered,” said Richard Borge, an AMS interventional cardiologist who is medical director for the group’s surgery center.
How much cardiac care — among the most profitable business lines for hospitals — will move out of hospital outpatient departments remains unknown. But cardiac surgical clinics will not take over heart care to the extent seen when outpatient orthopedic centers began offering hip and joint replacements,predicted Lauren Clementi, a senior vice president at Kaufman Hall, a Chicago consulting firm.
“This one’s a little trickier because the acuity of patients,” she said.
Cardiologists will continue treating many patients with complex medical needs in hospitals, which remain the only option for riskier procedures such as open-heart surgeries.
Gregory Schmitt went to AMS Surgery Center to undergo procedures for a heart stent and stents in both legs.The retired machine-shop owner, who lives in Ivyland, called such centers great for patients.
“I highly recommend it. It’s much easier than trying to navigate a hospital,” Schmitt said.
How we got here
Healthcare has been shifting awayfrom requiring overnight hospital stays, even for common procedures like cataract surgery.The trend starteddecades ago with same-day procedures in hospitals, followed by the rise of freestanding surgery centers.
In cardiology, people now commonly receivestents and pacemakers as outpatient care. But until recently, doctors had to implant the devices in a hospital.
“Once upon a time, every patient we cathed had to spend the night in the hospital,” said veteran cardiologist Mark Victor, referring to cardiac catheterization.
With the rise of outpatient procedures,Victor said, the question for many clinicians became: “If they’re hospital ambulatory, why do they have to be in the hospital at all?”
Victor has long advocated for the adoption of outpatient cardiology proceduresas the CEO of Cardiology Consultants of Philadelphia. Thelarge cardiology practice joined last year a national private-equity backed group, Cardiovascular Logistics, and will soon start performing surgical procedures at the center opening near King of Prussia.
In 2020, Medicare started paying for outpatient cardiac catheterizations — which entail running a catheter through a blood vessel in the thigh or wrist to examine the heart and install devices like stents.
Richard Borge is medical director of AMS Cardiology Surgery Center in Horsham, whose arrival is moving advanced cardiac care from hospitals to outpatient clinics.
Even then, Pennsylvania rules required cardiac catheterizations to occur in an acute-care hospital, according to Stephen Abresch, director of government affairs for the Ambulatory Surgery Center Association, a national trade group in Alexandria, Va.
Pennsylvania lawmakers cleared the way for expansion byeliminating that restriction in 2022 as part of a broad expansion of what the state’s surgery centers were allowed to do. “It had been a quarter century since the state had gone in and reviewed that,” he said.
The Heart & Vascular Center of the Main Line has scheduled its first cardiac ablations this week. Horsham’s AMSaims to start offering those procedures in June. Victor’s King of Prussia groupexpects to add ablations in the future as well.
Impact on hospitals
It is too soon to know how the new surgery centers will impact the region’s existing health systems. In some cases, independent cardiologists generate significant patient numbers forhospitals’ cath labs.
After Bryn Mawr Medical Specialists opened its cardiovascular surgery center near Main Line Health’s Bryn Mawr Hospital, the private group performed fewer procedures on low-risk patients at the hospital.
To sustain patient volumes, Main Line has increased collaboration with other physician practices, while continuing to treat an“older patient population, whose more complex health conditions require the advanced expertise and emergency support only a hospital setting can provide,” officials said in a statement.
In Horsham, most of the patients coming to AMS would have gone toJefferson Abington Hospital before the surgery center opened in partnership with Atria Health, a private-equity backed group, Borge said.
Jefferson declined to comment.
King of Prussia’s Ambulatory Cardiovascular Center of Pennsylvania is opening through anunusual four-way partnership involving Cardiology Consultants of Philadelphia, Cardiovascular Logistics, SCA (a unit of UnitedHealth’s Optum), and the University of Pennsylvania Health System.
“Ours is not going to seriously impact any one hospital system, which they’re all relieved about,” said Victor, who is also president of the Mid-Atlantic region for Cardiovascular Logistics. He said other health systems were invited to invest in the surgery center, but only Penn did so.
Penn declined to comment for this article. On the Alvarez & Marsal What’s Your Moonshot podcast, the health system’s chief operating officer, Michele Volpe, recently said the system needs ”to move a bit faster in taking much of the work that we are doing in inpatient ORs and moving them into outpatient or ambulatory freestanding ORs.”
AMS Cardiology’s ambulatory surgery center in Horsham is one of four new cardiovascular surgery centers in Southeastern Pennsylvania.
