More Philadelphians are visiting emergency departments with the flu than a year ago, as cases are surging across Pennsylvania.
Flu cases in late December hit higher counts locally and statewide than at this time last year, according to city and state data. It’s too early to say whether flu has peaked for the season, or whether cases will continue to rise, health officials say.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Philadelphia-area physicians say they’re dealing with an increased flu caseload, including patients suffering from severe complications.
COVID-19 and respiratory syncytial virus (RSV) cases are also rising, but flu is the biggest concern right now, said Brett Gilbert, Main Line Health’s infectious disease chief.
“We’ve been fighting COVID for the last five years, while flu took a back seat,” he said. “But flu is in the driver’s seat this year.”
One reason for the high number of flu cases this early in the flu season, which runs from winter to early spring and typically peaks in December to February, is a new flu variant that emerged this summer.
World health experts meet twice a year to determine which flu variants are circulating and recommend seasonal flu shots to target them.
The variant causing the most cases right now, subclade K, was detected after flu shots for the Northern Hemisphere had already been selected this year, Gilbert said. “There is some degree of vaccine-disease mismatch,” he said.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
But that doesn’t mean that the current flu vaccine is not effective, especially in preventing hospitalizations and deaths.
“It may not be so great at preventing the illness itself, but [with a vaccine], it may be a mild illness, easily treatable with antivirals or supportive care,” Gilbert said.
Childhood flu vaccination rates in Philadelphia were even higher than the statewide rate, with about 56% of children vaccinated this season.
Some of the most serious cases of flu that pediatrician Daniel Taylor sees are among unvaccinated children.
At St. Christopher’s Hospital for Children, where Taylor sees patients, the outpatient sick clinic is filled with children with severe cases of flu and RSV.
Some are suffering from dehydration and require care in the ER at the North Philadelphia hospital.
Taylor stresses the risk of serious complications from the flu in conversations with parents about vaccination. (Taylor also regularly writes about his experiences as a physician for The Inquirer.)
The flu can trigger severe health crises that can cause brain damage or temporary paralysis from inflammation of the spinal cord. Taylor has seen two children this flu season with benign acute childhood myositis, a rare complication of an upper respiratory infection that causes swelling and muscle damage in the legs, and in even rarer cases can lead to kidney failure.
“They’re not able to walk, and in so much pain from the swelling of the legs,” he said.
Nine children have died nationwide from the flu this season. The season before, flu deaths among children were the highest since 2004, when the Centers for Disease Control and Prevention began tracking them, the American Academy of Pediatrics noted. Among Americans of all ages, the CDC has estimated 5,000 total flu deaths so far this season.
Taylor said that President Donald Trump’s chaotic upheaval of longstanding vaccine policy — with the CDC changing recommendations around flu vaccines and slashing six vaccines from the routine childhood immunization list — makes it harder for physicians to help patients.
He said he had recently met with a mother who told him she’d previously vaccinated her children, but now was avoiding vaccines because she was “scared of giving her kid vaccines with everything going on in the government.”
“They hear something different from the government and the CDC, and they question the relationship” with their doctor, Taylor said.
About 47% of Philadelphians have been vaccinated so far this season, above the national rate.
Patients who are feeling sick can get tested for the flu at a hospital or a doctor’s office, and home tests are also available. Antiviral treatments can help ease symptoms. Wearing a mask can also protect others from contracting the flu.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
In Philadelphia, residents can get free flu and COVID vaccines at five health centers, and the health department regularly conducts vaccine outreach in the city, said Gayle Mendoza, a spokesperson for the Philadelphia Department of Public Health.
“People might say ‘We’re past the holidays, what’s the point in getting vaccinated?’” she said. “Sure, winter break is behind us, but the influenza virus is still forging ahead.”
Sweeping changes to the United States’ childhood vaccine schedule announced Monday by federal officials will decrease the number of recommended childhood immunizations from 17 to 11.
Outraged pediatricians and infectious disease experts say the move will increase cases of preventable illnesses, hospitalizations, and deaths. Among the vaccines affected is an immunization for rotavirus whose co-inventor, Paul Offit, directs the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Now, vaccination for the serious gastrointestinal illness is among those no longer universally recommended by the Centers for Disease Control and Prevention.
The guidance change also affects immunizations for flu, respiratory syncytial virus (RSV), meningococcal disease, hepatitis A, and hepatitis B. The CDC now recommends them for children at high risk of serious illness, or when parents of otherwise healthy children decide with their doctor to give their child vaccines for these diseases.
The CDC’s move is the latest in a chaotic upheaval of the nation’s vaccine policy overseen by Health and Human Services Secretary Robert F. Kennedy, Jr.
“I think the goal of RFK Jr. is to make vaccines optional,” said Offit, a longtime critic of Kennedy, saying the anti-vaccine activist “is doing everything he can to make vaccines less available, less affordable, and more feared.”
Other experts said the decision was made without transparency and had little scientific backing. It comes at a time when more Americans are refusing vaccines; in Pennsylvania kindergarteners’ measles vaccination rates have dipped below the critical 95% threshold required to prevent the disease from spreading widely.
The Infectious Disease Society of America called the move “the latest reckless step in Secretary Kennedy’s assault on the national vaccine infrastructure that has saved millions of lives.”
Ronald G. Nahass, a New Jersey-based physician and IDSA’s president, said in a statement that Kennedy’s actions “put families and communities at risk and will make America sicker.”
The American Academy of Pediatrics, a leading professional medical society, said it would continue to recommend that all children be vaccinated against rotavirus, hepatitis, and other diseases removed from the CDC’s routine immunization list.
Under the new guidelines, the CDC will continue to recommend that all children get vaccinated for diphtheria, tetanus, whooping cough or pertussis, haemophilus influenzae type b, pneumococcal conjugate, polio, measles, mumps, rubella, human papillomavirus or HPV, and chickenpox.
The agency will also recommend that children at high risk for serious complications receive vaccines for respiratory syncytial virus (RSV), hepatitis A, hepatitis B, dengue, and two meningococcal diseases.
Previously, an independent committee that advises the agency in November recommended delaying hepatitis B vaccines for newborns.
“This framework empowers parents and physicians to make individualized decisions based on risk, while maintaining strong protection against serious disease,” said Mehmet Oz, a physician and administrator of the Centers for Medicare & Medicaid Services, in a statement.
Federal officials said that insurance will continue to cover vaccinations, the Associated Press reported.
President Donald Trump is joined by Health and Human Services Secretary Robert F. Kennedy Jr., left, and Centers for Medicare & Medicaid Services administrator Dr. Mehmet Oz in the Roosevelt Room of the White House in September.
Vaccine policy around the world
Offit spent 26 years developing a rotavirus vaccine after treating children with the illness during his medical residency in Pittsburgh — including one patient who died. Rotavirus causes vomiting and diarrhea that can lead to dehydration and is particularly dangerous for young children. There are two vaccines available, one of which Offit helped to develop.
“I try not to take this personally,” he said of the new federal guidance.
“But what we hadn’t eliminated was the virus,” he said.
HHS officials said that their review of worldwide vaccination policies found that the United States vaccinates for more diseases than other developed countries.
But, they said, many countries that recommend fewer vaccines still achieve “strong child health outcomes” and “maintain high vaccination rates through public trust and education rather than mandates.”
Denmark may have better health outcomes, but it also has a national healthcare system, a lower childhood poverty level, and free childcare, Offit noted in a recent blog post.
And, he said, Denmark — which does not recommend routine rotavirus or RSV vaccination — sees children hospitalized from those viruses at higher rates than the United States.
“Denmark is nothing to emulate. They should be emulating us,” Offit said.
Likewise, AAP president Andrew Racine said in a statement that America is a “unique country” with different health risks and public health infrastructure than Denmark.
