Blood banks across the Philadelphia region say donations are urgently needed this week as they brace for anticipated post-holiday blood shortages.
New Jersey Blood Services, whose coverage area includes South Jersey, declared a blood emergency on Tuesday, stating they had less than a two-day supply for the more than 200 hospitals they serve across New Jersey, New York, and Connecticut.
The American Red Cross of Southeastern Pennsylvania separately said Philadelphia and South Jersey, as well as the nation at large, are on the cusp of a blood shortage.
January is a difficult time for blood donations — so much so that President Richard Nixon signed a proclamation in 1969 declaring it “National Blood Donor Month.”
This year, a trifecta of seasonal illness, severe weather, and holiday disruptions has resulted ina significant decline in donations, said Chelsey Smith, a spokesperson for New Jersey Blood Services.
Flu cases surged in recent weeks. Meanwhile, Christmas and New Year’s Day both fell midweek, on days when the organization normally sees high collection. Blood donation levels dropped toalmost 40% below what is needed to meet hospital demand.
“We essentially experienced a mere total loss of midweek collections for two straight weeks, and that adds up very quickly,” Smith said.
The most urgent needs are for red blood cells and platelets.
The group urges people to donate at least once per season, emphasizing that blood is a perishable product. Red blood cells only last about 42 days after a donation. Platelets, which are especially critical for cancer patients going through chemotherapy, have a shelf life of just five to seven days.
“When those donations drop, it directly impacts our blood supply, and hospitals usually feel the effects of that pretty quickly,” Smith said.
Blood shortages are becoming more frequent
Blood shortages and emergencies have become more common following the pandemic, Smith said.
Fewer young people are donating, for starters, which she attributes to the loss of school collections during the height of COVID-19.
“We weren’t able to go into high schools and instill those lifelong values of donating blood when they’re young,” she said.
More people are also working from home, a challenge for the New Jersey organization thatused to rely heavily on corporate workplace blood drives.
New Jersey Blood Services declared a blood emergency last summer as well.
“Pre-COVID, blood emergencies were not quite as common. Post-COVID, they’re almost routine,” Smith said.
The American Red Cross also saw a lower number of people donate over the holidays than anticipated, according to Alana Mauger, a spokespersonfor the Southeastern Pennsylvania chapter.
Organizersreleased calls this week for donations in hopes of preventing a shortage, which they’re on the cusp of.
The group alsopartnered with the National Football League this month to offer a chance at winning a trip to Super Bowl LX to those who donate.
Saquon Barkley is participating in the campaign, sharing his own experiences as a blood donor.
“It only takes about an hour and once you realize in that short amount of time how much help it can bring — it’s a beautiful thing,” the Eagles running back said in a Monday news release.
New Jersey’s acting health commissioner, Jeff Brown, urged donors not to wait to donate.
“Schedule an appointment today or visit a walk-in center this week. Your donation can save a life,” he said in a statement.
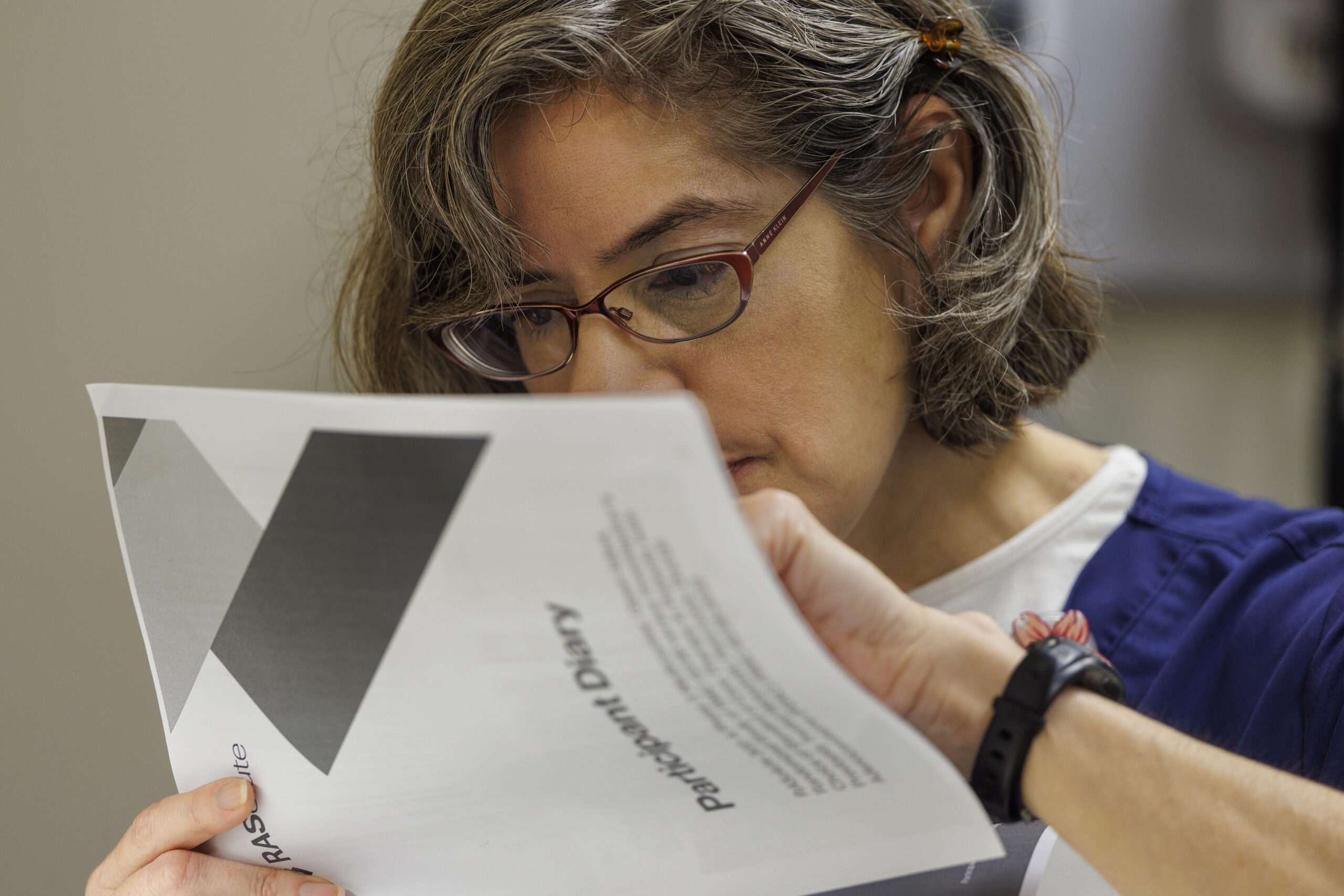
University of Pennsylvania researchers recently won a $25 million grant to see if they can fight heart disease with a game that promotesa healthy behavior — walking.
