The University of Pennsylvania is getting $7.8 million over the next two years to study an overlooked aspect of human health: the lymphatic system.
Often described as the body’s sewer system, its main job is to maintain the body’s balance of fluid and filter out waste. Millions of Americans live with dysfunction in the system, often unknowingly.
The time to diagnose some lymphatic disorders is at least five years, said Maxim Itkin, an interventional radiologist who directs Penn’s center specializing in lymphatic disorders.
He’s even had a patient who experienced unexplained symptoms for 50 years before getting treatment.
“Right now, most healthcare providers simply aren’t equipped — or trained — to recognize lymphatic dysfunction, and the tools they need are virtually nonexistent,” said Kimberley Steele, a program manager at the Advanced Research Projects Agency for Health (ARPA-H), the federal agency organizing the research effort.
That’s why the government, through ARPA-H, is investing $135.7 million toward research headed by 11 institutions in the U.S. and Canada, including Penn, to improve detection of issues in the lymphatic system.
With its slice of funding, the team at Penn will develop ways to image the network and identify hidden signs of disease.
An inside look
Similar to plumbing, fluids in the lymphatic system can be flowing, obstructed, or leaking.
Doctors are able to “close” these leaks and even “open” obstructed areas, but the problem is knowing when those procedures are needed.
Existing contrast agents — substances used to increase visibility of tissues during imaging — for the lymphatic system are largely considered obsolete and offer poor resolution, said Itkin, who is leading the Penn project, which started last October.
When he began researching the system 20 years ago, he “started to realize that it’s of enormous importance, and it’s forgotten primarily because nobody can image [it] and do interventions,” he said.
Maxim Itkin, an interventional radiologist at the Hospital of the University of Pennsylvania, found a way to track the flow of lymphatic fluid using X-ray imaging equipment.
Itkin and his team have come up with ways of imaging by injecting dye into lymph nodes and tissues and tracing the dye’s location. This has enabled him to diagnose hidden conditions and develop new treatment methods.
The ARPA-H funding will allow them to go even further, developing imaging agents that focus on the parts of the lymphatic system in the liver and gut — organs that generate the majority of the network’s flow in the body.
These will be used for CT (computed tomography) and MRI (magnetic resonance imaging) scans.
One of the imagingcandidates is designed to be swallowed and absorbed in the intestine, so doctors can see the lymphatic system in the gut. The second imaging agent will be administered via IV to show the system in the liver.
“It was my dream to see the lymphatic system from inside by itself,” Itkin said.
They’ll be using an approach called AI-driven multi-omics, where AI will analyze samples for unique molecules being excreted by the lymphatic system in the liver.
Penn and several other funded groups are working with the New York-based nonprofit Lymphatic Education and Research Network to help with research and patient recruitment.
Current funding is for two years, with the potential to extend for another three years.
Itkin says seeing the lymphatic system in the liver will be a thrill.
Before 1751, sick Pennsylvanians had few healthcare options other than often expensive home visits from doctors. That changed when Benjamin Franklin and physician Thomas Bond established a medical institution to treat the physically and mentally ill for free.
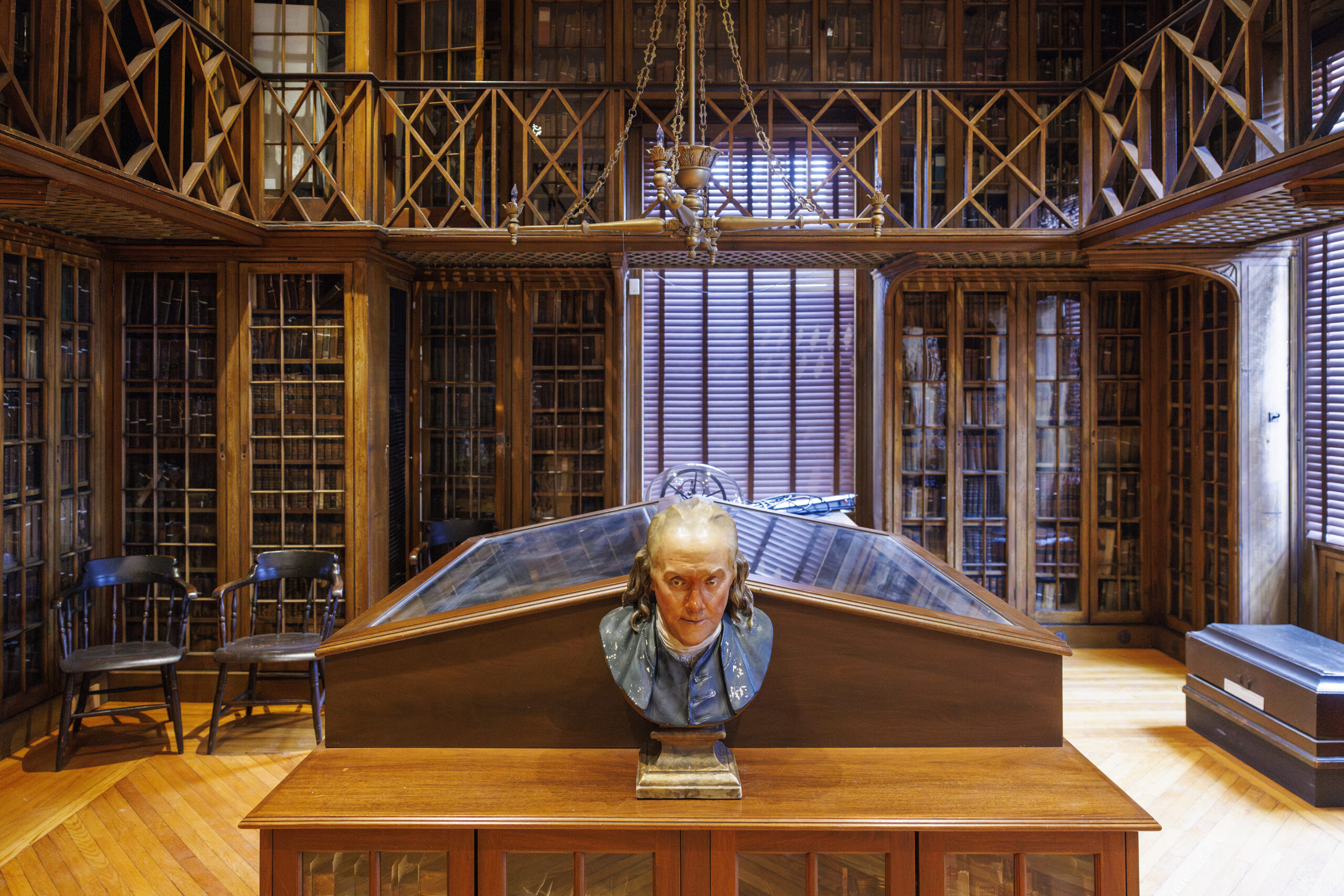
The result was the Pennsylvania Hospital on Spruce Street. The 275-year-old institution became home to the country’s first surgical amphitheater to teach students, the oldest medical library, and a nursing museum, among other historic firsts. It continues to advancemedical research as part of Penn Medicine.