“This is no way to make our country healthier,” Racine said.
Pennsylvania Gov. Josh Shapiro said that the state will “continue to rely on evidence-based guidance” including vaccine recommendations from the AAP.
“RFK Jr. is once again trying to sow chaos and confusion among parents — but know this: these changes at the federal level do not affect Pennsylvanians’ access to vaccines in our Commonwealth,“ he said in a statement. ”Pennsylvanians should continue to consult with their doctors and make informed decisions based on the best scientific evidence.”
New Jersey’s Acting Health Commissioner Jeffrey A. Brown said in a statement that the state sets vaccine requirements for school and childcare, and that those have not changed despite shifts at the federal level. He added vaccines in the state remain covered by insurance and the state is committed to protecting residents’ health.
“Federal efforts to reduce the number of vaccines recommended for all children in the United States are not supported by the available data nor the consensus of public health and medical experts,” Brown said. “Instead, deterring participation in vaccination risks leaving children vulnerable to serious and preventable infections.”
Changing public attitudes
In a December survey, the Annenberg Public Policy Center at the University of Pennsylvania found that more than a third of 1,006 Americans polled were more likely to trust the American Medical Association, a leading professional medical society, over the CDC if the two conflicted on vaccine policy.
At the time of the survey, the CDC had recently changed its website to suggest — against decades of evidence showing otherwise — that there could be a link between vaccines and autism.
Asking the public to make their own decisions on whether to vaccinate their children can make people vulnerable to misinformation, Annenberg director Kathleen Hall Jamieson said in an interview with The Inquirer last week.
“The public doesn’t have time to do research on its own, on average, and in the process, they can get lost in a mire of misinformation and confusion very easily,” she said. “It’s easy to think one is doing one’s research when one is way down the rabbit hole.”
In the poll, the preference to trust the AMA over the CDC held true across political parties and was particularly pronounced among older Americans. The only age group more likely to accept the CDC over the AMA in the event of conflicting vaccine advice was 18- to 29-year-olds.
“The fact that, as the CDC began to change statements, the public shifted its trust to other organizations on consequential issues — that’s a statement that says the public intelligence is real,” Jamieson said.
The AAP’s Racine reiterated Monday that the society will continue to publish its own vaccine recommendations and help physicians to advise parents.
“Your child’s pediatrician has the medical training, special knowledge, and scientific evidence about how to support children’s health, safety, and well-being. Working together, you can make informed decisions about what’s best for your child,” Racine said.
Offit cautioned parents against avoiding vaccinations, as high rates do not just protect healthy children — they’re also vital for children with immune disorders who cannot be vaccinated.
And, he said, parents shouldn’t discount the risks of hospitalization or death from vaccine-preventable diseases.
“There’s this sort of myth of invulnerability — you never think it’s going to happen to you, until it happens to you,” he said.
After a year of major shifts in the federal government’s policy toward vaccines, Americans are now more likely to trust the American Medical Association than the Centers for Disease Control and Prevention when the two conflict on vaccine guidance, a new survey shows.
Trump’s secretary of health and human services, Robert F. Kennedy Jr., is a longtime anti-vaccine activist. Earlier in 2025, he fired a committee of outside experts who advise the CDC on vaccine policy, replacing the committee with a handpicked group that includes other vaccine critics.
The reconstituted panel subsequently changed recommendations on who should receive COVID-19 vaccines, prompting states like Pennsylvania to change their own policies around vaccine distribution to ensure continued access. The panel also recommended delaying hepatitis B shots for newborns, prompting outrage from medical experts who said the move will increase cases of the serious liver disease.
And in November, the CDC website, which for years had noted that decades of research showed no link between receiving vaccines and developing autism, was updated to state the opposite. The site now reads: “The claim ‘vaccines do not cause autism’ is not an evidence-based claim because studies have not ruled out the possibility that infant vaccines cause autism.”
In the wake of those decisions, it is crucial for medical providers and health communicators to understand how the public views vaccination, said Kathleen Hall Jamieson, Annenberg’s director.
Kennedy’s guidance often encourages patients to make their own decisions with doctors about vaccines, she said. But that often puts the burden on Americans to process scientific research on their own — and makes them vulnerable to misinformation, she said.
“The public doesn’t have time to do research on its own, on average, and in the process, they can get lost in a mire of misinformation and confusion very easily. It requires a skill set to navigate scholarly literature. And it’s easy to think one is doing one’s research when one is way down the rabbit hole,” Jamieson said.
Autism, vaccines, and trust in the CDC
Annenberg researchers wanted to understand where the public is turning for information on vaccines as trust in the CDC has fallen.
Shortly after the CDC changed its website on vaccines and autism, Annenberg researchers asked 1,006 adults about what they would do if the CDC’s advice conflicted with that of a major medical professional organization like the AMA, which strongly condemned the website changes.
While about half of the respondents said they believe the CDC provides trustworthy information on vaccine safety, the survey found that 35% of respondents said they would be more likely to accept recommendations from the AMA if they conflicted with the CDC. Just 16% of respondents said they would side with the CDC in that case.
That preference held true across political parties and was particularly pronounced among older Americans. The only age group more likely to accept the CDC over the AMA was 18- to 29-year-olds: 24% said they would accept the CDC’s recommendations, and 19% said they would accept the AMA’s.
“The fact that, as the CDC began to change statements, the public shifted its trust to other organizations on consequential issues — that’s a statement that says the public intelligence is real,” Jamieson said.
“The public is paying enough attention to say, ‘I can’t necessarily go to the CDC on that topic.’ That’s a statement that says we’re in better shape than you might have guessed that we were.”
Gauging public knowledge on vaccines
In another series of surveys, Annenberg researchers gauged what Americans already know about common vaccines in order to help public health officials communicate with the public more effectively.
“One of the goals of our surveying is to find what kinds of knowledge the public finds helpful and increase the likelihood that people make science-consistent decisions,” Jamieson said.
A survey on whooping cough, also known as pertussis, was conducted in the fall in response to a national rise in cases. The disease is caused by a bacterial infection and can result in a severe cough that lasts for months. It is particularly dangerous for infants, especially those too young to be vaccinated against the disease.
About 30% of 1,637 respondents said they were not sure whether pertussis was the same as whooping cough and 35% said they were not sure whether a vaccine exists for it. Annenberg had reported similar findings a year before — an alarming conclusion, researchers said, because health officials have blamed a rise in cases in part on decreasing vaccination rates.
“Maybe we’re not doing the best possible job in communicating what we know about relative risks of the disease, the relative risks of vaccine, and the ways in which whooping cough is transmitted,” Jamieson said. “These are all questions designed to figure out the equation people are working through.”
Support for measles, mumps, and rubella vaccine
Likewise, a late-fall survey on attitudes toward the measles, mumps, and rubella vaccine (MMR) found that 86% of respondents said they would be likely to recommend that eligible people in their household get the MMR vaccine.
That is a “small but significant” decline from last year, when 90% said they would recommend the vaccine, researchers said.
Respondents are now also less likely to recommend vaccines for HPV and polio.
That may be because the MMR vaccine has been so effective that the public can no longer remember what it was like to contract measles, Jamieson said.
“I am elderly. I have gone through whole periods of my life in which these vaccines did not exist. I know what measles looks like — extraordinarily uncomfortable — with risks that are real and demonstrable,” Jamieson said. “And the vaccine has worked for people I care about in the subsequent generations.”
Support for MMR vaccines is still overwhelmingly high, Jamieson said. But the threshold to maintain herd immunity for measles is also high — about 95% of people must be vaccinated in order to prevent the spread of the disease and protect people who cannot be vaccinated.
And, if people live in communities where vaccines are less accepted, they could be at higher risk than the general population.
“The state of Pennsylvania can be at 95%, but if my church isn’t at 95%, I can get measles if I’ve not been fully immunized or if I can’t be vaccinated,” Jamieson said.