The intervention works by tracking how many steps a person takes each day and assigning points and levels accordingly. Participants get text messages with their daily tally.
The Penn team previously tested the concept in a clinical trial with 1,062 patients and found the approach increased participants’ activity by an average of nearly 2,000 steps daily.
Now, with funding from the nonprofit Patient-Centered Outcomes Research Institute, they hope to show that their game cannot only promote exercise, but can alsoreduce the incidence of heart events.
Dozens of studies have already shown that people who take more steps a day experiencefewer heart attacks and strokes. However, these findings have largely been based on observational data, which is not proof of a cause-and-effect relationship.
The Penn team will be using the $25 million grant to pursue the gold standard for establishing scientific causality: a randomized controlled trial. Patients will get divided into two groups — one gets to play the game, and the other does not — so researchers can compare their outcomes.
Theclinical trial involving 18,000 participants will launch in a year and a half and runfor roughly five years. Patients will be recruited through a partnership with the private healthcare system Ascension, which spans 15 states and the District of Columbia.
Scientists theorize that walking could help by reducing blood pressure, blood sugar, and inflammation. Activity may also improve the way muscles get oxygen from the blood, “so that your heart doesn’t have to work as hard,” said Alexander Fanaroff, a Penn cardiologist and one of the lead researchers on the project.
The researchteam will see whether the participants who had access to the gamesustained significantly fewer instances of stroke, heart attack, or heart failure.
Only people with an elevated risk of heart disease can take part in the trial.
Making walking into a game
As a cardiologist, Fanaroff spends a lot of time telling patients to exercise more.
It doesn’t always work.
“The hardest thing for people to do is change their behavior,” he said.
The Penn team has spent the last decade using concepts from behavioral economics — a field that combines psychology and economics to understand human decision-making — to hone an intervention to promote exercise.
The current program design, which works like a game, is the product of three previous clinical trials that showed the potential of Penn’s game-based approach to improving physical activity.
Here’s how it works:First, participants establish their baseline step count over two weeks, and then set a goal to increase their daily stepsby 33% to 50%.
Each week, patients are given 70 points — that’s 10 per day. Every day that they meet their goal, they keep their points. If they fail to keep up, they lose 10 points.
They move up or down levels each week, based on the cumulative points.
Patients need only to own a smartphone to participate, since their steps are tracked by thebuilt-in sensors now in most devices.
Daily results aredelivered through text.
“If you have an app on your phone, you might not look at it, but if you’re getting a text message every day, you’re engaged,” Fanaroff said.
Participants also identify a support partner, such as a family member or friend, who will get weekly email updates on how the person is doing in the game.
The study is entirely remote, with patients enrolling via a web platform.
Participants who are not sorted into the game approach will receive “usual care,” which consists of medical providers simply telling patients to be more physically active. They will also download a standard exercise app, which normally monitors their steps without turning it into a game.
This includes anybody who has ever had a heart attack or stroke, or received a stent, Fanaroff said. It also includes almost all people over 65 with multiple cardiovascular risk factors such as high blood pressure, high cholesterol, obesity, or diabetes.
“It’s not everybody, but it is a good-sized chunk of the population,” he said.
If successful, he hopes the evidence could convince insurers to fund programs that increase physical activity.
The Penn team estimates the game could be delivered for less than $50 per person.
“If it’s effective at reducing cardiovascular events, it would actually probably be cost-saving to the health system,” Fanaroff said.
He also hopes the results can guide doctors to bettercounsel patients.
“We just don’t know the best way to get people to increase physical activity at all, so all we wind up doing is telling people, ‘Physical activity is important for your health,’” he said.
Irene Blair was expected to have another six to eight months to live in June, after her pancreatic cancer rapidly advanced to stage 4 less than a year after her initial diagnosis.
A new drug being tested in clinical trials around the world, including at Penn Medicine’s Abramson Cancer Center, was the 59-year-old grandmother from Newark, Del.’s best hope for more time.
The drug belongs to a class of pharmaceuticals long considered the holy grail of cancer research. It is a KRAS inhibitor, capable of blocking a protein that fuels an especially deadly cancer. Only 13% of pancreatic cancer patients are still alive five years after their diagnosis, the highest mortality rate of all cancers.
Called daraxonrasib, the drug is not considered a cure. But the results emerging from clinical trials point to the first major advancement in decades for a devastating cancer usually caught in late stages. Former Nebraska Sen. Ben Sasse last week disclosed in a blunt social media post that he was recently diagnosed with metastasized, stage-four pancreatic cancer and is “gonna die.”
In recent months, the federal government has sped up the review timeline for the drug made by California-based company Revolution Medicines, Inc., based on early clinical trial results.
Across 38 patients in a phase 1 trial, the drug appeared to double the survival time for at least half of patients compared to standard chemotherapy, from roughly seven months to 15.6 months.
“In pancreatic cancer, for too long, we haven’t had effective therapies beyond just chemotherapy,” said Mark O’Hara, Blair’s oncologist who leads multiple clinical trials testing KRAS inhibitors at Penn.