Center City’s ReVaMP Health & Vascular Surgery Center wantsto bring in cardiologists from nonaffiliated practices,and even the city’s big health systems. The facility opened last year, spearheaded by Re-Vasc Med Professionals’ two interventional cardiologists in partnership with Surgery Partners, a publicly traded manager of surgery centers nationwide.
“I’m 100% sure this is going to be the trend of the future,” Re-Vasc CEO and founder Jon George said.
A health insurer’s perspective
Richard Snyder, a top executive at Independence Blue Cross, the largest health insurer in Southeastern Pennsylvania, has for years watched joint replacements and other procedures shift from hospitals to lower-cost surgery centers.
The financial impact goes beyond the lower prices at surgery centers, he said, expecting that hospitals will not simply cede these patients to new competitors.
Some hospitals might decide to take a lower payment for outpatient procedures. “Traditionally, that happens when we have capacity in lower-cost settings,” he said.
At the same time, Medicare is pushing to pay the same price for services, wherever they are performed. “Hospitals, by necessity, will need to move some things to lower-cost settings in order to not lose money on them,” Snyder said.
University of Pennsylvania health expert Ezekiel Emanuel’s casual conversations often evolve into impromptu medical consultations.
People askEmanuel — an oncologist, bioethicist, and health policy scholar who helped write the Affordable Care Act — how to live healthier.
He said that “incessant asking” inspired him at a time when both information and misinformation are booming in the wellness space.
His new book, “Eat Your Ice Cream: Six Simple Rules for a Long and Healthy Life,” landed on bookshelves in January. He uses the pages toargue that the goal of life should not be to simply live the longest, but rather to lead a healthy and fulfilling life.
The Penn professor, who has antique maps in his office and has taught a course on Ben Franklin, weaves inhis appreciation for history throughout the book. Emanuel’s advicealso addresses contemporary issues such as vaccines and vaping. And hesharespersonal family stories involvinghis father (to whom the book is dedicated).
In one of his favorite anecdotes, he describes looking for a cheap car to buy with his bar mitzvah money. Thinking he found a great deal on a Volvo, Emanuel and his brother bought the car, brought it home, and realized it couldn’t go in reverse.
“My father says, ‘You guys are schmucks!’” he recalled.
That became the first of his six rules: “Don’t be a schmuck — avoid self-destructive risks.”
The Inquirer spoke with Emanuel about tips for livinga healthy life in a conversation lightly edited for length and clarity.
Why do you think wellness has become so big?
People feel like the world’s topsy-turvy. They’re not controlling it. It is controlling them. They want to assert control over the world, and one way they can do it is through wellness.
What have people gotten wrong about wellness?
Spending 10 hours a week on wellness, like some people recommend, is crazy. Just insane. You should not do that. You can spend two or three hours a week, get all the benefit you need, and focus your time on other things — your family, close friends, having a successful career, making the world better, making Philadelphia better. Those are the things that matter.
What does your first rule (Don’t be a schmuck) mean?
The first rule is, really, take reasonable risks, but not unreasonable risks.
The most dangerous thing most of us do in everyday life is turn the ignition on in our car. Driving is actually quite dangerous over a lifetime. And you have to compare the risk you’re willing to take to the risk of driving. I try to organize a chapter laying out unreasonable risks like BASE jumping [an extreme sport in which a person parachutes from a dangerous height]. Why is that so stupid? Well, look at the data. I try to make that assessment much more quantitative.
What is your second rule?
The importance of social relations.
It doesn’t get emphasized by almost anyone in the [wellness] field, and it’s vastly the most important for longevity, for health, and for happiness. We’ve got tons of data. There’s more than 3 million people who’ve been studied on the relationship between loneliness, social isolation, and ill health.
If you look at the Harvard Study of Adult Development, which started in the late 1930s, the single most important predictor of a long, healthy life with the fewest comorbidities is the number and quality of your social relationships.
Overall, a professor at Brigham Young University has summarized that being socially isolated is ‘like smoking 15 cigarettes a day.’
Tell us about your last four rules.
The third one is stay mentally sharp. If the body’s working fine, but cognitive decline has set in, that would be hell to me. I don’t want to live like that.
There are only a few people like Ben Franklin where it does not appear to decline at all. One of the things actually I learned after I finished the book is Franklin was the oldest person (aged 81) at the Constitutional Convention in 1787. He was still very nimble with his mind, able to put things together, to craft compromises and things.
Some of it’s obviously genes, but some of it’s also things you can do — what you can eat, how you exercise, your retirement, your strategies, social interaction, challenges, etc. The brain is a lot like muscle in that either you use it or you lose it.