Philadelphia is on track to record the lowest number of fatal overdoses in nearly a decade in 2025, according to preliminary state data.
State officials reported 747 overdose deaths in the city as of Dec. 23. The city last recorded fewer than1,000 deaths in 2016, when 907 people died of overdoses.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Likewise, overdose deaths are dropping in Pennsylvania, with a 29% decline in deaths reported statewide between 2023 and 2024, according to preliminary data from the state.
Preliminary data for 2025 indicate that deaths are also on track to decline again across the state, with 2,178 overdoses reported as of Dec. 23, according to state data. In all of 2024, the state recorded 3,340 overdose deaths.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
City officials in Philadelphia said there are slight differences in how the state and the city report overdose data and could not comment extensively on the state figures. But the city’s own data also show dramatic drops in deaths in the last several years.
As recently as 2022, deaths in the city had soared to their highest-ever rate. But they decreased slightly in 2023.
Citing preliminary data from 2024, Philly Stat 360, a city-run database that tracks quality-of-life metrics, reported 1,064 overdose deaths — a 19% decrease in fatal overdoses from the year before. The city has not yet released its own statistics for 2025.
“My first reaction to hearing these numbers is absolute joy,” said Keli McLoyd, the director of the Philadelphia Overdose Response Unit (ORU). “With that said, the number should be zero. Every overdose is preventable. Every single one of those lives lost is a person.”
State officials said their work to expand overdose prevention efforts and ease entry to treatment has contributed to the dramatic drops in deaths. Still, they said, there is more work to be done.
“Even with the overall decreases, we are still losing too many people — mothers, fathers, sons, daughters, grandparents, grandchildren — to overdose,” said Stephany Dugan, a spokesperson for the Pennsylvania Department of Drug and Alcohol Programs.
She added that all Pennsylvanians “deserve equal and equitable access” to addiction treatment.
Decreases in overdoses in Philadelphia
Discerning the cause of the dramatic drops in overdose deaths can be difficult, city officials say.
“We have to acknowledge that it’s a huge, huge change, and so we really are hopefully doing something right. But I think it’s going to be very hard, if not impossible, to say that one thing resulted in this massive reduction in fatal overdose deaths,” McLoyd said.
Still, efforts at the state and local levels to increase access to naloxone, the overdose-reversing drug, likely made a difference, she said.
A number of local advocates in the addiction medicine field have speculated that there is still much to learn about how the COVID-19 pandemic affected overdose rates, said Daniel Teixeira da Silva, the director of the Division of Substance Use Prevention and Harm Reduction at the Philadelphia Department of Public Health.
“When we look at the [overdose] increases after 2016, leading up to COVID, we can tie that to the introduction of fentanyl to the [drug] supply,” he said Monday, referring to the synthetic opioid behind most of the city’s fatal overdoses.
“When you look at the increases from 2020 to 2022 — this is where I just don’t think we know enough yet. It’s hard to say COVID didn’t impact [deaths]. We look at what was going on at the time, contributors to more risky substance use such as people losing employment, the isolation,” Teixeira da Silva said.
Likewise, he said, policy changes that came about during the pandemic, such as easing some restrictions around opioid addiction medications, could be contributing to a drop in deaths now.
“Maybe we’re seeing benefits of the policies enacted during COVID,” he said.
A changing drug landscape
On Philly Stat 360, city officials said fentanyl still drives nearly all of the opioid overdose deaths in the city.
But about 70% of deaths involved a stimulant like cocaine or methamphetamine in 2024. And about half of the city’s fatal overdoses that year involved both stimulants and opioids.
Taking stock of the drop in overdose deaths, city officials noted the success of a 2024 program at the ORU to deliver naloxone, the opioid overdose-reversing drug sold under the brand name Narcan, to households in neighborhoods seeing a high number of overdoses.
They included neighborhoods in North Philadelphia, where overdose deaths had risen over the last several years. Across the city, Black and Hispanic communities had seen high rises in overdoses — but neighbors often reported receiving fewer resources to address them.
Workers assigned to the naloxone initiative knocked on 100,000 doors offering the medication and access to addiction treatment. In some neighborhoods, up to 88% of neighbors who answered their doors accepted some kind of resource from staffers, according to a city report on the program. McLoyd also helmed an effort to ensure all city fire stations had naloxone on hand.
“We’re sharing those messages that this is a tool for everyone, not just people who use drugs or people who love those who use drugs,” since some people may hide their addiction from others, she said.
This year, the city launched another campaign to educate residents about the risk of heart disease from stimulant use. Eighty percent of overdose deaths among Black Philadelphians in 2023 involved a stimulant, and about half of the Black Philadelphians who died of an overdose between 2019 and 2022 had a history of cardiovascular disease.
“We see opioid-stimulant [overdose deaths] decreasing, but stimulant-only [overdoses] being really persistent,” Teixeira da Silva said. “Stimulant overdoses are not reversed by Narcan,” so it is important to help vulnerable residents understand the specific harms caused by stimulants.
As overdoses decrease in the general population, McLoyd said, it is crucial to maintain outreach efforts toward groups that have seen rising overdoses in recent years, like pregnant people and teens in the juvenile justice system.
“Within certain populations, overdoses are still disproportionately high. We want to develop programs that speak specifically to those populations,” she said.
City officials have also hailed the Riverview Wellness Center, a 234-bed recovery home that offers supportive services to people who have completed a 30-day stay in inpatient treatment.
But Mayor Cherelle L. Parker’s administration has faced criticism from advocates for people in addiction over her decision last yearto slash funding for syringe exchanges. Critics have also decried City Council legislation that regulates mobile medical services for people with addiction, requiring permits to offer care and limiting operating hours and locations in some neighborhoods.
Teixeira da Silva said that the city is using the legislation to more effectively coordinate care for people with addiction. He said his division has been involved in the new permitting process for mobile services to “get them approved as fast as possible to ensure there isn’t a gap in access.”
Statewide initiatives
Across Pennsylvania, the state’s Overdose Prevention Program handed out more than 415,000 doses of naloxone in the first six months of 2025, said Dugan, the Pennsylvania Department of Drug and Alcohol Programs spokesperson.
Those doses helped reverse more than 6,100 overdoses, Dugan said earlier this month.
The state also distributed 437,000 test strips to help drug users detect fentanyl and xylazine. The animal tranquilizer contaminated much of Philadelphia’s illicit opioid supply starting at the beginning of the decade and can cause severe skin wounds that sometimes lead to amputation.
Authorities credited efforts to increase access to treatment in rural counties and to decrease wait times for addiction treatment, implementing a “warm handoff” program that allows patients to transfer directly from hospitals to addiction treatment.
More than 22,000 Pennsylvanians were offered addiction treatment from hospitals in the first 10 months of 2025. Nearly 60% of people who received referrals accepted them, state officials said.
Advocates say that the state’s focus on programs to prevent overdoses has paid off.
“I’m really impressed and grateful for the state and their investment in harm-reduction programs,” said Sarah Laurel, who heads the Philadelphia-based addiction outreach organization Savage Sisters.
But as the drug supply changes, she said, it is vital for health officials to collect more data on other harms of drug use besides overdoses.
For example, medetomidine, another powerful animal tranquilizer not approved for human use, has supplanted xylazine in Philadelphia’s illicit opioid supply.
It causes intense withdrawal that has flooded emergency rooms with patients suffering from dangerous spikes in blood pressure and other heart complications. Some doctors have raised concerns that patients undergoing medetomidine withdrawal risk brain damage from high blood pressure.
Medetomidine was detected in about 15% of all fatal overdoses in Philadelphia between May 2024 and May 2025, according to preliminary city data obtained by The Inquirer this fall.