Blair started the therapy through a phase 3 trial in July. Within three weeks, her cancer-associated pain went away.
In October, her tumors looked stable or decreasing on scans. Her most recent December scan showed her cancer had not progressed.
Aside from occasional facial rashes, she feels normal. It’s a big improvement from how she felt previously on chemotherapy, which caused her to lose 35 pounds and become so weak she couldn’t walk.
The question now is how long the therapy can remain effective. Blair seeksextra time to “start living life.”
She officially retired from her job in real estate in May and wants to travel, with trips planned to see family in California and Florida.
Holidays have been especially hard for her.
“You just wonder, ‘Will I be here next year?’” she said.
Irene Blair and her husband, Charles, at a beach in Delaware.
How does the therapy work?
Cancer researchers have worked to design a drug targeting KRAS, a protein that acts like a “gas pedal” for cancer growth when mutated, since its discovery in 1982.
The mutant protein is like a pedal stuck in the down position, driving uncontrolled proliferation — which tumors thrive on. These mutations are found in a quarter of human cancers, mostly aggressive cancers of the pancreas, lung, and colon.
Scientists finally succeeded in 2021, when the first drugs capable of blocking KRAS were approved by the FDA for lung cancer. Dozens of KRAS inhibitors are now invarious stages of development.
Daraxonrasib is one of the first tested for pancreatic cancer, a tumor type where nearly 90% of cases have these mutations. Also called a ‘pan-RAS inhibitor,’ it not only targets KRAS, but two other related proteins that drive cancer when mutated, HRAS and NRAS.
More than 90% of the 83 patients in a phase 1 trial saw their pancreatic cancer stall during treatment, and roughly 30% saw shrinkage.
While taking the drug, at least half of patients gained more than eight monthsbefore the cancer started progressing again.
The drug comes in pill form.
The drug comes in the form of three pills, taken daily at home.
The most prevalent side effect is a rash — 91% of patients in a phase 1 trial experienced this symptom, with 8% having severe cases. It often shows up on the face or scalp and is similar to acne, O’Hara said.
Diarrhea, nausea, vomiting, and mouth sores are other common symptoms.
O’Hara said these are manageable with medications for most patients and still allow them to have a better quality of life than chemotherapy.
“I want to be able to give KRAS inhibitors to all my patients right now,” he said.
Irene Blair of Newark, Del., meets with her doctor, Mark O’Hara, at her December appointment.
Looking forward
O’Hara runs multiple trials of KRAS inhibitors at Penn.
Some of them are testing the inhibitor as a treatment for patients with metastatic cancer after other options have stopped working.Another is evaluating its use in combination with chemotherapy as an initial approach.
“I’m looking for more tools to put in that toolbox, and I think this provides a new tool,” O’Hara said.
Ben Stanger, a gastroenterologist and scientist at Penn, has led experiments in mice that showed combining a KRAS inhibitor with immunotherapy may be more effective than using the former alone.
If this approach makes it into clinical trials as well, it could still take years to evaluate the safety and efficacy of the combination.
He believes KRAS inhibitors could be “a game-changer” for pancreatic cancer if approved, particularly if paired with other anti-cancer drugs.
“Goal number one would be to make pancreas cancer, instead of a death sentence, into a more ‘chronic’ disease that is treated over time,” he said.
In October, the drug was also one of the first selected for a new program that aims to accelerate review times for drugs from one year to as short as a month, potentially putting it on a faster path to approval.
Daraxonrasib, also known as RMC-6236, earned Breakthrough Therapy and Orphan Drug designations in 2025.
Limited options
When Blair first started having back pain around May 2024, she thought it was a pulled muscle from kickboxing.
She put a heating pad on the back of her chair and went on with life.
Afterher father had a stroke that July, she got it checked out at the hospital where he was admitted.
A day later, she was diagnosed with stage 2B pancreatic cancer.
“My first thought is, ‘I’m dying,’” she said.
Had she been diagnosed earlier, she would have retired early, instead of worrying about saving money.
Instead, she spent her final working year undergoing surgery to remove partof her pancreas, spleen, and several lymph nodes, followed by 12 difficultsessions of chemotherapy.
When she finished her last session in March, Blair’s scans showed no evidence of the cancer. But by late April, her back pain returned.
Two months later, more scans showed that the cancer was now considered stage 4, as it had metastasized to her liver, forming 10 to 15 new tumors.
Her best option was to enter a clinical trial of daraxonrasib at Penn.
Much to her relief, she was chosento receive the drug in July upon enrolling in a study in which half of patients are randomized to receive chemotherapy.
“It’s enabled me to start living again,” she said, but knows eventually the therapy will likely stop working.
In that case, doctors may try the standard chemotherapy — which usually works for three to four months — or test a different therapy based on her cancer’s genomic profile, O’Hara said.
For now, she described herself as “living scan to scan,” seeking as much time as possible with her son, grandchildren, and husband.
Irene Blair and her husband Charles, son Tom, daughter-in-law Kelsey, and two of her three grandchildren, Aidan and Madilynn.
Blair’s next evaluation is in February. She hopes it shows her disease remains stable, and she can stay in the trial.
Despite being one of the rockiest years yet for science — marked by millions of dollars in funding cuts and controversial shake-ups to the federal infrastructure — Philadelphia scientists still managed to celebrate many wins in 2025.
They also won national and international honors for work in physics, cancer research, and drug repurposing. And although no local scientists won a Nobel Prize this year, two at Monell Chemical Senses Center were recognized by its satirical counterpart, the Ig Nobel Prize.
Here are five notable Philly science wins from 2025:
1. Baby KJ is successfully treated with personalized gene editing therapy
Philadelphia-area child KJ Muldoon,now 16 months old, has already been called a “trailblazing baby” by the top scientific journalNature and recognized by the publicationas one of 10 people who helped shape science in 2025.
This international recognition came after his life-threatening genetic condition was successfully treated with a personalized gene editing therapy earlier this year by doctors at Children’s Hospital of Philadelphia and the Hospital of the University of Pennsylvania.