The last three rules are the typical: eating well, exercising, and sleeping advice.
Are there things that you’d want the media to emphasize more when talking about wellness and health?
There are two really fundamental things on the ‘to do’ side for eating.
One is you should eat more fermented foods. Whether it’s yogurt or cottage cheese or aged cheeses or kimchi. It’s very important for the microbiome. In Philadelphia, one of our treasures is Di Bruno Bros.cheese shop. They have 200 cheeses on display. Go and get some cheese. It’s really good.
The other is that more than 90% of Americans don’t get enough fiber in their diet every day. You need to eat more fruits and vegetables. I start out every day by merging these two. This morning, I had a bowl of berries, or some kind of fruit, with yogurt, granola, and oats. I also added hemp hearts, which are high in protein, good fats, omega-3s and omega-6s. Then add a salad at dinner, and you pretty much have enough fruits and vegetables.
Can you explain the title of your book, “Eat Your Ice Cream“?
Ice cream is good. Dairy products are associated with higher height, especially if, early in life, you eat a lot of dairy. Second, [dairy consumption] is also associated with a lower risk of colorectal cancer, which is all in the news these days.
And most importantly, it’s about joy. It’s fun. Who doesn’t like ice cream? But it’s important to get good ice cream, not stuff with emulsifiers and fillers and all of that.
Have a little joy. It goes a long way toward making life lovely.
Every Cure, a biotech nonprofit started by a University of Pennsylvania researcher, has landed $76 million in federal funding to advance its artificial intelligence match-making tool that identifies existing drugs to treat rare diseases.
Over the next three years, Philadelphia-based Every Cure will use the funding from the Advanced Research Projects Agency for Health (ARPA-H) to pursue preclinical studies for at least 20 drugs that show promise for being repurposed for rare diseases with no other treatment options. The company will also pursue clinical trials to further test the safety and effectiveness of repurposing another 10 existing drugs.
The nonprofit was co-founded in 2022 by David Fajgenbaum, an associate professor at University of Pennsylvania, after his own experience with a rare disease.
He was diagnosed with Castleman disease as a medical student at Penn, and experimented in a campus lab with his own blood to try to find an off-label medication that could address his symptoms.
Every Cure’s AI tool expedites a drug discovery process that is otherwise often left to chance. When patients with rare diseases have few treatment options, doctors may scour medical journals or tap expert networks for leads on other drugs to try with mixed results.
The tool automates the process, using an algorithm to read massive biomedical data about diseases, medications, genes, and proteins. The tool looks for bits of data that diseases and medications may have in common that were previously unrecognized.
“This next phase will allow us to do the essential work of evaluating these potentially life-saving treatments in the lab and clinical trials, accelerating access to potential treatments for those who urgently need them,” Fajgenbaum, Every Cure’s President, said in a statement.
The new funding adds to $108 million in federal support the nonprofit has already received.
An Arizona State University vice provost and dean, who has degrees in mathematics and geography and has studied urban planning, will become Temple University’s next senior vice president and provost.
Elizabeth “Libby” A. Wentz, 62, an Ohio native with a doctorate from Pennsylvania State University, will step into her new role at Temple July 1, subject to approval by the board of trustees, the school announced Monday.
“My background in urban planning has kind of shaped who I am and shaped my thinking, and I just think that there’s so many great opportunities for recruiting students, for creating internships for students, for creating research experiences for students in an urban environment that the university’s rural counterparts don’t have in the same way,” Wentz said in an interview.
Wentz has overseen Arizona State’s Graduate College since 2020 and previously was dean of social sciences, which included geography and urban planning. She will replace David Boardman, who has been Temple’s interim provost since July when Gregory Mandel left the job. Boardman was not a candidate for the job and will continue his role as dean of the college of media and communication.
As Temple’s provost — essentially the university’s number two leader — she will oversee 17 schools and colleges, multiple campuses, and the school’s undergraduate, graduate, and professional programs.
She is the first provost in at least more than a decade to come from outside the university and was selected through a national search, chaired by a faculty member and a dean.
“Libby sort of stuck out for me after the hour I spent with her as being literally right on the same page relative to her ability to articulate the mission and the purpose of Temple and why that was so important,” Temple president John Fry said in an interview.
He was struck by her commitment to student success, he said. “She obviously had time to interact with students and, I think took like really special care and interest in our students,” he said.
And, Arizona State has grown tremendously in part because of its commitment to online programs, he said, which are a priority in Temple’s strategic plan. Temple has lost about a quarter of its enrollment over the last decade.