“It’s great they’re distributing naloxone at the rate they are. However, we have not really seen a ton of data on the complications that this polychemical substance wave is causing for people,” Laurel said.
“It’s a big area where we can look into the people we’re serving and the way their lives are being impacted by drugs.”
Teixeira da Silva said that city officials successfully pushed federal officials this fall to institute new medical billing codes for xylazine use and related amputations, a crucial step to allow hospitals to better track harms from the drug. They are hoping to do the same for medetomidine and its withdrawal symptoms.
“I definitely agree that we need a broader perspective in terms of the harms caused by drug use beyond death,” he said. “Of course, death is the worst harm. That has to be a metric that we continue to monitor and work toward zero.”
Philadelphia is suing a host of drug manufacturers and pharmacy benefit managers in federal court, alleging that they conspired to increase insulin prices to drive sky-high profits as patients struggled to afford life-saving medications.
City officials said rising diabetes medication prices have caused the city to “significantly overpay” for diabetes medication for city employees and their families, noting in a news release that insulin prices have increased from $20 per vial in the 1990s to $300 to $700 per vial today.
About 14% of adults in Philadelphia have diabetes, the city said.
“Philadelphia suffers from one of the highest rates of diabetes in the United States, especially in our Black and brown communities,” Health Commissioner Palak Raval-Nelson said in a statement.
“When people cannot afford their insulin, they frequently go without or cut back, leading to disastrous consequences both for themselves and Philadelphia as a whole. Their lives are degraded, and we all pay the associated health costs.”
The suit, filed Tuesday, follows similar litigation filed by District Attorney Larry Krasner in 2024. Hundreds of companies, unions, and other local and state governments, including Bucks County, have also filed suit alongside Philadelphia as part of a wide-ranging lawsuit in federal court in New Jersey, the city said.
In the suit, the city accuses drugmakers and pharmacy benefit managers, or PBMs, of colluding to drive up profits on diabetes drugs. PBMs work with drug manufacturers, insurers, and pharmacies, negotiating prices and developing formularies — lists of prescription drugs that are available on a given insurance plan.
To ensure their drugs were included on formularies, drug manufacturers increased prices on diabetes drugs and then paid “a significant, yet undisclosed” portion of the resulting profits back to the PBMs, the city’s lawsuit said.
That meant lower-priced or generic diabetes medications received “less favorable placement” on formularies, passing higher costs onto consumers, according to the lawsuit.
The suit names nearly two dozen prominent drugmakers and PBMs, including Eli Lilly & Co., Optum RX, Sanofi, Novo Nordisk, and CVS Caremark. Optum officials did not immediately return a request for comment.
In a statement, a Lilly spokesperson said the company has worked for years to lower costs for people with diabetes by capping prices at $35 per month. The average out-of-pocket Lilly insulin cost was $14.86 a month for patients in 2024, the spokesperson said.
“These copycat lawsuits are baseless,” the spokesperson wrote.
Sanofi officials declined to comment on the allegations but said in a statement their “pricing practices have always complied with the law.” The company said it works to lower costs for patients, but that in the U.S. healthcare system, “savings negotiated by health insurance companies and PBMs” aren’t often reflected in patients’ co-pays.
CVS officials said in an email that “pharmaceutical companies alone” are responsible for setting insulin prices and that they would welcome efforts from drug manufacturers to lower prices.
“Allegations that we play any role in determining the prices charged by manufacturers for their products are false, and we intend to vigorously defend against this baseless suit,“ officials said.
Novo Nordisk officials similarly called the allegations in the suit “meritless” and said the company has a number of initiatives to make insulin more affordable for patients.
Staff writer Sarah Gantz contributed to this article.
Recovery Centers of America, a prominent addiction rehab provider, will pay $2 million to settle claims by the federal government that it illegally dispensed strictly regulated medications and billed Medicaid for services it did not provide.
The DEA said RCA “dispensed controlled substances in an unlawful matter” and did not comply with federal recordkeeping rules for drugs and other substances that are closely regulated due to their potential for abuse.
Federal officials did not specify the controlled substances involved.
In a settlement agreement, federal authorities said that the DEA found a number of recordkeeping issues at an RCA facility in Devon, including that the facility did not maintain records showing that it had received controlled substances, and did not record the number of containers of the substances or the date they had been received. Some prescriptions for controlled substances were issued to “house stock” instead of named patients, authorities said.
The facility also did not keep accurate records of the controlled substances on hand at the site, authorities allege.
They also found recordkeeping issues at another RCA facility in Maryland.
In 2017, a whistleblower who was once employed at RCA filed a lawsuit alleging that some facilities had admitted patients on Medicaid, but had not complied with state and federal regulations on providing them with rehab services.
Under federal law, whistleblowers can sue on behalf of the government when they believe a company has submitted false claims for government funding, federal authorities said.
Federal authorities said that between 2017 and 2019, some RCA facilities billed the Federal Employees Health Benefits Program and Medicaid for care that they did not document and did not actually provide.
The settlement will resolve the whistleblower’s lawsuit.
RCA did not immediately return a request for comment.
The company has agreed to pay $1 million to resolve the controlled substance claims and $1 million to resolve the billing claims. RCA did not admit liability as part of the settlement agreement.
Federal law also enables whistleblowers to receive money from the settlement. The former employee will receive $230,000, authorities said.
RCA will also pay the employee $450,000 and $75,000 to cover attorney’s fees, according to the settlement agreement.
“Drug and alcohol treatment facilities must prescribe and store controlled substances in a manner that comports with rules designed to ensure that dangerous drugs do not fall into the wrong hands. They also must provide treatment services that comply with all governing laws and regulations,” U.S. Attorney David Metcalf said in a statement.
“When they fail in either of those critical duties they will face significant consequences.”
In Philadelphia, the city where the hepatitis B vaccine was discovered, experts sharply criticized a decision on Friday by the nation’s leading vaccine advisory panel to end a longstanding recommendation that all infants be immunized at birth against the serious liver disease.
The Advisory Committee on Immunization Practices, a committee that makes recommendations to the Centers for Disease Control and Prevention on the vaccines that Americans should receive, voted 8-3 to change its guidance on when and to whom the hepatitis B vaccine should be administered.
National medical professional societies have opposed changes to the administration of a vaccine proven to be safe and effective, crediting it with all but eliminating the spread of the virus in young children.
The hepatitis B vaccine revisions underscored growing concern that the federal government’s vaccine guidance is no longer credible under President Donald Trump’s administration.
“Cases will go up,” said Sarah Long, an infectious disease pediatrician and a professor of pediatrics at Drexel University’s College of Medicine.
She called the vote “outrageous,” saying it’s much safer to ensure every child gets protection as soon as possible from a virus that can have lifelong effects, causing in some people cirrhosis and liver cancer.
“Why wouldn’t you want to apply a cancer-preventing vaccine to every potential susceptible child?” Long said.
Long is herself a former member of the committee of independent experts. Her term ended in July 2024, about a year before Health and Human Services Secretary Robert F. Kennedy Jr. fired all of ACIP’s 17 members and reappointed handpicked members that included some who, like Kennedy, have advocated against vaccines.
At meetings on Thursday and Friday, the committee reviewed a recommendation in place since 1991: that, shortly after birth, infants receive the first in a series of hepatitis B vaccinations.
ACIP will now recommend that infants receive a hepatitis B shot at birth only if their mother was not tested or tests positive for hepatitis B.
Parents can still decide with their doctors to give a dose at birth if the baby’s mother tests negative.
The committee recommended delaying the shot, recommending that babies should get their first hepatitis dose at “no earlier” than two months if they do not receive a birth dose.
Parents who test negative for the virus should discuss “vaccine benefits, vaccine risks, and infection risks” with their doctors to decide “when or if their child will begin the hepatitis B vaccine series,” HHS officials wrote in a statement.