Baby KJ was born in August 2024 with a metabolic disorder that prevented his liver from being able to process protein. Called severe carbamoyl phosphate synthetase 1 (CPS1) deficiency, the disorder puts babies at risk of severe brain damage and is fatal more than half the time.
With few options to treat him, the CHOP and Penn team — led by doctors Kiran Musunuru and Rebecca Ahrens-Nicklas — opted for a gene-editing technology known as CRISPR to create a customized drug for KJ that would fix the genetic mutation that was driving his disease.
After receiving three doses, KJ was able to return home in June — ending his 307-day-long stay at the hospital. Though not a cure, the medication has dramatically improved his liver function and made the effects of his disease milder, doctors say.
2. Penn physicists share the Breakthrough Prize in Fundamental Physics
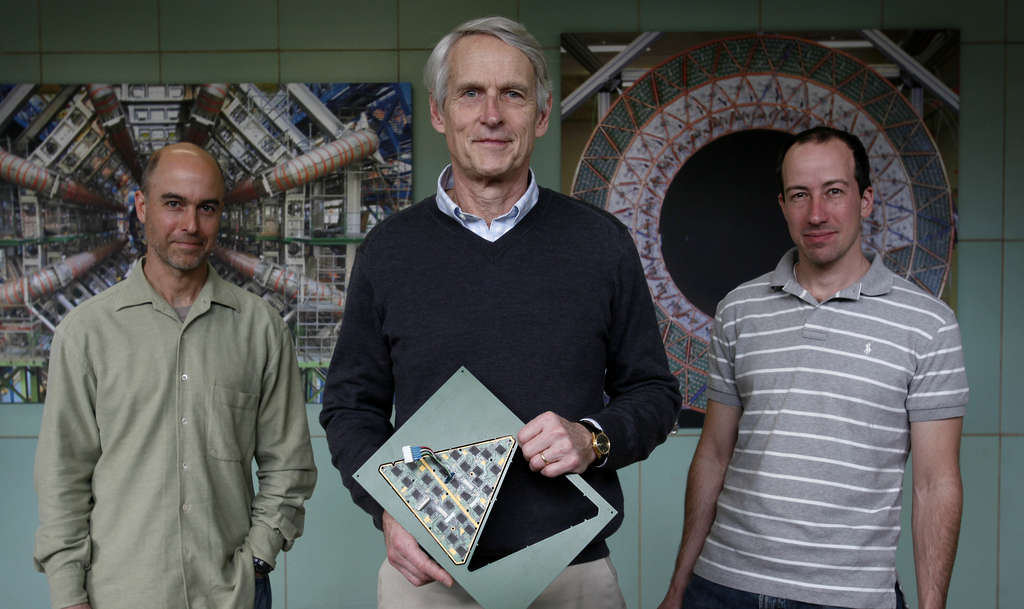
Penn particle physicists (from left) Joseph Kroll, Brig Williams, and Elliot Lipeles, pictured in 2011. They are part of the ATLAS research team that helped discover the Higgs boson, an elementary particle, and were honored with the 2025 Breakthrough Prize for their ongoing Higgs research.
This year, Penn physicists shared one of science’s biggest honors: the Breakthrough Prize.
They were among 13,000 scientists across more than 70 countries to be recognized for their involvement in particle physics experiments at the European Organization for Nuclear Research, known as CERN, in Switzerland.
These decades-long research collaborations have explored the fundamental structure of particles that make up the universe, using CERN’s Large Hadron Collider, a 17-mile-long particle accelerator.
The Penn team — consisting of more than two dozen scientists, including Joseph Kroll, Evelyn Thomson, Elliot Lipeles, Dylan Rankin, and Brig Williams — was specifically part of the ATLAS Experiment, which played a key role in the discovery of the Higgs boson particle, a critical particle in modern particle physics theory. The Higgs discovery helped confirm how fundamental particles acquire mass.
3. David Fajgenbaum honored for drug repurposing research
David Fajgenbaum was diagnosed with Castleman disease, a rare lymph node disorder with limited treatment options. When chemotherapy didn’t work, the third-year medical student worked with his doctors to discover that a medication approved for preventing organ rejection in transplant patients could help him, too.
Penn immunologist David Fajgenbaum received one of the nation’s oldest science prizes, the John Scott Award, this year for his pioneering work repurposing existing drugs for new uses.
He entered this field 15 years ago after a rare and deadly diagnosis of idiopathic multicentric Castleman disease nearly killed him. The disease had no approved treatment nor any treatment guidelines at the time.
Then a medical student at Penn, Fajgenbaum started collecting samples of his blood to test for abnormalities. The data helped him identify an existing drug called sirolimus — primarily given to organ transplant recipients — which has put him in remission for the last decade.
Now through his nonprofit Every Cure, Fajgenbaum has made it his mission to use AI technology to match available medications with rare, hard-to-treat diseases.
He published a case study in the New England Journal of Medicine in February, where his AI tool helped identify an off-label treatment for another patient with Castleman disease who, at the time, was entering hospice care after all available treatments had failed. As of that study’s publication, the patient has been in a yearslong remission.
4. Lilly Gateway Labs biotech incubator coming to Philly
Eli Lilly is opening a branch of Lilly Gateway Labs, an incubator for developing biotech companies, in Philadelphia, the Indianapolis company announced Wednesday. The site, in a new life sciences building at 2300 Market St. in Philadelphia, is the fifth in the United States for the pharmaceutical giant.
Pharmaceutical giant Eli Lilly & Co announced in November its plans to open a Lilly Gateway Labs site — an incubator for early-stage biotech companies — in Center City.
The incubator, which will be Lilly’s fifth in the United States, will span 44,000 square feet on the first two levels of 2300 Market St. Since the program’s launch in 2019, companies at the other locations (in Boston, South San Francisco, and San Diego) have raised more than $3 billion from investors toward more than 50 therapeutic programs, according to Lilly.