“We don’t have the kind of online enrollment that you would expect a place like Temple to have,” Fry said. “One of the things Libby and I did speak about was her familiarity with the ASU online infrastructure. She’s taught in it. She obviously has led parts of it.”
Temple remains amid searches for several other key positions, including chief operating officer and law and engineering school deans.
Wentz said she was attracted to Temple because she wanted to remain at an urban university and has long admired the work of Fry, who has had a longstanding relationship with Arizona State president Michael M. Crow. Temple a year ago became part of the University Innovation Alliance, a small nonprofit sponsored through Arizona State that is aimed at finding innovations to improve learning and increase college attendance, retention, and graduation rates ― especially for low-income students ― then scaling those innovations.
“They built a really strong rapport and have a very similar philosophy around higher education which also very much aligns with kind of my own interest and my own philosophy,” Wentz said.
Both Temple and Arizona State, which has its main campus in Tempe, are major research institutions; Arizona is much bigger with over 194,000 students, compared to Temple with more than 33,000, including its international campuses.
“Honestly the biggest difference [between the two] is the weather right now,” Wentz joked, noting that it was 81 and sunny in Tempe on Sunday as Philadelphia prepared for blizzard conditions.
Arizona State does not have a faculty union, so learning to work with Temple’s faculty union will be new.
“That’s going to be an exciting area for me to learn about,” she said.
Urban planning background
Fry has a reputation as an urban planner and in his prior leadership jobs at the University of Pennsylvania, Drexel, and Franklin and Marshall focused on development and improving the campuses and their neighborhoods. He has aspirations for Temple, too, including building an “innovation corridor” stretching from Temple’s recently acquired Terra Hall at Broad and Walnut Streets in Center City to the health campus, a little more than a mile north of main campus on Broad Street.
Wentz said she and Fry had not talked about urban planning, but that she looks forward to working on the university’s new strategic plan, which includes more green spaces, a new 1,000-bed residence hall, a STEM complex, and an emphasis on more attractive and defined entrances to its North Philadelphia main campus. The three pillars of the plan are student success, research in action, and place-based impact.
“Those are going to be some really exciting conversations that I look forward to having with John, as well as with the Temple planners to think about how do we make it a safe space for students and a great learning environment.” she said.
During a 2022 talk at Arizona State, Wentz discussed how urban planning figured into her work.
“Most of the work that I do applies to the urban environment and urban analytics, so trying to understand how it is that cities work and trying to make the physical urban environment a better place for people to live,” Wentz said during that talk.
Building trust and collaboration
In her new role at Temple, she said, early on she will focus on getting to know the community and the university’s financial model and make clear her commitment to shared governance and data-informed decision making.
Wentz, who grew up near Cleveland and got her bachelor’s in mathematics and master’s in geography at Ohio State University, spent the last 30 years at Arizona State. She became a professor there in 1997.
She helped the university launch its medical school and has grown graduate enrollment and graduate student funding.
Wentz said she prides herself on building a culture of trust and collaboration and has worked with the local community. She said she’s looking forward to doing the same at Temple.
She plans to come to Philadelphia in a couple weeks and look for a place to live, she said.
“I’m going to come after the snowstorm, I think, instead of before,” she said Sunday.
When Sarah Bynum was pregnant with her first child in 2017, her primary care doctor suggested she stop taking her antidepressant.
He told her there wasn’t enough research to justify staying on the medication.
By the time she delivered her daughter, the Delaware County woman’s anxiety was so bad that she decided never again togo through a pregnancy without her antidepressant.
Bynum, who has taken medication for anxiety since she was a teenager, is one of the nearly 18% of women in the U.S. on an antidepressant. She takes a drug known as an SSRI, the most common class of antidepressants, which medical societies generally consider safe to use during pregnancy.
Kelly Zafman, an OB-GYN at the Hospital of the University of Pennsylvania, decided to research the issue that has also recently been under discussion on the federal level.She’s observed that patients often get mixed-messaging from providers.
“The other side of the conversation that gets missed is this risk of not continuing medications,” said Zafman, who is in her final year of fellowship training in maternal-fetal medicine.
Preliminary findings from herresearch showed the risk of a mental health emergency nearly doubled in women who discontinued SSRIs or SNRIs (another popular type of antidepressant), compared to those who stayed on their medication.She presented the unpublished resultsthis month at the meeting of the Society for Maternal-Fetal Medicine.
The analysis used data from 1,462 privately insured Pennsylvania women with active antidepressant prescriptions who gave birth between 2023 and 2024. While pregnant, 81% of them stopped or interrupted usage.