Some committee members said most babies are not at high risk for infection and questioned whether there’s adequate research to support the shots for infants, The Associated Press reported. But two others said there was no evidence that birth doses harm babies. The CDC’s own website cites decades of studies showing few risks from the vaccine.
‘Why wait until two months?’
The decision makes little sense, said Paul Offit, a nationally renowned vaccine expert and physician who leads Children’s Hospital of Philadelphia’s Vaccine Education Center and has often clashed with Kennedy.
“I don’t think this RFK Jr.-appointed anti-vaccine group calling itself the ACIP understands critical aspects of this virus,” he said. “This vaccine is as safe at two months as it is at birth. Why wait until two months?”
It’s dangerous to wait to vaccinate babies against hepatitis B because the virus is highly contagious and can spread from a mother to a child at birth, and through actions as seemingly innocuous as sharing a toothbrush, a washcloth, or a razor.
Pennsylvania has seen a 95% reduction in acute hepatitis B cases since the birth dose was implemented, health officials said in a news release earlier this week, calling transmission to newborns, infants, and toddlers “nearly eliminated.”
Across the state, no mothers have passed the disease to their children at birth since 2019, and no cases have been detected in children under 4 since 2007.
State health officials had urged the committee to keep the birth dose recommendation.
Secretary of Health and Human Services Robert F. Kennedy Jr. at a November meeting of the Western Governors’ Association in Scottsdale, Ariz.
Public perceptions of the vaccine
Most Americans support hepatitis B vaccinations for newborns, a recent study from the University of Pennsylvania’s Annenberg Public Policy Center found.
The center surveyed 1,637 Americans last month, noting that the CDC recommended that all children be vaccinated for hepatitis B at birth, and three-fourths of respondents said they were very likely or somewhat likely to recommend the vaccine for a newborn in their household.
Though a majority of survey respondents across political parties said they were likely to recommend the vaccine, Republicans were least likely to recommend it.
About 40% of respondents correctly answered a question about the disease the hepatitis B vaccine prevents. One-third said they were not sure what disease it prevents.
Next steps
ACIP’s recommendations must be adopted by the CDC director. The White House fired former CDC director Susan Monarez this summer, in part because she had refused to unquestioningly sign off on ACIP recommendations.
In her place, the acting director, Jim O’Neill, will decide whether to adopt the new recommendations.
Pennsylvania and New Jersey are among the states that have moved this year to ensure residents can continue to access vaccines amid the reconstituted panel’s earlier controversial changes to the vaccine schedule.
In Pennsylvania, Gov. Josh Shapiro signed an executive order in October aimed at protecting access to vaccines. One of its directives asks the state Department of Insurance to require that insurance companies cover vaccines recommended by leading national medical associations, including the American Academy of Pediatrics, which continues to recommend hepatitis B vaccines at birth.
In a statement after Friday’s vote, Pennsylvania’s Secretary of Human Services, Val Arkoosh, urged doctors and parents to follow AAP recommendations when vaccinating infants.
And the state’s insurance commissioner, Michael Humphreys, said that insurers in the state will continue to cover the vaccine for newborns, “full stop.” He added insurers have already committed to covering birth doses through at least 2026, and that the department expects insurers to continue their coverage beyond that date.
In a post on X, the social media platform formerly known as Twitter, Shapiro criticized Friday’s decision as “threatening access to safe, effective Hepatitis B vaccines for newborns, putting them at risk of getting a serious infection with lifelong consequences.”
In New Jersey, insurance companies are expected to continue to cover all immunizations recommended by the state health department, which includes birth doses of the hepatitis B vaccine, the state Department of Banking and Insurance said in a statement after the committee’s vote.
The department’s commissioner, Justin Zimmerman, said the federal government is “taking actions that threaten the health of residents.”
CHOP’s Offit said he believed most doctors will continue to recommend the birth dose.
“Doctors will know this is a bad idea and will do what they’re always doing — recommend the birth dose,” he said.
But he and Drexel’s Long are among the experts increasingly concerned about the confusion ACIP’s decision could sow.
And the decision from one of the nation’s highest-profile public health authorities could push more people to forgo the vaccine, Offit said.
“I think people will feel empowered to say, ‘I don’t want this vaccine because ACIP said I don’t have to get it,” he said.
Kelly Wyatt winced as a nurse unwrapped layers of gauze from her left leg, exposing the massive wound beneath.
Yellow and red and gray, weeping plasma and agonizingly painful at the slightest touch, it covered almost the entirety of the end of her leg — the site of the amputation she had undergone four years before.
Emergency room doctors at the time had warned her that if the drugs she was using didn’t kill her, her wounds would.
Now Wyatt is 14 months into recovery from an addiction to fentanyl, a potent synthetic opioid, and xylazine, an animal tranquilizer never approved for human use. The emergence of xylazine, known as “tranq” on the streets, early in the decade marked the beginning of a dangerous new era for Philadelphians addicted to illicit opioids.
Wyatt, 52, is among hundreds of Philadelphians facing lifelong medical needs from tranq, as the latest wave of the area’s drug crisis has seen a rapidly evolving succession of veterinary and industrial chemicals compound the dangers of the powerful opioids being sold on the streets.
Some have become regular patients in burn units and wound care clinics at area hospitals, among the only places capable of treating severe tranq injuries.
As part of its ongoing coverage of the area’s drug crisis, The Inquirer followed Wyatt for more than a year as she went through early recovery and worked with doctors to heal her wound.
Kelly Wyatt receives treatment at Jefferson Einstein Philadelphia Hospital’s Center for Wound Healing in Philadelphia in November.
Wyatt initially shrugged when the small sores had emerged on her legs, only to watch them grow into massive abscesses, resulting in an amputation below her knee. Her ongoing tranq use prevented the wound on her left leg from healing properly. Even after recent months of sobriety and careful treatment, doctors are still warning her that they may have to amputate more of her leg.
But Wyatt’s tranq wounds go still deeper.
Over the last several years, both of her sons had spiraled into addiction. By January, both of them were dead.
A family photo of Dakota Wyatt, left, and Tyler, right.
Spiraling into addiction
Several members of Wyatt’s family have struggled with addiction.
Wyatt experimented with drugs as a teenager, but was sober during her kids’ early childhoods. She didn’t drink alcohol, let alone seek out illicit drugs, after giving birth to her eldest son, Dakota, at 18. She raised two sons and a daughter in a neighborhood near Pennypack Park.
Her days had a familiar rhythm: packing lunches, picking the kids up from school, watching them play together at the local park. In her spare time, she dabbled in mixed-media art, designing the window displays at the downtown restaurant where she worked for years. One Philadelphia Flower Show-themed display had a working waterfall.
Her youngest, Tyler, was a happy child, grinning wide in every school picture and sharing inside jokes and a love for music with his brother. Dakota, more sensitive, had struggled with anxiety from an early age; Wyatt remembers him asking her at bedtime what the family would do if their house burned down in the night. But he could always make her laugh, and she and the boys would sing along to the same music in the car: ’90s alt-rock, Johnny Cash, the local hip-hop station.
In 1999, she divorced their father. A few years later, at 28, she took her first Percocet pill, an opioid painkiller approved for medical use that is widely abused as a street drug.She had just started working at a bar, and the long hours were wearing on her.
With the pills, “I could get more cleaning done, I could push my body more,” she said. “And it snowballed.”
She was not aware when her sons began using drugs themselves in their teenage years. “I didn’t know for a long, long time,” she said.
Afterward, Wyatt tried to help them seek treatment, even while her own drug use increased, she said.
But a series of traumatic life events resulted in all falling deeper into addiction together.
Wyatt’s ex-husband died following long-standing health issues, including diabetes.