Lilly plans to house six to eight companies at the Philadelphia location, with the goal of welcoming the first startups in the first quarter of 2026.
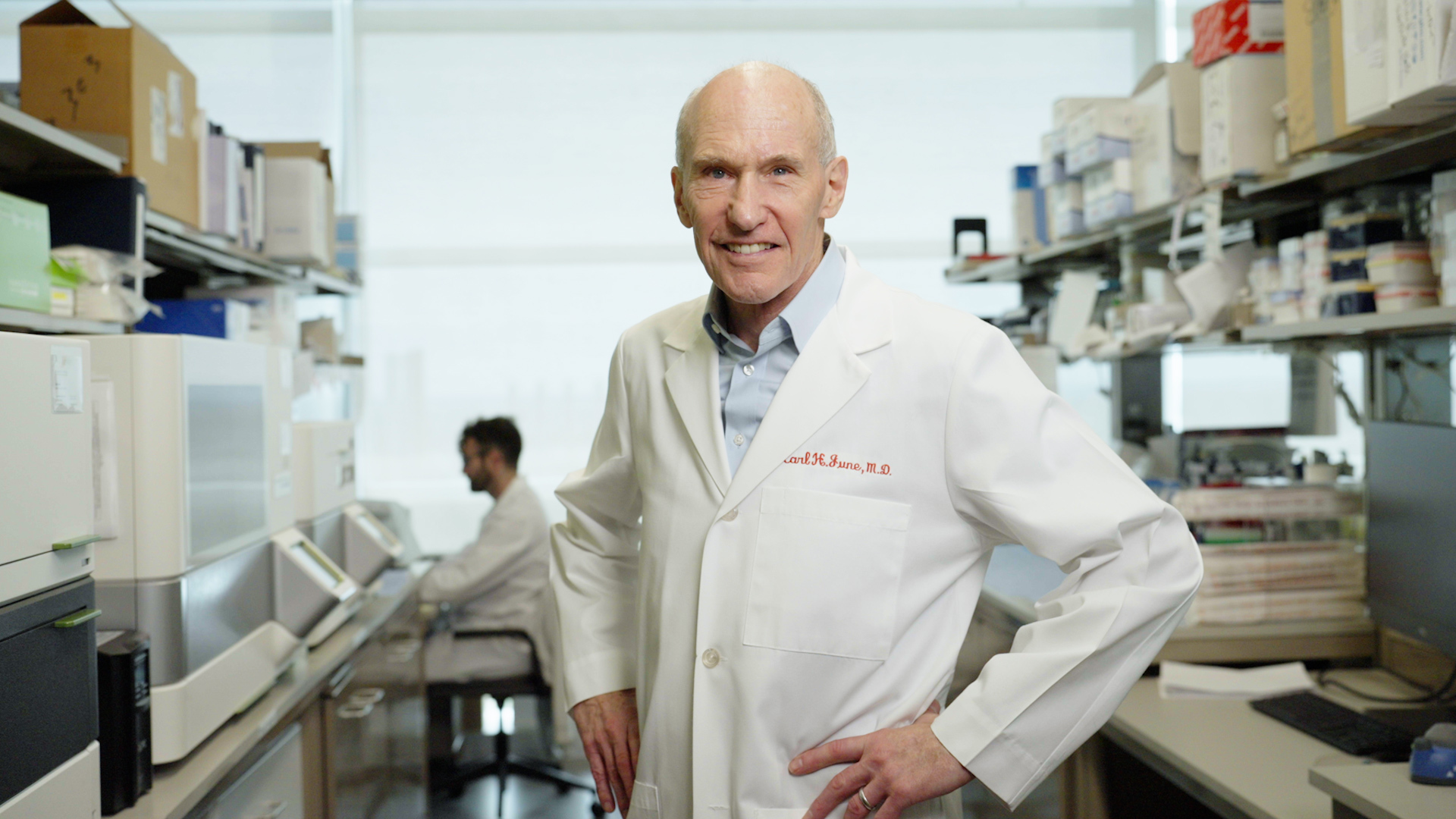
5. Carl June wins international honors for CAR-T research
Carl June won international prizes for his cancer research at the University of Pennsylvania.
Penn cancer scientist Carl June added two more international prizes to his trophy case in September for his pioneering work engineering the body’s immune system to fight cancer.
June is known for developing the first FDA-approved CAR-T therapy, an immunotherapy in which regular immune cells are genetically modified to become cancer-killing super soldiers. It has revolutionized treatment for blood cancers, saving tens of thousands of lives since its first use in a 2010 clinical trial he co-led at Penn.
Though his past work is what won him the inaugural Broermann Medical Innovation Award and the 2025 Balzan Prize for Gene and Gene-Modified Cell Therapy this year, his lab has remained busy, working on ways to apply CAR-T to solid cancers, enhance the therapy for lymphoma, and even re-engineer cells inside the body.
June has also made moves on the biotech front: A company he co-founded with the purpose of applying CAR-T to autoimmune diseases, Capstan Therapeutics, was bought by AbbVie this summer for $2.1 billion.
When Scott Edgell was discharged from the military after a service-related head injury at age 20, he thought he would resume life as normal.
But over the next four decades, the Lancaster Countyman was troubled by frequent migraines, memory problems, dizziness, irritability, and balance issues. Even everyday activities, like grocery shopping or eating at a restaurant, became overwhelming.
“I didn’t understand what was happening to my body,” said Edgell, who is now 57.
He realized the head injury he suffered while serving in the military was to blame after watching the 2015 movie Concussion, but struggled to find doctors who knew how to help him.
Just as he started to lose hope in late 2023, he learned abouta Jefferson Health program in Willow Grove for veterans and first responders with traumatic brain injuries (TBIs). The clinic provides physical and cognitive rehabilitation to participants over a three-week intensive outpatient program.
Edgell is among the estimated one in four veterans who have had a TBI. More than half a million U.S. military members have been diagnosed with the injury since 2000, according to the Department of Defense.