Now the nation’s oldest charteredhospital will become Philadelphia’s newest museum.
The hospital’s Pine Building, which started construction in 1755, will be converted to the Pennsylvania Hospital Museum, Penn announced on Monday. The museum in the majestic Georgian architecture building at Eighth and Pine Streets, designed by architect Samuel Rhoads, is scheduled to open to the public on May8.
“It’s a very Philadelphia story to hear the history of the hospital because it really is about caring for other people,” said Stacey Peeples, lead archivist at Pennsylvania Hospital.
Stacey Peeples, lead archivist at Pennsylvania Hospital, described artifacts in the hospital’s new museum.
The medical library, surgical amphitheater, and apothecary have all been restored for the museum. Eight galleries will feature videos, hands-on activities, and archival objects describing the history of the hospital and the care it delivered.
The opening of the museum in the hospital’s 275th year coincides with America’s Semiquincentennial celebrations. (The University of Pennsylvania Health System, which merged with the hospital in October 1997, will run the museum.)
One of Peeples’ favorite items on display is a collection of medical cases compiled by the hospital’s doctors in the early 19th century.
Housed in the historic library, the book is flipped to a page showing a man with a seven-pound tumor in his cheek and neck area. Visitors can also find the actual preserved tumor from 1805 on display in the back of the room.
A historic medical book compiling interesting cases at Pennsylvania Hospital shows an image of Pete Colberry, a patient who fell from ship rigging and was stabilized on a bed to hold him in place, circa 1804.
A look at early medicine
Pennsylvania Hospital’s apothecary — where medicines were mixed and sold — was last used for that purpose in the early 1900s.
Most recently, it served as a conference room.
It’ll now be restored to its original layout, based on historic images from the 19th century. That includes bringing back alcoves filled with shelves of bottles, the scale used to weigh ingredients, as well as a giant counter where the apothecary could mix medications, Peeples said.
An archival image of Mildred Carlisle working in the Pennsylvania Hospital apothecary, circa 1920s.
In the historic library, the only room ready for news media to view this week, the artifacts remained scattered around.
A tonsil guillotine, designed to remove tonsils using a blade, sat next to early surgical tools and stethoscopes. Some objects, such as the scalpel, have not changed significantly in form through the years.
“But how we treat those objects certainly is very, very different. We want to make sure everything’s sanitized now,” Peeplessaid.
Surgical instruments belonging to Dr. James Wilson from the 1800s.
Other artifacts included old tools of medical education.Like three anatomical casts of women who died during childbirth in the mid-1700s that were used for anatomical study in lieu of cadavers.
The museum’s exhibits will showcase the hospital’s history of delivering care related to behavioral health and women’s health, as well as its role treating patients during times of conflicts, beginning with the Seven Years’ War, and through pandemics.
“People would always talk about us being able to do something on a larger scale like this, and I honestly wasn’t sure that was ever going to happen,” said Peeples, who has been at the hospital for 25 years.
Tickets will go on sale at the end of the month and cost $12 per person, with discounts for those 12 and under, 65 and over, and the military.
The plan is for the museum to be a permanent fixture, open Wednesdays to Sundays. The rest of the hospital will keep operating as normal.
Interior of the Historic Library of Pennsylvania Hospital, located at Eighth and Pine Streets.
The hospital, older than the nation, houses 517 licensed inpatient beds, and saw 19,759 adult admissions, 54,023 emergency department visits, and 5,163 births in fiscal year 2025, per Penn Medicine’s statement.
“Pennsylvania Hospital is a jewel in the crown that is Penn Medicine, where our staff draw energy from our rich history to shape the future of medicine,” Alicia Gresham, CEO of Pennsylvania Hospital, said in a statement.
Jefferson Health oncologist Jennifer Johnson had exhausted all the standard treatment options for her 49-year-old patient with esophageal cancer, who was likely to die within months.
Surgery, chemotherapy, radiation, and immunotherapy had kept the Northeast Philadelphia woman alive for six years after her diagnosis, but no longer were enough to stop her cancer from spreading.
Johnson knew her patient needed something novel. She recalled a presentation several years prior at a conference for head and neck cancers, where a doctor discussedan experimental treatment called T-cell receptor (TCR) therapy.
This type of cancer immunotherapy works by engineering the immune system to fight cancer, and falls into the same family of treatments as CAR-T, or chimeric antigen receptor (CAR) T cell therapy, an approach pioneered at the University of Pennsylvania that has revolutionized treatment for blood cancers.
She thought TCR therapy’s clever approach could work against solid tumors, where CAR-T had not been effective.
“I just remember sitting in the room and watching him present, thinking, I’m gonna use that one day,” the oncologist and cancer researcher recalled.
As it would happen, the approach was being tested in a phase II clinical trial at Rutgers Cancer Institute against tumors just like her patient’s: metastatic cancers driven by a virus called human papillomavirus 16. One of the most common strains, HPV16 causes roughly half of cervical cancer cases worldwide, as well as cancers of the head and neck area, anus, and genitals.
Cases that reach the metastatic stage like Johnson’s patient often run out of treatment options. Whether T-cell receptor therapy would work was unknown, but the alternatives were expected to fail.
“Anything that you might offer them would definitely not be expected to make their cancer go away completely and do it for a long time,” said Christian Hinrichs, the oncologist and scientist heading the trial whose presentation Johnson saw.
But interim results from the first half of the trial showed improvement in six out of 10 patients, whose tumors at least partially shrank. And two of them had no evidence of cancer after treatment.
Johnson’s patient, Maria Pascale, was one of thetwo whose promising early results were presented at a medical conference and highlighted in a research abstract in the Journal for ImmunoTherapy of Cancer in November.
She arrived at the health system in New Jersey in the summer of 2024 in such poor health thather lungs were starting to collapse.
The therapy has enabled her to celebrate two birthdays, start martial arts classes, reunite with old friends visiting from Argentina, and see her 23-year-old son get engaged.
“Imagine the wedding, then later the grandkids, I’m always thinking about [that],” she said.
What is a T-cell receptor therapy?
In the immune system, T cells act as frontline defenders against viruses, bacteria, and other threats.