Then Dakota, who drove a Zamboni at a local ice rink, was injured in an accident at work — losing the tips of his fingers while cleaning the machine. He had been using more opioids to deal with the pain.
Wyatt began buying drugs with him in Kensington, at the vast open-air drug market that is the epicenter of Philadelphia’s opioid crisis. “It was normalizing — I’m his mom and I’m with him in that crazy environment. I’m sure it made him feel like it was OK. And I regret that,” Wyatt said.
“I regret a lot of stuff. But that was the beginning.”
Kelly Wyatt leaves her wound care appointment at Jefferson Einstein Philadelphia Hospital’s Center for Wound Healing in November.
Tranq warning signs
It was the mid-2010s, and the drugs on the street were changing. The stronger synthetic opioid fentanyl was just emerging; dealers chanted “fetty-fetty-fetty” on the corners to draw in customers.
And then Wyatt began hearing talk of “tranq” getting mixed into the drug supply.
That was around the time that Dakota developed wounds on his arm, open sores that would not close. Wyatt found small wounds on her arms and legs — “like melon-ball scoops.”
One day, she saw a flier, handed out by health authorities in Kensington, warning that tranq can cause skin lesions.
“All of a sudden,” she recalled, “things made sense.”
But her addiction was so severe that she was afraid to stop using the fentanyl-tranq mix now prevalent in the illicit drug market. She fixated on avoiding xylazine’s severe withdrawal symptoms — chills, sweating, anxiety, and agitation — which don’t respond to traditional opioid withdrawal medications. She worried about seeking treatment with no guarantee of relief.
By the time Wyatt was admitted to a hospital in 2021, she was hallucinating from sepsis, a severe complication from an infection that can lead to organ failure, shock, and death.
When she woke up eight days later, a doctor told her she was at risk of having one leg amputated, and maybe both. “Please let me keep as much of my leg as possible,” she recalls begging a doctor who wanted to remove her entire leg.
Kelly Wyatt receives treatment for a serious xylazine wound at the site of her amputation at Jefferson Einstein Philadelphia Hospital’s Center for Wound Healing in November.
“The doctor thought I should get the whole leg cut off. The other thing I could do was amputate below the knee, and then get tons of operations for the infection,” she said.
Her oldest son’s tranq wounds had also worsened. Dakota had wounds on his legs and an arm, which was eventually amputated later that year. He also suffered a heart infection linked to his drug use, and needed a valve replacement.
After a month in the hospital, he came home and continued using drugs.
He developed new lesions. Maggots ate at his rotting skin. Wyatt cleaned the bugs out of his wounds.
Wyatt tried bargaining with her son, promising they could get addiction treatment together. She offered to get him enough drugs that he wouldn’t enter withdrawal while waiting for care at the hospital. Sometimes, he managed to stay at the hospital for a few hours, but never longer.
“He was too embarrassed to go anywhere, he was too afraid to get clean, and he was too afraid to be sick. He told us he would rather die than go through withdrawal again,” she said. “A couple times, he asked me if I wanted to just shoot up and lay down and die with him.”
“‘I want to live,’” she recalls telling him, “‘and I don’t want to live without you.’”
Kelly Wyatt waits for treatment for a serious wound on her leg at Jefferson Einstein Philadelphia Hospital’s Center for Wound Healing in November.
Loss and recovery
One night in January 2024, Dakota was having trouble breathing and seemed to be hallucinating, speaking nonsense. He asked Wyatt to call an ambulance to the house.
Dakota died before the family reached the hospital. His cause of death was listed as drug intoxication.
Wyatt believes ongoing health issues from his wounds hastened his death. Her grief intensified her own drug use, leading to more xylazine wounds. The wound that had opened near her amputation grew worse.
A month after Dakota’s death, she entered drug treatment. After three months, she relapsed and overdosed on cocaine and fentanyl. Her first thought after waking up was to use again, but instead she chose rehab.
“I didn’t want to die,” Wyatt said. “I didn’t want to be in pain anymore.”
She arrived at the Behavioral Wellness Center at Girard in July 2024, hoping to enter outpatient rehab.
Instead, physicians recommended their inpatient clinic that could also treat her wounds, one of the few such facilities in Philadelphia.
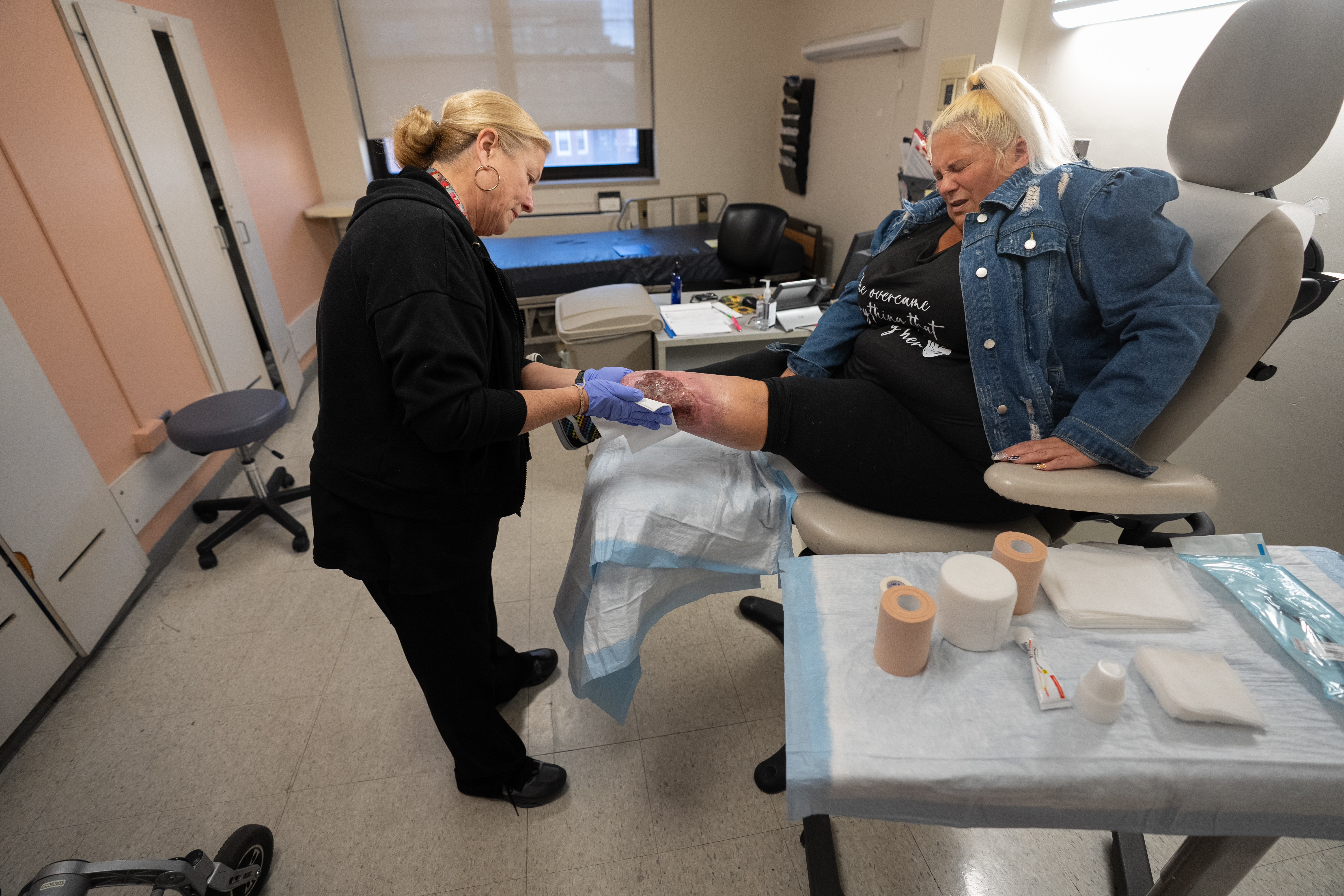
In August 2024, Kelly Wyatt attended a wound care appointment as part of her inpatient care at Girard Behavioral Health, one of a few addiction rehabs in the city that can treat xylazine wounds.