Many suffer TBIs as a result of combat-related incidents, exposure to blasts during explosions, training accidents, and vehicle crashes.
While some patients can recover completely, up to 30% of those with mild TBIs, also commonly called concussions — which account for the vast majority of TBI cases — experience long-term symptoms.
The lasting effects of TBIs are often overlooked among veterans because of the injury’s invisibility. Yet they can be life-altering, affecting employment, personal relationships, and overall quality of life.
Veterans with a TBI had suicide rates 55% higher than veterans without the injury, one study found.
Jefferson’s program, called the MossRehab Institute for Brain Health, was founded in 2022 and has treated roughly 100 patients. Itruns on donations — the biggest being from the veterans’ wellness nonprofit Avalon Action Alliance, which has provided $1.25 million annually.
Donations allow them to offer the program at no out-of-pocket cost to veterans and first responders, and cover housing, transportation, and meals during the three weeks.
“I walked in those doors at the lowest part of my life,” said Edgell, who participated in June 2024.
Though there’s no cure for his injury, the program has helped him rebuild his life.
“All you can do is learn to manage your symptoms,” he said.
Edgell and his family, including his wife Tami, stepdaughter Monica Bressler, son-in-law Kenny Bressler, and granddaughter Hayvin.
The program
Edgell entered the MossRehab program in June 2024 as part of a cohort of four.
The first step in his rehabwas learning about what was happening to his brain.
His accident occurred back in 1989, when a steel hatch swung shut and hit him in the back of the head during a training exercise at Fort Riley, Kan.
Doctors at the time provided memory exercises, mental health support, and physical rehabilitation to improve his gait, but nothing brought him back to baseline.
Edgell managed to push through his memory problems in college by putting in extra effort into studying, and ultimately became an electronics engineer.
However, it became harder to cope with the symptoms as he got older.
Even brief outings would exhaust him to the point of needing days to recover.
When his wife, Tami, would ask what she could do to help him, he wouldn’t know what to say.
One therapist at the program offered him a helpful analogy: If a normal brain is like a six-burner stove, then having a brain injury is like being down to only three burners.
“You’re trying to do everything with two or three burners that you would normally do with six, and your brain just becomes very fatigued and overwhelmed,” Edgell said.
The program teaches participants to adapt to their brain’s new way of functioning, whether through physical rehabilitation for symptoms such as dizziness, or cognitive rehabilitation to address issues affecting attention, concentration, memory, and mood.
“We’re basically retraining the brain to do something that it’s having difficulty doing because of an injury,” said Yevgeniya Sergeyenko, a physical medicine & rehabilitation physician and clinical director of the program.
Since treatment for TBIs revolves around managing the symptoms — which can vary widely between patients — the program has staff across an array of specialties that patients see throughout their three-week stay.
One provider helped Edgell, who was struggling to get more than a few hours of sleep a night, find medication to help him sleep.
A physical therapist, meanwhile, assisted with his balance and core structure, so he could walk and move around more easily.
Others taught Edgell exercises to improve his dexterity, speech, and memory.
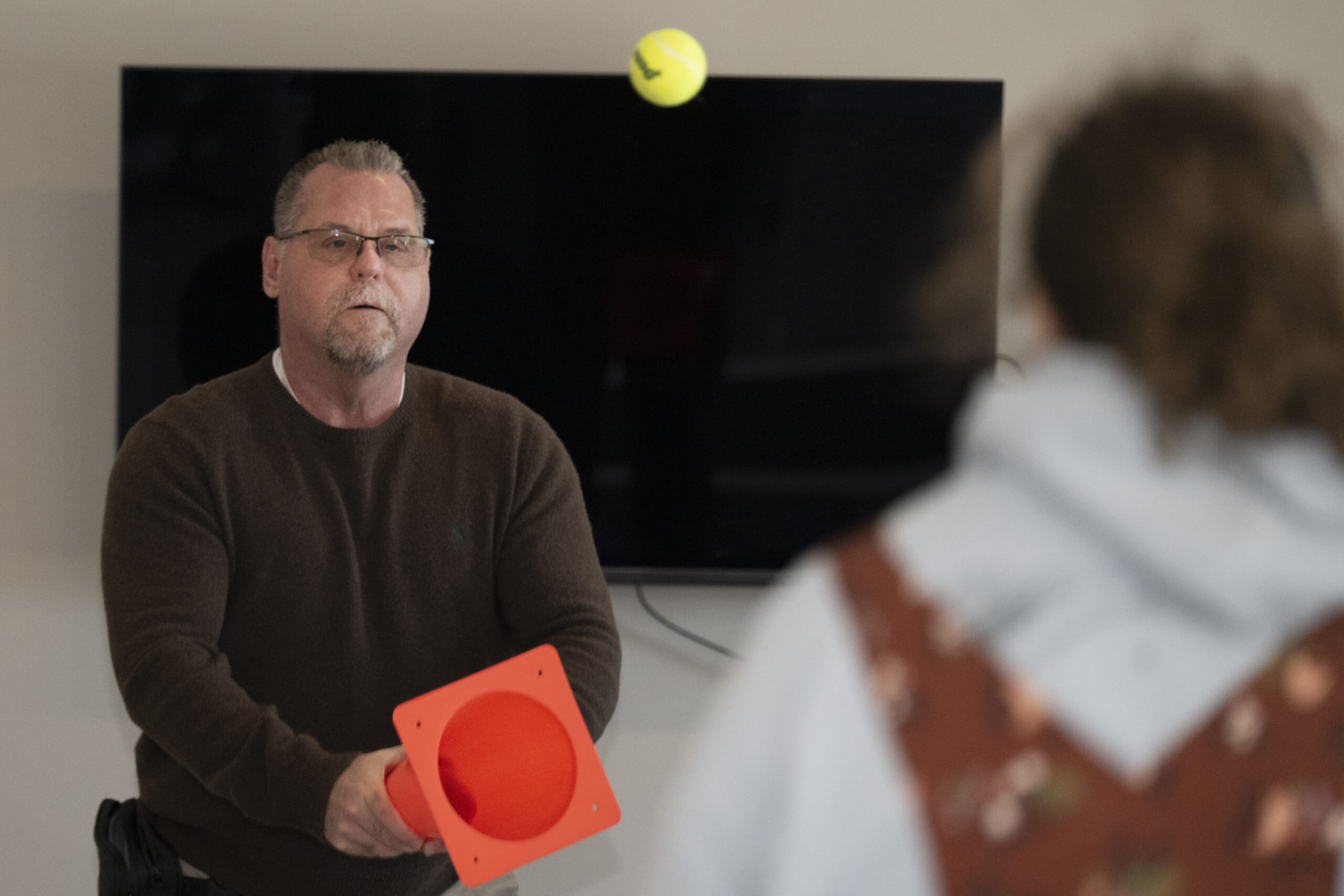
Army veteran Scott Edgell participates in a cohort session at the MossRehab Institute for Brain Health.