Zafman said the highly personal decision comes down to factors such as the patient’s prior pregnancies, mental health history, and how well-controlled their symptoms are.
Ultimately, the potential risks have to be weighed against those of untreated depression or anxiety.
“It’s really a risk‑risk conversation,” Zafman said.
Research on the safety of antidepressants in pregnancy continues to evolve. Some potential risks identified in older research appear overstated when compared with more recent, better-designed studies, Zafman said.
She cited as an example a rare but serious condition called persistent pulmonary hypertension — which causes a breathing issue — for which scientific evidence remains conflicting.
“There’s definitely an association, but it’s not totally clear how causative it is,” Zafman said.
Another concern, neonatal adaptation syndrome, tends to involve mild difficulties with feeding and breathing thatresolve within days. Medical intervention is rarely required, and the treatment essentially is to cuddle and feed your baby, Zafman said.
While antidepressants potentially pose risks in pregnancy, she said, overall, the risks of long lasting effects are “extraordinarily low.”
A personal decision
Bynum, a patient at Penn Medicine, was not on antidepressants during her first pregnancy. (She was not part of this particular study but has participated in other research with Zafman.)
Five months into the pregnancy, she learned her daughter would be born with a congenital heart defect that would require monitoring, and later, surgery.
Family and friends tried to help her, but they weren’t able to calm her heightened anxiety the way her medication usually would.
When she became pregnant with her second child, she knew she wanted to have a “more mentally healthy pregnancy.”
“I needed to be mentally and physically present not just for myself, but my daughter,” she said.
She asked her OB-GYNs if she could continue on her antidepressant, Paxil. They weren’t sure.
She turned to the fetal heart experts at Children’s Hospital of Philadelphia, who looked into the medical evidence and told her it was fine to continue taking her antidepressant.
Sarah Bynum decided she would not go without her antidepressant for future pregnancies.
Bynum has since had three healthy pregnancies while taking the antidepressant.
She felt it was the right decision.
“I need to focus on having a healthy pregnancy with as minimal stress as possible,” Bynum said. “And if that means taking a medication, that’s what’s gonna work.”
Editor’s note: This story has been updated to clarify a quote by the researcher.
Following several years of major worker organizing efforts and high-profile strikes, 2025 brought a change in momentum for the labor movement. President Donald Trump’s administration sought to end federal workers’ union contracts and, through a firing, left the National Labor Relations Board without a quorum and unable to make decisions.
But the percentage of workers who are union members nationwide has stayed pretty steady in the last year, new data shows. And in Pennsylvania and New Jersey, union membership rates fell.
In 2025, 10% of the country’s total workforce was part of a union, compared to 9.9% in 2024, according to new data from the U.S. Bureau of Labor Statistics. It’s the first time since 2020 that the rate has inched up — albeit slightly — instead of down.
However, BLS noted, this year’s estimates are not fully comparable to past years because they are based on a BLS survey that is missing October figures due to the government being shut down in October and part of November.
In the past year, there have been “a lot of kind of anti-labor efforts coming out of the White House,” said Todd Vachon, assistant professor of labor studies and employment relations at Rutgers University.
Despite those efforts Vachon said, “labor has pretty much maintained the same at the national level. … The Trump attacks haven’t really had any effect yet, at least in the first year.”
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Union membership rates dropped to an all-time low nationwide in 2023 and remained pretty similar in 2024. During those years, roughly one in 10 U.S. workers was part of a union.
When BLS first started recording this data in 1983, about two in 10 U.S. workers were unionized. There were 17.7 million unionized workers in 1983 and 14.7 million last year.
Danny Bauder, president of the Philadelphia Council AFL-CIO, speaks at an event supporting federal workers in October.
Unionizing in N.J. and Pa.
In New Jersey, 14.7% of workers were unionized last year, and in Pennsylvania, it was 10.9%.
In both states, that was a decline of around one percentage point from 2024, but BLS noted that state-level data “should be interpreted with caution,” due to the shutdown-related incomplete data.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Some local labor action highlights from this past year include:
Whole Foods unionization: Workers at the Spring Garden location voted to form a union in January, becoming the first unionized Whole Foods staff. Whole Foods challenged the election, and the NLRB was without a quorum to decide the case last year.
Graduate student workers at the University of Pennsylvania reached a tentative agreement on a first contract this month after threatening to strike, nearly two years after unionizing.
Employees of several hotels went on strike in Octoberand November as their union, Unite Here Local 274, sought new contracts for roughly 1,000 members at eight Philadelphia hotels.
National Starbucks strike: Philadelphia Starbucks workers joined a nationwide strike in November amid contract negotiations. Some have returned to their jobs, but over 1,000 continued to strike as of early February.