Wyatt was living there and undergoing treatment a month later, in August 2024, when she wheeled her motorized wheelchair into a clinic room and took deep breaths as nurses carefully peeled back layers of moisturized gauze on her left leg, cleaning the wound.
Still in the shaky early months of recovery, and needing to remain in inpatient rehab, she remained worried about Tyler, who was still using drugs.
“He was the primary caretaker of his brother. They would be in their room, getting high together. And now he’s just in that room by himself, day in and day out,” she said in an interview that summer.
“I kept saying, ‘I think I should go home to him.’ And everybody kept saying to me, ‘You have to work on yourself first. He’ll be fine,’” she later recalled.
“And then he wasn’t fine.”
Kelly Wyatt and her partner Randy Stewart at the headquarters of Resources for Human Development, which runs the skilled nursing and inpatient addiction treatment center where Wyatt sought treatment this winter.
A mother’s guilt
Wyatt was still in rehab in January 2025 when her partner, Randy Stewart, called. He hadn’t seen Tyler in hours and thought he might have left the family’s house.
Wyatt called several hospitals and then asked Randy to check the bathroom in the back of the house.
He found Tyler on the floor.
“I just thought, God, please no,” Wyatt said. “Not again. You can’t do this to me again.”
Tyler’s cause of death was also listed as “drug intoxication.”
He died at 27, a year and 10 days after his brother.
Wyatt is still wracked by guilt. Guilt that she used drugs with her sons. That she used drugs at all. That she wasn’t there when either of her boys died. That her daughter, who does not use drugs, stopped speaking to her. Sometimes, she dreams about her children and wakes up screaming.
As she continues treatment, Wyatt said, she hopes her story will help other families struggling with addiction, especially the realities of tranq use.
“Sometimes I’m embarrassed to talk about it. But I feel like I have to,” she said. “Because people need to know. If one person sees this and gets some medical care, gets any kind of help, I would be happy.”
Heidi Hunt, a wound care-certified registered nurse, cleans the wound on Kelly Wyatt’s leg at Jefferson Einstein Philadelphia Hospital’s Center for Wound Healing in November.
Treating tranq’s wounds
For Wyatt, maintaining her recovery from addiction and caring for her wounds are full-time occupations that sometimes are in conflict.
Methadone, the opioid addiction treatment drug that has helped Wyatt curb cravings for more than a year, can be dispensed only at special clinics.
Wyatt’s clinic journey meant three hours a day on a bus where she couldn’t keep her leg elevated. The wound worsened until she was able to switch to a closer methadone clinic.
Wyatt relies on Stewart to help her move around her home, where the only bathroom that she can access is the one where Tyler died.
“Cleaning, taking care of me, changing my wound dressings, talking about my sons — he calms me down. It’s been a lot, and he’s really done a lot,” she said.
Kelly Wyatt and her partner Randy Stewart in July.
Once a week, Wyatt travels to Jefferson Einstein Philadelphia Hospital’s Center for Wound Healing for wound care.
At a recent appointment, nurse practitioner Danielle Curran scraped away infected skin, measured the wounds, cleaned and re-bandaged her lesion.
In between office visits, nurses also go to her home to clean and re-bandage her wound twice weekly. Several times this year, Wyatt has undergone debridement surgery to remove more damaged skin under anesthesia.
If the treatments manage to shrink her wound, Curran said, Wyatt could try a skin graft and eventually receive a prosthetic leg that could help her get around more easily.
Curran has treated about 20 xylazine patients at the clinic over the last few years. About 10, including Wyatt, are still getting regular care. Others have relapsed and returned to the streets. Several have died of overdoses.
She is relieved that, as Philadelphia’s opioid crisis continues to evolve, tranq is becoming less prevalent. But it has been replaced in street drugs by another animal tranquilizer, medetomidine, which does not appear to cause flesh wounds but, rather, agonizing withdrawal symptoms. Skin lesions among opioid users have decreased in the last year.
Yet Curran still insists on seeing patients like Wyatt with xylazine wounds weekly, trying to help them through their injuries and hopefully their recovery, too. “I like to be another person holding them accountable, to stay on the path. We try to give them that support.”
Sometimes, that support means simply reminding Wyatt how far she has come in the four years since the amputation, and now 14 months of sobriety.
At a recent appointment, after carefully scraping dead skin away from Wyatt’s leg with a small curette, Curran walked through her next steps: A disinfecting gel to keep bacteria out of the wound. A course of antibiotics to avoid infection. Another debridement surgery, in a few weeks.
“As a rule of thumb,” Curran told a reporter, “it’s very hard to give timelines for wound care, because of all the things that could possibly go wrong. A wound this size, though? It could take years.”
Wyatt began to cry. “It’s already been four years,” she said.
Curran turned to her. “You’ve made so much progress,” she said gently. “Give yourself time.”
Kelly Wyatt enters the wound care clinic at Girard Behavioral Health in August 2024.
Editor’s note: This story has been updated to clarify the name of the Jefferson Health clinic where Kelly Wyatt received wound care.
In a small clinic room at Mother of Mercy House on Allegheny Avenue in Kensington, Emma Anderson unwrapped a bandage from a man’s swollen hand.
“It hurts really bad in the cold,” the man said, wincing at the inflamed wound that covered most of a right-hand finger.
Cleaning it with saline solution proved so painful that Anderson, an EMT and St. Joseph’s University student, let the patient take the lead, wiping carefully at the yellowish-white tissue at the center of the wound.
It was his second time attending the wound care clinic at Mother of Mercy, the Catholic nonprofit that twice a week opens its doors to people with addiction dealing with the serious skin lesions, caused by the animal tranquilizer xylazine, that can develop into wounds so severe the only treatment is amputation.
Called “tranq” on the streets, xylazine was never approved for human use and has wreaked havoc across the city since dealers began adding it to fentanyl to extend the opioid’s short-lived high.
In the five years since it emerged as a threat, amputations among opioid users have more than doubled. The Philadelphia drug supply is now changing again, and though emergency rooms in the last year have treated fewer xylazine wounds, the crisis is far from over.
The man who visited Mother of Mercy’s clinic on a recent Tuesday, who gave only his first name, Steven, because of the stigma surrounding drug use, noticed the alarming wound on his hand a few weeks ago.
Steven had seen people sleeping on the streets with flies hovering around their gaping wounds. He had hoped that he could avoid a wound himself: He smokes fentanyl, instead of injecting it, and knows that injection drug users are generally at a higher risk for skin infections. But, like many people who smoke their drugs, he had developed a wound anyway.
“Believe it or not,” Steven said, between deep breaths during the painful cleaning, “I actually was an EMT myself at one point.”
‘How did we let it get this bad?’
Mother of Mercy, founded in 2015 in Kensington, partners with St. Joseph’s Institute of Clinical Bioethics to host the clinics. The institute, headed byFather Peter Clark, a Jesuit priest and a bioethicist at several area hospitals, has long held a monthly health clinic at the nonprofit’s Kensington headquarters.
In the last year, they expanded the program to offer more wound care opportunities to a community increasingly in need of them.
Father Peter Clark, the director of the Institute of Clinical Bioethics at St. Joseph’s University, and Ean Hudak, a St. Joseph’s student and staffer at the Mother of Mercy House wound care clinic, assist a person who had fallen unconscious on Allegheny Avenue in Kensington.
“To be physically down here in the heart of it, and seeing it on a weekly, monthly basis, it opens your eyes. How did we let it get this bad?” said Steven Silver, the assistant director of research and development at St. Joseph’s, who was welcoming clients at the door on a recent clinic day.