Sometimes, these cells aren’t great at their jobs.
In the face of cancer, T cells can become exhausted over time, and fail to recognize invaders or mount attacks.
The idea behind immunotherapy is to transform these regular immune cells into cancer-fighting super-soldiers.
The Rutgers approach, an engineered TCR therapy, involves collecting T cells from a patient’s blood and genetically engineering them to better target a cancer cell for attack.
Afterward, the scientists grow more of the enhanced T cells in the lab and infuse them back into the patient.
The “prototype” for this style of therapy is CAR-T, a treatment that has saved tens of thousands of lives since the first FDA approval in 2017. Scientists have not yet been able to replicate the therapy’s success in blood cancers in solid cancers, although some early stage trials have shown potential.
TCR therapy is thought to be more promising against the latter cancer type — which is what’s being treated in the Rutgers trial — due to differences in the way the engineered T cells identify cancer cells.
CAR-T therapy uses what’s called a chimeric antigen receptor, a protein that recognizes a cell as cancer based on what’s on the outside of the cell.
It’s like knowing you’re at your friend’s house because of a specific doormat or set of house numbers on the exterior.
TCR therapy uses what’s called a T-cell receptor, which can recognize cancer cells based on what’s inside the cell.
It’s like knowing you’re at your friend’s house because you can see your friend inside.
Sometimes cancer cells have more unique identifiable elements on the outside, but other times they don’t. Imagine if multiple houses had the same doormat.
“That target would be on other cells that aren’t cancer cells and cause lots of toxicity,” said Carl June, the pioneering cancer scientist at Penn who developed the first FDA-approved CAR-T therapy and was not involved in the Rutgers trial.
That’s been the problem that’s held back CAR-T’s use in solid tumors.
The target in the Rutgers trial is a protein called HPV16 E7, found inside the cell. In tumors driven by the virus HPV16, it plays a key role in turning a cell into cancer.
“That’s like going after its Achilles’ heel,” June said.
Swarming the cancer
Pascale first arrived at Thomas Jefferson University Hospital in Center City in 2018 after suffering injuries in a car accident.
Doctors found a mass in the 43-year-old’s neck that turned out to be cancer.
Surgeons removed the mass,and she was fine until 2021 when doctors, including Johnson, found the cancer at the top of her esophagus.
They treated her with a combination of chemotherapy and radiation, which worked until March of 2022, when the cancer started appearing in Pascale’s lungs.
“All bets were off,” Johnson said.
Doctors gave Pascale chemotherapy and immunotherapy over the next couple of years, but in the spring of 2024, she developed an allergy to one of her chemotherapy drugs.
Around the same time, the cancer spread to the skin on Pascale’s back.
That’s when Johnson transferred her care to Hinrichs’ team at Rutgers.
Pascale started preparations for the treatment in July 2024, spending a couple weeks in the hospital.
The Rutgers team took T cells from her blood, gave her chemotherapy to knock her immune system down, and then transfused the engineered cells back into her body.
Within 48 hours, Pascale started feeling horrible.
“It was painful. It was my whole body, like I had pneumonia,” she said.
She had trouble breathing as the cells fought the cancer in her lungs. Hinrichs described it as “the T cells swarming the cancer,” leading to an inflammatory reaction.
The same thing occurred on her back. When Pascale’s sister came over, she saw one of the tumors in her skin was suddenly the size of a lemon.
Another one appeared red and felt like someone was burning a cigarette on her back.
The pain continued for three days, and then she felt well enough to go home. Pascale and her sister could see and feel the nodules on her back get smaller, until eventually they were gone.
Roughly five months later, Pascale’s scans showed no evidence of cancer. As of last month, a year and a half after she received the treatment, that was still true.
“What’s three days of pain compared with the opportunity that I have to live a lot of beautiful things with my family and friends?” Pascale said.
Maria Pascale walks with her sister Maria Durante and her doctor Christian Hinrichs at Rutgers.
The future of the treatment
Hinrichs said his team is working to figure out why two of the patients, including Pascale and a patient with anal cancer, responded better to the treatment.
He cautioned that it’s too early to draw sweeping conclusions since the sample size is small. (Researchers will seek to recruit another 10 patients for the ongoing trial.)
The patients who had complete responses will need follow-up scans every few months to make sure their cancers have not returned.
It will still take years to finish evaluating safety and efficacy. Treatments tested in clinical trials often do not advance to become standard practice.
June, the Penn scientist, called the trial’s early results promising and noted that there weren’t any major safety problems reported.
Adverse effects seen in the trial were mainly those caused by the chemotherapy.
However, the drawback of using TCR therapy is that patients need a certain genetic background for it to work, June said. This is similar to how not every organ donor would be a good match for a recipient.
The genetic profile chosen for the Rutgers therapy is the most common in America. However, it is less common in Black and Asian people compared to white people.
Scientists hope it could one day be possible to manufacture the therapy witha warehouse approach, where TCR therapies that work across genetic backgrounds could be mixed and matched.
“It’s a practical issue that the drug companies face,” June said.
CAR-T, in comparison, canbe used more broadly across different genetic backgrounds.
What matters most, since the treatment is expensive to make, is that the responses hold up over time, June said.
(The TCR therapy’s cost has not yet been set, Hinrichs said, since it is currently manufactured individually for each patient.)
“If they’re long lasting, then it’s really going to be a huge advance because nothing else works in the patients he’s treated,” June said.
At Jefferson, Johnson is cautiously optimistic about the treatment that has kept her patient alive.
If the therapy makes it through the rest of the trial process and proves effective, she hopes it could become “another thing in our armamentarium against this type of cancer.” (A type that doctors would hope to see less of since the introduction of the HPV vaccine in 2006.)
“I can’t tell you how wonderful it is to have a patient responding and living well when you saw things going the wrong way,” Johnson said.
Editor’s note: This story has been updated to clarify where the research has been presented and a reference to the prevalence of the genetic profile used in TCR therapy.
Marketed as a ticket to deeper sleep, the soft hum of pink noise has become part of millions’ nightly routines.
However, its use may come at the cost of sleep quality, a University of Pennsylvania study suggests.
Published this month in the medical journal Sleep, the study found that the presence of pink noise at night reduced REM sleep — the stagewhen most vivid dreams occur and memory, emotional regulation, and learning are supported. This was based on a sample size of 25 healthy adults assessed over seven days in a sleep lab.
To Mathias Basner, a Penn professor of psychiatry and lead author on the study, it’s evidence that background noise may not be risk-free.
“The negative consequences of the pink noise far outweigh the positive ones that we saw,” he said.