Some forms of therapy were less conventional.
There was horticultural therapy — a therapy that involves working with plants — which Sergeyenko said has been shown to lower blood pressure and is intended to help with emotional regulation.
Patients also did yoga and other mindfulness and movement activities intended to calm the nervous system.
Edgell said yoga wasn’t his favorite, but he found art therapy helped him communicate more openly.
One of the exercises at the start of the program asked himto draw a tree. He drew one that “was not doing very well,” he said.
At the end of the three weeks, he drew a lush version full of leaves. The framed drawing now hangsin his dining room.
“I look at that everyday to see where I came from,” he said.
Army veteran Scott Edgell shows drawings of trees representing himself during a cohort session at the MossRehab Institute for Brain Health.
Outcomes
Program organizers say returning to a pre-injury baseline is not always a realistic goal.
“There’s not a medicine that you can give that’s going to make all of your brain injury symptoms subside,” said Kate O’Rourke, the program director at the clinic.
The program aims toimprove function and quality of life.
As of September, the last time outcome statistics were compiled, 82 patients had gone through the three-week intensive. Sixty-five percent saw significant reduction in their symptoms, as measured bytheir Neurobehavioral Symptom Inventory scores — which assesses a patient’s severity of neurobehavioral symptoms from 0 to 88. The average reductionwas 13.26 points.
Ninety-nine percent of patients reported that they personally felt they improved after the program.
Current patients (Jeff Todd Malloch and Jessica Mack) and Army veteran Scott Edgell participate in a cohort session with his therapy dog, Lars, at the MossRehab Institute for Brain Health.
Edgell regularly reaches out to staff for advice, and meets with the program’s alumni in monthly conference calls.
He still has bad days sometimes, but he’s able to manage them better.
Before, when he would go to a grocery store or restaurant, he would become overwhelmed by the noise, lights, and commotion.
“I couldn’t catch my triggers before I fell off the cliff,” Edgell said.
He was only able to leave the house four to five times a month.
Working with a service dog at MossRehab inspired him to get one of his own.
Now, when he starts to react, a golden doodle named Lars will nudge him, giving him a moment to let his brain calm down.
Edgell and his service dog, a golden doodle named Lars.
Today, he’s able toleave the house more frequently and for longer.
He and his wife have reconnected with friends and engaged more in social activities.
“I still get tired, I still need breaks, but my recovery time is a lot faster, and it’s not nearly as devastating,” Edgell said.
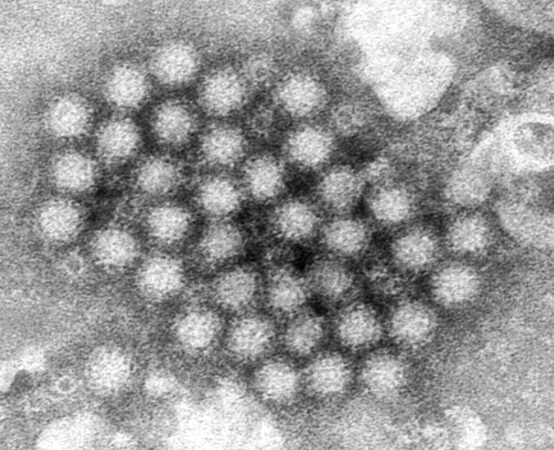
A South Jersey school was hit with an outbreak of gastrointestinal illness last week, as cases of norovirus, a common stomach bug, recently surged nationwide.
Camden County officials could not definitively say the illness was norovirus, since no lab testing has been done. However, they noted it was a candidate.
“The symptoms, infectious period, and incubation periods seem to be consistent with norovirus,” said Caryelle Vilaubi, director of the Camden County Department of Health and Human Services.
The school in Haddonfield, which officials declined to identify further, first reported a spike in gastrointestinal symptoms among students on Dec. 10, followed by an increase the next day.
Cases have since fallen dramatically, Vilaubi said, as outbreak control measures — including use of disinfectants, sending sick students home, and promoting proper hand hygiene — have been put into place.
They’re hoping to end the outbreak in the school community as early as next week, if they can go without new cases for four days, she said.
A variety ofsources can cause gastrointestinal illness, including viruses, bacteria, and parasites. Norovirus is one of the common culprits this time of year.
“We typically see a spike from November through April, not just in Camden County, but throughout the state, and often throughout much of the country,” Vilaubi said.
The highly contagious virus can spread through close contact with an infected person or with contaminated food, water, and surfaces. Symptoms usually include nausea, vomiting, diarrhea, and stomach pain, and start 12 to 48 hours after exposure.
Most people will feel better after one to three days.
Here’s what to know about the virus:
How can you protect yourself against norovirus?
Norovirus is a “hardy and resistant virus,” Vilaubi noted, making it especially hard to clean off. Hand sanitizers are not effective against it.
It is also relatively resistant to heat, able to survive temperatures up to 145°F.