The program is staffed by medical students and undergraduates, all trained in wound care. Many say the work they do at the clinic is unlike any medical training they’ve been offered at school.
Undergraduates like Anderson and Ean Hudak, who takes shifts at the clinic in between applying to nursing schools, say they’re hoping to use their experience as they pursue careers in the medical field.
On Tuesdays and Thursdays, organizers serve hot meals and wait inthe small clinic room for patients to trickle in, usually about 20 a week.
Once a month, the team takes to the streets with wound care supplies, such as bandages, saline sprays, and antiseptic cleansers. They look for people on the streets who may not be able to reach the clinic.
Clark said the clinic stepped up its hours in an effort to help patients keep their wounds clean more consistently — and hopefully prevent more amputations. “It’s increasing [patients’] ability to know what to do and how to keep the wounds clean — hopefully to help them out,” he said.
The trust factor
This year, medetomidine, another animal tranquilizer that causes severe withdrawal, has supplanted xylazine’s dominance in the Philadelphia area drug supply. Fewer patients addicted to opioids are visiting emergency rooms with soft-tissue damage, according to city data.
But it’s unknown how medetomidine affects those wounds, and there are still enough people suffering from them in Kensington, the epicenter of the city’s opioid crisis, that the clinic felt it necessary to increase its hours.
Hosting more frequent clinics also deepens relationships with patients. “People are coming back, which is good,” Clark said. “The trust factor is a huge issue.”
Many of the clinic’s patients avoid hospitals, fearing long waits for care: “At the ERs, they wait eight hours and they sign themselves out, or they’re coming down from a high, and nobody’s taking care of the withdrawal,” Clark said. “It’s a big mess.”
At the clinic,staff are regularly on the phone with wound care physicians at Temple University Hospital, who can flag patients with xylazine wounds and get them prompt care before they enter withdrawal, he said.
They also connect patients with housing, inpatient rehabs, and hospital care, for those with wounds too serious for the clinic to handle.
Several weeks ago, they called an ambulance to get a man with a wound that exposed his bone to the hospital.
Staff collect data to share with area hospitals so physicians can get a better understanding of the situation on the street — measuring patients’ wounds, collecting demographic data, and asking patients about which drugs they use.
Each leaves the clinic with a hospital bracelet documenting the care they’ve received so staff can keep track of their care from week to week.
‘It’s always an uphill battle’
Not all patients at the clinic are suffering from xylazine wounds. On a recent weekday, one man asked for help bandaging scrapes on his knuckles. He’d tried to fight someone who was stealing his belongings.
Another man said he’d been robbed and pepper-sprayed and asked staff to help wash the last traces of Mace out of his eyes.
As staffers looked for eyedrops among their medical supplies, Clark poked his head into the room. “We need someone with Narcan,” he said, referring to the opioid overdose-reversing spray.
Across the street, a man was slumped on a stoop, unresponsive.
Clark and Hudak dodged cars on Allegheny Avenue, knelt down by the man, and managed to gently shake him awake.
Slowly, he revived enough to speak a bit and showed them a wound on his leg, which they cleaned and wrapped in gauze. “You have some cracked skin — do you want us to put some moisturizer on your hands?” Hudak asked.
With temperatures dropping, the team is worried that patients’ skin will dry out, making their wounds more painful. (The summer months present a different challenge, with wounds leaking fluids.) And many patients may be too cold to travel to the clinic, making the monthly street rounds even more crucial.
On Nov. 19, a webpage at the Centers for Disease Control and Prevention was updated with a stunning reversal of the agency’s long-held — and scientifically backed — position on vaccines and autism.
Previously, the CDC has noted on its website that decades of research show no link between receiving vaccines and developing autism.
Now, the site reads: “The claim ‘vaccines do not cause autism’ is not an evidence-based claim because studies have not ruled out the possibility that infant vaccines cause autism.”
A header on the webpage still reads “Vaccines do not cause autism.”
But the phrase is followed by an asterisk leading to another statement explaining the header remains “due to an agreement with the chair of the U.S. Senate Health, Education, Labor, and Pensions Committee that it would remain on the CDC website.”
The chair is Sen. Bill Cassidy (R., La.), who made his confirmation vote for Health and Human Services Secretary Robert F. Kennedy Jr. contingent on that agreement.
The move was met with outrage from public health experts who say that Kennedy, a longtime anti-vaccine advocate, is risking lives by calling vaccines’ safety into question. The New York Times reported two days later that he had personally ordered the website changed.
Diana Robins, the director of the A.J. Drexel Autism Institute at Drexel University, which studies autism from a public health perspective, spoke with The Inquirer about the update and what it means for public health.
This interview has been lightly edited for clarity and brevity.
Question: Take us through the update on the CDC’s website about vaccines and autism.
Answer: The frightening thing, to me, is if a person who is not really familiar with the science reads this website, there is a lot of convincing-sounding language. It feels like deliberate gaslighting.
It’s using terms they’ve learned from scientists over the last several months — “gold-standard science” and “evidence-based claims” — and using them in directly inaccurate ways.
The very first key point at the top of the page says, “The claim ‘vaccines do not cause autism’ is not an evidence-based claim because studies have not ruled out the possibility that infant vaccines cause autism.”
Part of what makes that so egregious is that scientists believe in the scientific process. Unfortunately, the federal administration is weaponizing the fact that scientists won’t come out and say it has been proven. A scientist will never say we have 100% ruled out all possibilities. Something we think we know could change tomorrow when we learn something new.
But there are dozens of studies over many, many years that fail to show a link between vaccines and autism. All the studies that are rigorous and methodologically sound fail to show a link between vaccines and autism. That is unequivocal.
Q: What’s the danger in changing the CDC’s language around vaccines?
A: Vaccines save lives. Vaccines are one of the frontline public health strategies to support health in the population. We’re already seeing what happens when vaccine compliance goes down, when there’s an erosion of the public confidence in vaccines.
There have been measles outbreaks in the last year in the United States. Some kids just get sick and they get better, but some kids have serious illnesses and occasionally die. And it’s not just measles. We’re vaccinated against a lot of life-threatening diseases.
The cost is a huge shift in public health, and the protective factor that vaccines give us against life-threatening illness.
If you told me that reading books past 10 p.m. might cause autism, I would say there’s probably not a lot of cost if you stop reading books at 9:59. But not vaccinating children? The costs are huge. Even one death that’s preventable is a tragedy.
And there will be a lot of preventable serious illness and death if parents don’t vaccinate their children.
Q: How does this affect the public’s view of federal health agencies?
A: I think it makes it very difficult for people to know what to trust. And there is already decreased trust in the medical community, scientific community, higher education broadly.
If pages like this are intermingled with legitimate pages, how will people know which ones are the accurate pages and which are the ones with gaslighting and anti-science? I think people will likely lose their faith in the CDC altogether, which is a terrible blow to the public health of the whole country. If we can’t trust our Centers for Disease Control, who can we trust?
Q: How can scientists communicate accurate medical information with the public?
A: One thing I think is slightly heartening in the face of this devastation is that professional societies and organizations that are medical or scientific are all aligned. There have been so many statements that came out within the first day of this, and they are fully aligned in agreement. The only differences are in which words they yell the loudest.
You can usually not get scientists to agree to anything in a day. That means a lot. It’s the responsibility of all the legitimate scientists and public health experts to try to combat that misinformation every which way we can.
[At the A.J. Drexel Autism Institute], we’re trying to do more outreach to the public. We actually developed some vaccine info sheets just a couple months ago that are posted on our website. We have a new website … that brings together all of the information.
Vaccines are one of our biggest public health successes. If we roll those back, we have stepped back decades in the health of our country. It’s that big. It’s that serious.