Pink noise vs. white noise
Pink noise is what’s called a “broadband noise,” meaning sounds made up of a wide range of frequencies. The most well-known example of this, white noise, is considered the sound equivalent of the color white, which contains all colors combined.
Pink, brown, and other colored noises differ based on the frequencies they boost.
Pink noise, for example, emphasizes lower frequencies — making it sound similar to steady rainfall or ocean waves. It’s often used for sleep, although uses for focus and tinnitus have also been reported.
These types of background noise can mask unwanted sounds — an appealing quality in an increasingly noisy world.
Since the first white noise machine for sleep was released in the 1960s, hundreds of variations have spawned. Today, 10-hour videos of pink noise, which is often preferred over white noise for sleep due to its softer sound,pick up millions of views on YouTube.
“So many people are using it, and it’s really indiscriminate use,” Basner said.
Putting pink noise to the test
Having studied the effects of noise his whole career, Basner was surprised to learn several years ago that some people used it as a sleep aid.
That led him down a rabbit hole of research, where he found dozens of studies assessing the effects of broadband noise on sleep. However, most of them were considered to be low quality — sample sizes were small and the assessments were usually subjective.
“We don’t know whether it’s working, whether it’s harmful or not,” he said.
He designed his study to occur in the hypercontrolled environment of a sleep lab at the Hospital of the University of Pennsylvania,where participants were measured using polysomnography, a test that looks at brain waves, eye movements, and muscle tone.
This allowed his team to differentiate sleep stages and figure out what was happening biologically as participants were exposed to a variety of conditions: no noise, environmental noise, pink noise, pink noise and environmental noise combined, or environmental noise with ear plugs.
Each night, the 25 participants, comprised of 18 women and seven men,were given an eight-hour window to sleep. (Lights were out at 11 p.m. and back on at 7 a.m.)
His team found that environmental noise — which ranged from the sound of a helicopter to a sonic boom — led to a 23.4-minute decrease in stage 3 sleep. This so-called deep sleep phase where recovery occurs is important for physical repair and immune function, as well as memory.
And while pink noise didn’t affect deep sleep, it was associated with an average decrease of 18.6 minutes in REM sleep.
“REM sleep is extremely important for a lot of things like memory consolidation, emotion regulation, brain plasticity, and neurodevelopment,” Basner said.
Though the study didn’t look at children, he cautioned that babies spend around half of their time sleeping in REM, compared to a quarter in adults.
Based on his findings, he would discourage parents from using broadband noise machines in the bedrooms of newborns.
For adults who don’t want to forgo the noise, he would recommend using the lowest volume and setting a timer so it eventually turns off.
However, the best option would be to use foam ear plugs, he said. When paired with environmental noise in the study, they were able to block out noise and recover 72% of the deep sleep time that had been lost — although they did start losing effectiveness at higher noise levels, around 65 decibels.
“You didn’t get the REM sleep reduction because they didn’t play anything back,” Basner said.
A limitation of the study is that it had a relatively small sample size comprised of younger, healthy people without sleep disorders or hearing loss. It also only looked at the short-term effects of pink noise, and was conducted in a lab setting, versus the participants’ homes.
In the future, Basner hopes to study the long-term effects of pink noise on sleep, as well as test other types of broadband noise.
“We need to do the proper research to make sure that it is actually, at least, not harmful,” he said.
Philadelphia biotechs are worried about losing a key source of federal funding for early-stage innovation.
Known as “America’s seed fund,” the Small Business Innovation Research (SBIR) and Small Business Technology Transfer (STTR) programs helpsmall companies develop innovative technologies. In recent years, they’ve allocated $4 billion annually to more than 4,000 businesses nationwide. However, after Congress failed to reauthorize the decades-old programs last fall, their funding officially expired in September.
The fallout has affected more than a dozen local life sciences companies, raising concerns about whether they can maintain staffing and make up for thedelay in funds promised months ago, said Heath Naquin, senior vice president of innovation and new ventures at University City Science Center, a nonprofit commonly known as the Science Center that provides startup support.
For many, staffing and financing plans could be disrupted by funding shortfalls, as companies either haven’t gotten their payment yet or can’t get their funding for next year approved, he said.
An exact figure is unknown, but Naquin estimated that some affected companies could be short up to a million dollars for the year.
At the same time, the city of Philadelphialaunched last spring a new program that provides additional funding to those who have already earned SBIR/STTR grants. The 21 awardees who will share $450,000 from the city were announced publicly in January.
The citymoney is earmarked for technical assistance, such as the cost of attorneys, marketing, and anything else needed for commercialization, while SBIR/STTR money normally goes toward research and development.
“There is no overnight solution to SBIR right now,” said Tiffany Wilson, chief executive officer of the Science Center, which is partnering with the city to implement the program. “It’s just another layer of uncertainty that we’ve got to navigate through.”
New city-led program
Pennsylvania is not one of the dozens of states that offer matching programs to supplement the federal SBIR/STTR funds.
To fill that gap, Philadelphia launched its new city-level program, which is one of the first in the nation and the only one of its kind in the state.
The idea was to boost companies already vetted by the federal government that could still benefit from smaller amounts of money.
“Life science companies need millions of dollars, but this was a way that we could help Philadelphia-based companies thrive,” said Rebecca Grant, who runs the program and serves as senior director of life sciences and innovation for the city.
This year, the city offered funding to all eligible applicants.
The $450,000 is doled out in three tiers: companies with the earliest stage grants received $20,000 while those in the next phase received $40,000. Those whose grants were no longer active received $2,500.
The program is still a pilot, and city leaders hope to run it on an annual basis, Grant said.
Naquin has heard from at least three companies in the last six months that are formally considering moving to Philadelphia as a result of the program’s existence.
The SBIR/STTR grants are valuable to early-stage biotechs for two reasons: They provide funding without asking for ownership or equity in return, and signal to potential investors that the company is less risky, Wilson explained.
The programs traditionally have been reauthorized every few years without major lapses. However, recent debates over reforms have created a deadlock.
Policymakers from both parties want to address companies that are repeatedly going back for more funding, concerns over foreign involvement, and how to better support commercialization, Naquin said.
“We’re still in a waiting game,” he said, adding that the programs were not reauthorized in the latest government funding bill passed this week.
With the SBIR/STTR pipeline stalled, the Science Center has had to pivot. Federal support for science has been particularly precarious under President Donald Trump’s second administration, with widespread cuts and pauses to millions of dollars worth of programs and grants.
Late last year, the center launched aninitiative to help startups figure out which agencies still have available funding opportunities.
The aim is to help them better shop around for the grants that they can apply to, Wilson said.
Competition at Philadelphia-area medical schools intensified in 2025, with programs seeing about 50 applicants for every open spot.