New teacher contract: The Philadelphia Federation of Teachers got a new contract for 14,000 teachers, nurses, counselors, secretaries, and paraprofessionals, averting a strike.
Some 271,000 federal jobs were cut between January and November. Meanwhile, the union membership rate in the public sector increased by 0.7% nationally in the last year according to the new BLS data.
Vachon notes that the vast majority of public sector workers are at the municipal level, not federal.
“The hiring of police, and teachers, and sanitation workers across the thousands of cities around the U.S. more than compensated for [cuts at the federal level], because we see an increase in the public sector,” he said.
Trump also fired a member of the National Labor Relations Board (NLRB) early last year, which left it without a quorum to issue rulings. In some cases that can slow down the formation of a new union — at the Amazon-owned Whole Foods in Philadelphia, for example.
The number of union elections overseen by the NLRB declined last year and the overall number of workers involved in those elections dropped too, according to the nonpartisan Center for American Progress.
“A huge percentage of new union organizing is required every year just to maintain the same level of unionization, because of the churning and the growth of the overall labor force,” said Vachon. “If the labor force is not growing, then you can actually see increases in union density.”
And unions are being cautious of reaching out to the NLRB under the Trump administration, he notes.
“There’s a fear [that] if something gets sent up to the NLRB that the ruling is going to set a precedent that makes it even more difficult to organize,” said Vachon. “It’s kind of had a dampening effect in that way.”
Wawa customers have been able to order roasted chicken on sandwiches, salads, burritos, and more since summer 2024. Hoagie-loving Philadelphians may scroll past the high-protein option on Wawa’s trademarked built-to-order screens, while others tap its icon instinctively in their rush to order lunch.
Wawa CEO Chris Gheysens said he sees the chicken breast differently.
From idea to inception, “that was a labor of love for quite a long time,” Gheysens said in a recent interview. “It’s 37 grams of protein, something consumers are really looking for today.”
And, he added, “it’s still highly customizable, which our customers love doing at Wawa.”
To Gheysens, the menu addition shows how the Delaware County-based company responds to consumer demand. Just as it did decades ago when Philly-area store managers began brewing coffee for customers on the go, and in 1996, when Wawa executives decided to start selling gasoline.
Even now, with nearly 1,200 stores in 13 states and Washington, D.C., Wawa is still listening to consumer feedback, Gheysens said. And despite expanding as far away as Florida and Kentucky, the CEO said, the convenience-store giant remains especially in tune with its hometown fans.
“For a lot of people, it’s their daily routine,” said Gheysens, a South Jersey native. “It becomes a part of their neighborhood. It’s a relationship that’s built on consistency, on trust” — and on getting customers out the door in five minutes or less, depending on the time of day.
(function() { var l = function() { new pym.Parent( ‘wawa-stats__graphic’, ‘https://media.inquirer.com/storage/inquirer/ai2html/wawa-stats/index.html’); }; if(typeof(pym) === ‘undefined’) { var h = document.getElementsByTagName(‘head’)[0], s = document.createElement(‘script’); s.type = ‘text/javascript’; s.src = ‘https://pym.nprapps.org/pym.v1.min.js’; s.onload = l; h.appendChild(s); } else { l(); } })();
Customers say they are drawn to the homegrown chain for its convenience, consistency, quality, and wide-ranging menu of grab-and-go and made-to-order items (even though some miss the old Wawa delis where lunch meat was sliced on the spot).
In Runnemede, 78-year-old Barbara MacCahery said she goes to her local Wawa at least a couple of times a week — “sometimes for breakfast, sometimes for a sandwich, a lot of times for coffee.”
In MacCahery’s mind, she said, the chain has proven itself time and time again for decades: “It’s very rare that you’ll have a bad experience.”
Wawa’s ‘secret sauce’ for success
More than 100 years ago, Wawa started out as a dairy, delivering milk to Philadelphia-area households.
Wawa has set a national standard for success in the convenience-store industry, said Z. John Zhang, a marketing professor at the Wharton School of the University of Pennsylvania.
“It really is some kind of a secret sauce,” said Zhang, who studies retail management. “For many people, Wawa has become a destination store,” one that combines “speed, customization, and perceived high quality” with near-constant availability — many Wawa stores are open 24/7.