That’s the highest demand since 2022, with the number of applications bouncing back after a three-year decline, recently released data from the Association of American Medical Colleges(AAMC) shows.
The annual report offers a look at the composition of the nation’s future doctors through the demographics of the applicants and enrollees at M.D. degree-granting medical schools across the United States and Canada.
It showed increased class sizes and strong female enrollment across the Philadelphia area’s five M.D. degree-granting schools: University of Pennsylvania, Thomas Jefferson University, Temple University, Drexel University, and Cooper Medical School of Rowan University.
And the fraction of first-year medical students from Pennsylvania who identified as Black or African American, excluding the mixed-race student population, fell from 6.9% to 5.4% between 2023 and 2025.
The racial demographics of entering studentsare seeing increased scrutiny in light of the 2023 Supreme Court decision that effectively ended affirmative action, barring race from being used in higher education admissions.
The percentage of first-year medical students from Pennsylvania who are Black is lower this year than the national average. Pennsylvania also lags behind the national average for first-year enrollment of Hispanic or Latino medical students.
This data reflects the results of the application cycle that concluded last spring. Next year’s prospective medical school students are currently in the thick of admissions season, awaiting interviews and offers.
Here’s a look at the key trends we’re seeing:
Applications back up
Demand for spots at Philadelphia area-medical schools is back up after a three-year decline. There were nearly 5,000 more applications last cycle, a 9.3% increase, with all schools except Cooper seeing a boost.
Jefferson’s Sidney Kimmel Medical College helped drive growth the most, with a 16% increase in applications compared to the previous year.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
More medical students being trained
Orientation icebreakers might take a bit longer to get through at area-medical schools as first-year classes continue to get bigger.
In 2025, Philadelphia-area schools enrolled 1,089new medical students, compared to 991 in 2017. Drexel University College of Medicine contributed to half of that growth, adding 49 seats to its recent entering class compared to that of 2017.
Penn’s Perelman School of Medicine was the only school that did not increase its class size in 2025.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Female enrollment remains strong
More female students have entered Philly-area medical schools over the last decade.
In 2025, 55.4% of first-year enrollees at Philly-area medical schools were female, compared to 47.7% in 2017.
Drexel saw the biggest rise, with 181 women entering in 2025, compared to 120 in 2017.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Inside a heated tent on the Children’s Hospital of Philadelphia campus, 17-month-old KJ Muldoon wiggled around in his mother’s arms, smiling and clinging to a multicolored toy.
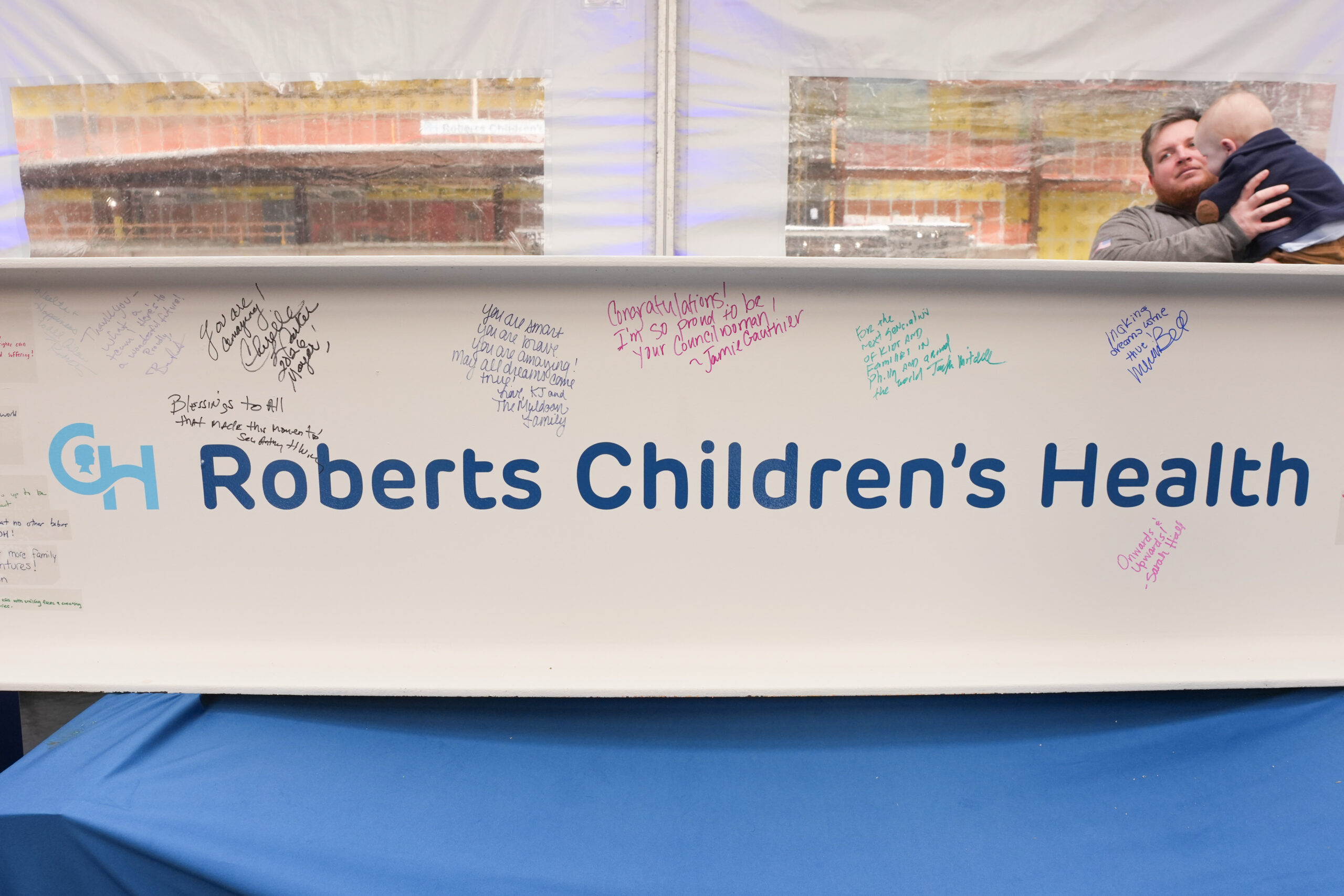
He was there to celebrate a 26-story patient tower at CHOP that his father, Kyle Muldoon, a longtime construction worker, is helping build. Called Roberts Children’s Health, the new inpatient complex is set to launch in 2028 and significantly expand the number of beds available for patients at CHOP’s main campus.