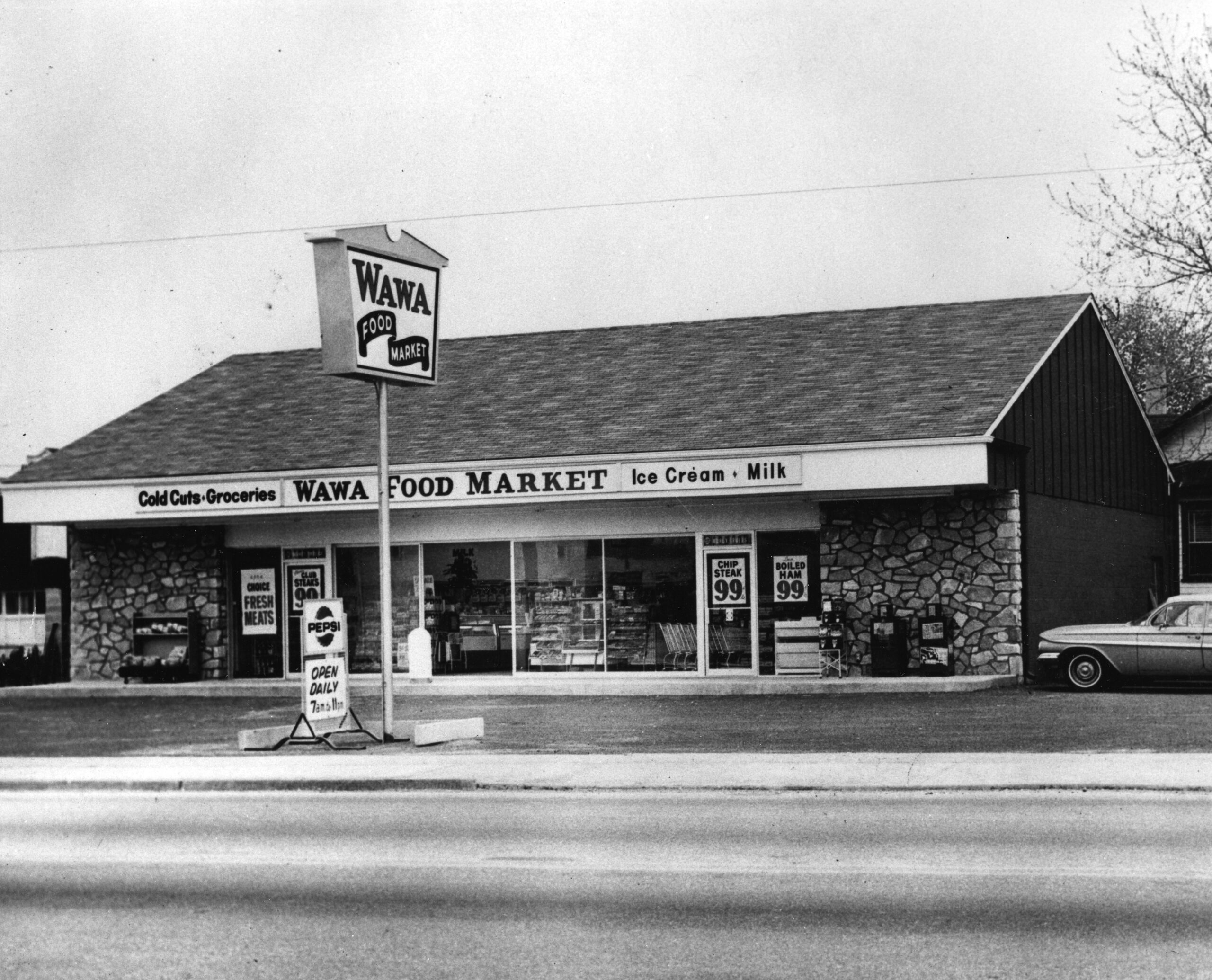
The company got its start as a dairy, delivering milk to Philly-area households. In 1964, it opened its first store in Folsom. Soon, the family-owned company expanded into New Jersey and Delaware, and established a reputation for quality and speed, with slogans like “People on the Go — Go to Wawa Food Markets.”
Wawa’s first convenience store opened in Folsom, Delaware County in 1964.
Wawa is privately held, owned in part by workers who get a percentage of their earnings contributed to an employee stock-ownership plan. Zhang said this program likely leads to more-invested employees who provide better customer service.
Because Wawa is not public, it is not required to disclose its finances, and company executives declined to discuss them.
But by many appearances, Wawa seems to be doing well: Over the last decade, the company has increased its store count by about 65% and doubled its workforce to about 50,000 associates.
Philly-area Wawas are often crowded, too, which is key to making money in the convenience-store industry.
A gas attendant fills up a customer’s tank at a Wawa in Pennsauken in 2020.