KyleMuldoon had joined the project back in December 2024, when KJ was still hospitalized at CHOP, where his life-threatening genetic condition was successfully treated with a first-of-its-kind personalized gene-editing therapy.
But in the months before the treatment developed by doctors at CHOP and the Hospital of the University of Pennsylvania sparked international attention, KJ’s father was recently unemployed. The Clifton Heights father of four had accepted a layoff to focus on his sick son.
Muldoon joined the crewin December 2024, allowing him to stay close by during KJ’s 307-day stay and contribute to a project that feels meaningful to him.
“Every day when I get up, I know what I’m doing this for,” Muldoon said.
KJ Muldoon, left, and his father Kyle Muldoon, right, at a news conference at CHOP.
His son KJ was born in August 2024 with a metabolic disorder that puts babies at risk of severe brain damageand is fatal in half of cases. Called severe carbamoyl phosphate synthetase 1 (CPS1) deficiency, it prevented KJ’s liver from being able to process protein.
Doctors Kiran Musunuru and Rebecca Ahrens-Nicklas useda gene-editing technology known as CRISPR to create a personalized drug that would fix the genetic mutation that was driving KJ’s disease. After receiving three doses, he was able to go home last June.
“This pipe dream that sounded like it came from a sci-fi movie became a reality,” Muldoon said.
The medication is not a cure, but it has dramatically improved KJ’s liver function and made the effects of his disease milder.
The treatment approach has been hailed for its potential for rare-disease drug development. The U.S. Food and Drug Administration in the fall announced a new approach to clinical trials to test novel drugs like the one designed for KJ, who was called “a trailblazing baby” by the British scientific journal Nature when it named him to its year-end list of the top 10 influential people.
With dietary restrictions and daily medication to keep his ammonia levels down, the toddler has been able to meet milestones, like walking and saying some words (currentlya lot of “mama” and “dada”).
These days, KJ likes playing catch, eating, and chasing his siblings around.
“Sometimes you got to sit back and take it all in, because we never knew if that was going to be a possibility,” Muldoon said.
The new tower’s construction is funded in part by a $125 million donation from Comcast CEO Brian Roberts and his wife, Aileen, whose name will be on the new building.
Wednesday’sevent included signing and raising the final structural beam of the building’s frame.
The event included signing and raising the final structural beam of the building. It was signed by patients at CHOP in Philadelphia.
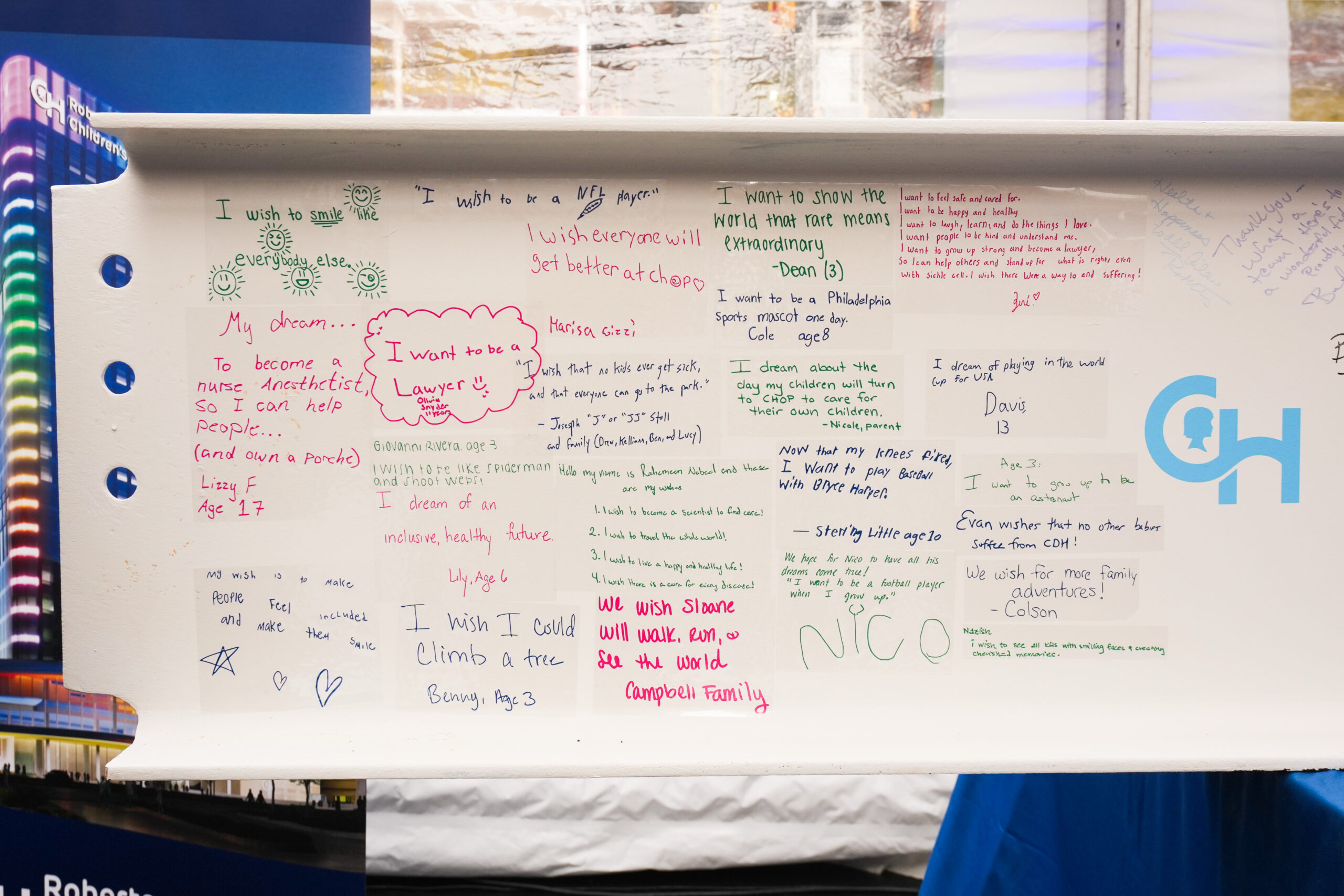
On the beam were colorful messages from patients at CHOP who were asked to write down their dreams.
Brian Roberts read some of their notes at the event.One girl said she wanted to become a nurse anesthetist so she “can help people and own a Porsche.” Another said, “My wish is that every kid that goes to Roberts Children’s Health comes out better and stronger.”
Roberts read aloud messages from patients at CHOP that were signed onto the beam.
Editor’s note: This story was updated to clarify the message a child wrote on a building beam and shared at the event.
The Wistar Institute’s long-standing president and CEO Dario Altieri will step down at the end of the year after leading the independent biomedical research institute for 11years, officials announced Monday.
Wistar plans to launch a national search for his successor, but did not share further details.
Altieri joined Wistar in 2010 as its cancer center director and first chief scientific officer. Five years later, he was promoted to the role of president and CEO.
During his tenure, the West Philadelphia-based institute’s annual budget quadrupled to more than $100 million, and its endowment tripled to $277 million, according to a news release.
The number of independent labs also grew from 30 to 41, and two new research centers were created.
Its cancer center, which Altieri directs, received its third consecutive renewal as a National Cancer Institute (NCI)-designated Basic Cancer Center with an “exceptional” rating.
“Due in large part to Dario’s efforts, Wistar is exceptionally well positioned for continued growth and success,” said Rick Horowitz, the board’s chair, in a statement.
The 67-year-old started his career in Milan, Italy, where he underwent his medical training. He has served in faculty roles at the Scripps Clinic and Research Foundation, Yale University, and the University of Massachusetts Medical School.
As a cancer biologist who still leads aresearch laboratory, he has authored more than 260 research papers and been listed as an inventor on 13 patents.
“[I] look forward to dedicating my time to the values of work that have defined me since I was a medical student: laboratory research, teaching and mentoring,” Altieri said in a Monday statement released by the institute.
The University of Pennsylvania has received an $8 million gift to redesign how it trains doctors at the Perelman School of Medicine, Penn officials announced Thursday.
Incorporating technology, AI, and data to create customized learning pathways for Penn medical students is an overarching goal. The effort comes at a time when increasingly easyaccess to medical information and changes in care delivery are leading medical schools nationwide to revamp their curricula.
The gift to Penn is from New York-based RTW Foundation, a philanthropy associated with the life sciences investment firmfounded by Perelman School graduate and Penn Medicine board member Rod Wong. Penn said the gift from Wong, and his wife, Marti Speranza Wong, is the largest single donation to support curriculum innovation at the medical school, which dates back to 1765.
At a news conference announcing his donation Thursday, Wong recalled his time atthe medical school right after its last major overhaul of the curriculum in 1998. One update underPenn’s “Curriculum 2000” revamp was recording and making lectures available online — a relatively innovative move at the time (YouTube wouldn’t be created for another several years).
“Technology has changed, and obviously we’re at this same inflection point because of AI and data science,” said Wong, who is managing partner and chief investment officer at RTW Investments LP.
Penn alumnus Rod Wong (center) sits with dean of Perelman School of Medicine Jonathan A. Epstein (left) after signing the gift agreement.
The vast majority of the $8 million gift will go toward hiring data scientists and engineers, supporting faculty, and building and acquiring the platforms needed to deliver the new curriculum.
Technology will be incorporated into new training techniques, such as byusing augmented or virtual reality to assist in learning anatomy, developing knowledge needed to diagnose illnesses and develop treatment plans, and mastering clinical skills such as IV placement and suturing.
For example, students can practice taking a person’s medical history or doing a physical exam on a virtual patient, while an AI agent is there to give feedback in real time.
“It’s really adaptive to the individual learner, but you do it at your own pace, on your own time,” said Lisa Bellini, executive vice dean of the medical school and a leader on the project.
The redesign will take place over the next three years as school leaders consult with stakeholders and work on building the platform.
Some of Wong’s gift will be used to create a biannual endowed lecture in business and entrepreneurship that will bring leaders in medicine and healthcare innovation to campus. The gift will also establish the Roderick Wong Entrepreneurship Pathway, which will provide mentorship, workshops, and project-based learning to students with business interests.
“We really need to incorporate the fundamentals of how best to use technology responsibly within the practice of medicine and create something incredibly enduring, because you’re not going to go through this exercise every three years,” Bellini said.
The Perelman School of Medicine is embarking on its curriculum revamp at a time when medical education is evolving at many schools.
Some medical schools have concentrated the traditional two years spent learning science into one year to give students more time to learn how to interact with patients and collaborate with other medical professionals.
A three-year medical school option is offered at institutions such as the Pennsylvania State University College of Medicine to speed doctors into the clinic and reduce students’ debt loads.
Jennifer Kogan, vice dean for undergraduate medical education at the Perelman School of Medicine, is a leader in the curriculum revamp.
Faster, flexible learning
Like most medical schools, Perelman has a standard curriculum where students take foundational science courses for a stretch of time and then transition to the hospital to gain clinical experience.
This can lead to some students repeating courses that they already mastered in college.
“If you were a biochemistry major as an undergrad, do you really have to take biochemistry again?” said Jennifer Kogan, vice dean of undergraduate medical education and a leader on the redesign project. “How could you better use that time to achieve whatever your career goals are?”
Leaders at Penn want to give students the flexibility to adjust their timelines based on their skill sets and goals.
Instead of setting a fixed time for how long a class or rotation will take, a student who masters a skill more quickly should be able to move on and devote their time to other interests, such as research or entrepreneurship.
Many students at Penn pursue dual degrees or research fellowships that end up adding a fifth year of medical school. Penn leaders hope adding flexibility to the curriculum could enable students to instead finish in four years or “maybe even three,” Kogan said. (The possibility of a three-year path is not yet guaranteed but will be explored.)
“It will be better set up to support students like me who have had to use significant federal loans to finance their way through medical school and might have benefited from the condensed training timeline,” said Alex Nisbet, a fourth-year medical student at Perelman who spoke at the signing event.
An attendee holds a pennant flag representing the Perelman School of Medicine.
The school will leverage data and AI to assess how individual students are progressing in what they’re calling a “precision education model.”
Though parts of the program will be piloted over the next three years, the first class to see the full implementation of the curriculum will be in the fall of 2029.