“We think it’s high-impulse, but 80% of all people who walk into a convenience store pretty much know what they want,” said Zelinski, who consults with retailers. (He declined to discuss specific companies and said he has never worked for Wawa.)
Successful operators have encouraged customers to spend more by adding seating and improving their food service, Zelinski said. And stores with better food see higher profit margins.
“Once you have somebody that’s addicted to your food service program, they’re more likely to come back to your store vs. a competing store,” he said.
In 2020, Wawa debuted new menu offerings, including hamburgers, pot roast, rotisserie chicken, pasta alfredo, and kids meals, at a tasting in Media.
Wawa has certainly gotten people hooked on their coffee, hoagies, and ever-expanding menu, Zhang said. Options added in recent years include pizza, wraps, protein-packed “power meals,” limited-edition coffee flavors, and smoothies “boosted” with protein, vitamins, and minerals.
This older Wawa in Cherry Hill closed in 2024. The township has six remaining Wawas.
Despite Wawa’s best efforts, not all stores thrive, Gheysens said. But “luckily for us, we’re still in growth mode, and don’t have to worry about closures in a broad way.”
Gheysens said he sees room for more Wawas in the Philadelphia market — even as convenience-store competitors like Maryland-based Royal Farms and Altoona-based Sheetz have opened new stores in the region.
Wawa executives want “to make sure that we are the number-one convenience store in the area, that’s important to us,” Gheysens said. “These are our hometown counties.”
What keeps Philly-area consumers going to Wawa
A Wawa customer eats a breakfast Sizzli during the 2024 grand opening of the company’s first central Pennsylvania store.
Many Philly-area consumers grew up alongside Wawa.
In interviews with nearly a dozen of them, some were quick to reminisce about early memories of their local stores, such as the distinct smell of coffee and deli meat or the excitement of a Wawa run with high school friends. Others bemoan what has changed with the company’s expansion, including more congested parking lots.
Most have a quick answer when asked what their Wawa order is.
Rick Gunter, 45, of Royersford, misses the Wawa of his youth. Back in the day, he said, the Wawa hoagies “hit different,” with lunch meat fresh off the slicer.
Contrary to some customers’ beliefs, most stores still bake Amoroso rolls — a custom recipe made exclusively for Wawa — fresh in store multiple times a day, Gheysens said. As for the deli meat, the CEO said that was another decision rooted in customer preference.
When customers have participated in blind tests of the pre-sliced meat Wawa uses today against a fresh-sliced alternative, “they can’t tell the difference,” Gheysens said. “They would choose our pre-sliced meats, because of what we’ve done in terms of quality and the supply chain and the ability to deliver them at such a pace.”
A sandwich maker at Wawa wraps a hoagie with turkey, provolone, tomato, and lettuce in this 2020 file photo.
Some customers disagree.
“It was way better when it was kind of also a deli. Now they try to make everything for everybody,” said Bill Morgan, 79, of East Coventry Township. “I’m within five miles of three Wawas, but I rarely eat their food. Only under extreme duress.”
Morgan acknowledged he must be in the minority, given how crowded Wawas are at lunchtime. And despite his distaste for much of their food, he said he still gets gas there and loves their coffee. And he can’t help but admire their business model.
The University of Pennsylvania Health System had an operating profit of $189 million in the first six months of fiscal 2026, up from $117 million in the same period a year ago, the nonprofit reported to bond investors Friday.
Operating income increased, even after Penn put $43 million put into reserves for medical malpractice claims. Two years ago, Penn had recorded charges totaling $90 million for the same purpose.
Here are more details on Penn’s results:
Revenue: Penn had $6.76 billion in total revenue, up nearly 12% even adjusting for the inclusion of Doylestown Health in fiscal 2026. Penn acquired Doylestown last April.
“We’ve had good volume growth over the prior year, particularly in our outpatient activity,” the health system’s chief financial officer, Julia Puchtler, said in an interview.
The system has also had an increase in the acuity level on the inpatient side, she said. That translated into more revenue.
Expenses: The $43 million malpractice charge boosted overall malpractice expenses through December to $125 million, from $69 million in the same period a year ago.
It’s not that Penn is seeing more claims, Puchtler said. “It’s really the average reserve per claim that we’re seeing accelerate,” she said.
Notable: Excluding Doylestown, Penn saw a 5.9% increase in patient volumes, Puchtler said. “That’s mostly outpatient,” she said. “Outpatient surgery, endoscopy, and some of our other infusion therapy are all increased over the prior year.”
Editor’s note: This article has been updated to reflect an additional medical malpractice charge in 2024, bring the total to $90 million.