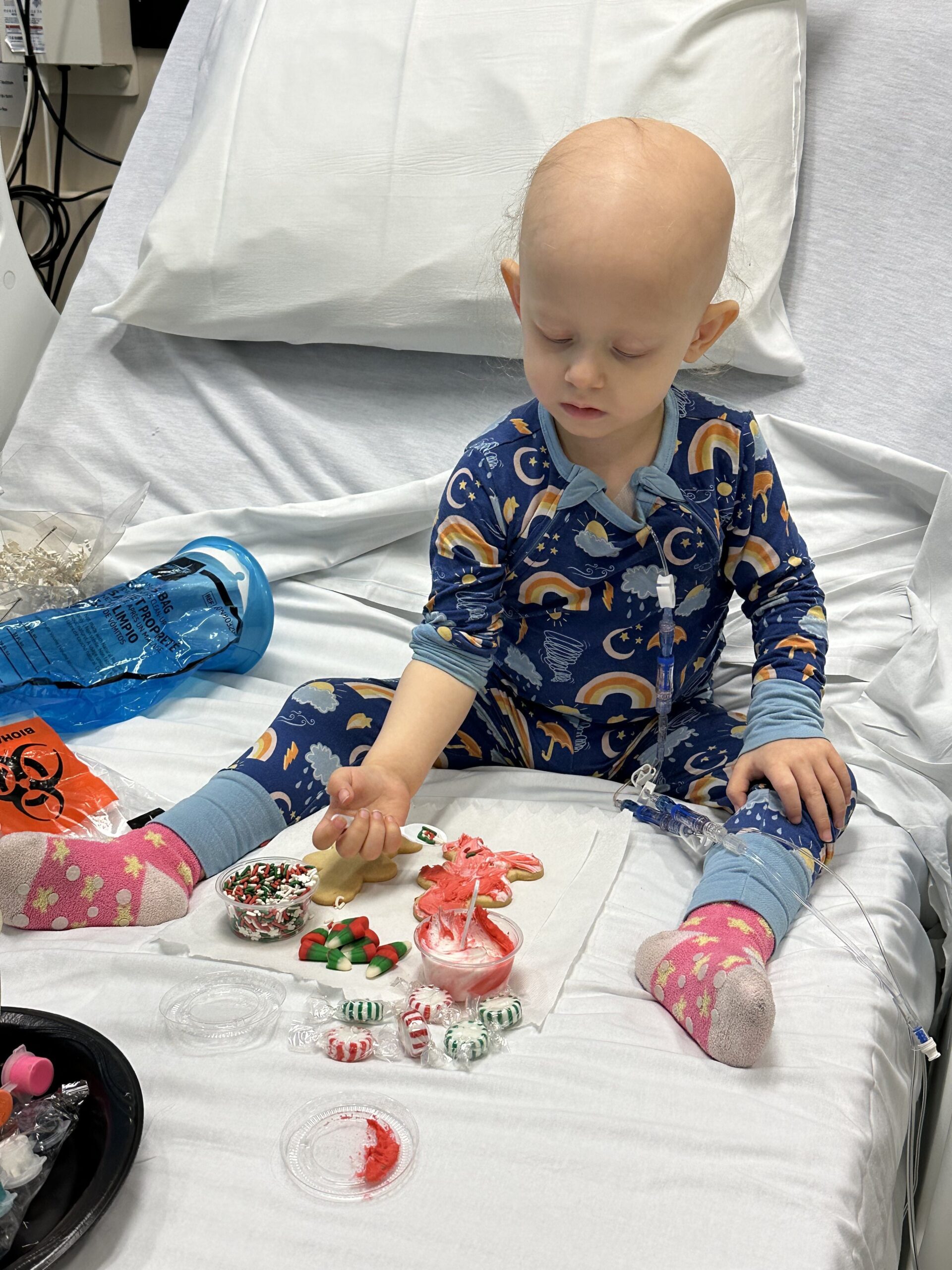
Adalyn Hetzel had just celebrated her second birthday in the spring of 2024 when doctors at Children’s Hospital of Philadelphia diagnosed her with an aggressive soft tissue cancer.
She endured 40 weeks of aggressive chemotherapy and a month of daily proton radiation therapy on her road to remission.
Now, the Bucks County toddler will spend the next year sharing her story as one of five ambassadors for the St. Baldrick’s Foundation, one of the nation’s largest childhood cancer charities.
The California-based organization has awarded more than $369 million in research grants since 2005, with $18 million going to Philadelphia-based institutions.
The selected children and their families will attend advocacy days in D.C., to appeal to lawmakers, share their stories with the public, and spread awareness on social media.
Kristopher Hetzel, Adalyn’s father, said their goal will be to advocate for research into more effective, less toxic treatments.
While more than 80% of kids diagnosed with cancer in the United States now survive the disease, many sustain long-term side effects due to the harsh therapies. One study found that by age 45, 95% of survivors had at least one chronic health condition, and 80% had one that was disabling or life-threatening.
Adalyn will likely have severe dental issues, limited jawbone growth, and an increased risk of developing secondary cancers due to the treatment later in life.
The threat of recurrence also still looms.
“It can’t be like that for these kids. We got to come up with better treatment,” Hetzel said.
Hetzel first noticed a small nodule on Adalyn’s tongue in April 2024.
After appointments with her pediatrician, dentist, and two oral surgeons left the family without a diagnosis, they went to CHOP, where a biopsy confirmed she had a highly aggressive form of soft tissue cancer called rhabdomyosarcoma.
“All of a sudden your world becomes so small and it’s just your kid. Nothing else matters,” Hetzel said.
Adalyn and her parents, Kristopher Hetzel and Allison Verdi.
Doctors started Adalyn immediately on an intense chemotherapy regimen combining three drugs. She also received a month’s worth of daily proton beam radiation, requiring general anesthesia each session due to her age.
By the end of the 40 weeks of chemotherapy, Adalyn dropped down to the 0.4th percentile of weight. She was so immunocompromised due to the treatment that when she contracted the flu, a critical response team at CHOP had to rush in.
Doctors withheld her final chemotherapy session for fear it could be life-threatening.
Adalyn Hetzel, a 3-year-old from Southampton, Pa., received 40 weeks of chemotherapy to treat her rhabdomyosarcoma.
Being an ambassador
In April, nearly a year after her diagnosis, Adalyn was declared to be in remission. She still receives scans every three months due to the potential for recurrence.
“[Adalyn] turned back into this playful, happy, joyful toddler who finally has the energy to be herself,” Hetzel said.
Her family decided to get involved with St. Baldrick’s after benefiting from their services firsthand. Right after Adalyn’s diagnosis, Hetzel recalled being given a binder with their logo on the front that laid out a “game plan of what our life was going to look like.”
That resource, called the Children’s Oncology Group Family Handbook, is funded by St. Baldrick’s and is given to newly diagnosed families around the country.
The St. Baldrick’s Foundation funds the Children’s Oncology Group Family Handbook.
Given her age, her father said he is cautious of not crossing the line in their advocacy and making her uncomfortable, and hopes that when she is older, she will understand the importance of sharing what she went through.
Jane Hoppen, director of family relations at St. Baldrick’s, said the family always has veto power. The foundation focuses on highlighting each child’s unique personality and interests to “serve as the face and voice of the foundation.”
For example, Adalyn, who loves chocolate-dipped croissants, will be featured on its social media for National Croissant Day.
“What we want for every kid who’s diagnosed is the ability to just go back and enjoy being a kid again,” Hoppen said.
Adalyn Hetzel, a 3-year-old from Southampton, loves croissants.