People should make sure to regularly disinfect high-touch surfaces such as doorknobs, keyboards, and light switches.
How long does norovirus last in adults?
Though people will usually feel better after one to three days, they are still highly contagious for a few days after.
“If your child begins to show symptoms, please keep them home until at least 48 hours after symptoms resolve to prevent further spreading the illness,” Virginia Betteridge, liaison to the Camden County Department of Health and Human Services, said in a Dec. 12 news release.
Those infected with norovirus should avoid contact with others as much as possible during this period.
How to treat norovirus at home?
There is no cure or specific treatment for norovirus. The advice generally is to let the virus run its course.
To ward off dehydration, people should make sure to drink lots of fluids to replace what’s lost from vomiting and diarrhea. Taking small sips of water and sucking on ice chips may be easier on an upset stomach.
People can also consider drinking clear broths, noncaffeinated sports drinks, and oral rehydration solutions, which are available over the counter.
Drinks that contain a lot of sugar, including soft drinks and certain fruit juices, can make diarrhea worse and should be avoided.
How does norovirus spread from person to person?
Norovirus is considered highly contagious, as only a small amount of virus is needed to infect someone.
People contract it by accidentally touching tiny particles of stool or vomit — where the virus is primarily shed — from an infected person and getting them in their mouths.
These particles easily contaminate hands, surfaces, food, or water.
Several Philadelphia-area violence prevention efforts will benefit from nearly $3 million in newly released state funding to help hospitals address a leading cause of death and injury.
The new funding for hospital-based violence intervention programs (HVIP) was announced by Pennsylvania Lt. Gov. Austin Davis on Wednesday at Penn Presbyterian Medical Center. One of the recipients, the Penn Trauma Violence Recovery Program, is based at the Penn Medicine hospital in University City.
Other local awardees includeTemple University Hospital in North Philadelphia and the Philadelphia-based nonprofit Urban Affairs Coalition. The coalition received funding on behalf of the Chester Community Coalition to relaunch a program that had been at the now-shuttered Crozer-Chester Medical Center.
The University of Pittsburgh Medical Center also received funding. The amounts awarded to each program were not announced.
The Pennsylvania Commission on Crime and Delinquency, which Davis chairs, received 15 applications in total seeking nearly $12 million in funding — four times what was available.
“Addressing the epidemic of gun violence is a top priority for our administration,” Davis said.
Lieutenant Governor Austin Davis speaks at a press conference announcing the $3 million in grants for hospital-based violence intervention programs.
The programs aim to connect patients at risk of repeat violence with resources while they are in a hospital, so they leave with a safety plan. Services can include long-term community-based case management, mentoring, and home visits.
Since the first HVIP was established in the mid-1990s, dozens have spread around the country and abroad, including in Philadelphia.
Several local institutions have these programs, including Temple Health, Children’s Hospital of Philadelphia, Penn Medicine, Jefferson Health, and Drexel University. The City of Philadelphia, in conjunction with the area’s Level 1 trauma centers, launched an HVIP Collaborative in 2021.
Studies have shown these programs reduce rates of repeat violent injuries and recidivism among participants.
After shootings spiked during the COVID-19 pandemic, gun violence is now declining in Philadelphia. As of July, shootings for the year were at their lowest total since at least 2015.
Davis noted that Philadelphia has seen a 15% decrease in homicides this year, with roughly four in fivegunshot victims surviving their injuries.
The new funding will allow the Penn Trauma Violence Recovery Program to increase its community presence and mental health programming, said its director, trauma surgeon Elinore Kaufman.
Through her experience treating victims of violence, she has learned that injuries can be deeper than the physical wounds.
The program was launched to address social factors often involved in violence by providingpsychosocial support and connecting patients with services to help with education,job training, and housing.
“We’ve worked with patients long enough now that we have high school graduation photos, we have baby pictures,” Kaufman said. “We have patients who want to give back and have joined our patient advisory board to help push us forward.”
Wistar Institute scientist Maureen Murphy wants to solve a decades-long mystery: Why is ovarian cancer often resistant to hormone therapy?
In a recently published study, she shared a new theory as to why treatments designed to block or remove hormones, known as hormone therapy, often fail in ovarian cancer — and a potential approach to make them more effective. Such therapies have cut the risk of death from certain breast cancers by a third and reduced the odds of a recurrence by half.
She pinpointed a problem facing hormone therapy — the vast majority of ovarian cancer cases have mutations in a key protein called p53.
Her study, published last month in the medical journalGenes and Development, suggests that mutations in p53, a protein that normally works to stop tumors from growing, drive resistance to hormone therapy and that their effects could be reversed.
“There are very few drugs that treat it,” Murphy said.
Her p53 mutation discovery led to her identifying a drug currently in clinical trials that’s promisingin a small number of cases. Murphy wants doctors to start testing the combination of the drug and hormone therapy in ovarian cancer.
If the approach makes it into a clinical trial, it would still take years to evaluate the safety and efficacy of the combination. Most treatments tested in clinical trials do not become standard practice.
“For ovarian cancer, the treatment hasn’t changed much in the last 20 years, and so we really do need new treatments,” Murphy said.
How does hormone therapy work?
Hormones are like the body’s mail service.
These chemicals carry messages to cells throughout the body, controlling mood, growth, reproduction, and development.
Tumors can co-opt hormones for their own purposes using proteins called receptors, which act like mailboxes to receive the messages.
Breast cancers, for example, often have estrogen receptors so that they can receive more of a hormone called estrogen. Similar to how bodybuilders use steroids to build muscle, tumors use estrogen to grow and divide.
“Breast and ovarian tumors love estrogen. They grow on it,” Murphy said.
Hormone therapy works by either blocking the receptors from receiving the hormones, or reducing the amount of hormones in the body altogether.
One of the first hormone therapy drugs for cancer, tamoxifen, was approved in the U.S. in 1977 to target the estrogen receptor in metastatic breast cancer.
In this study, Murphy looked at fulvestrant and elacestrant, two anti-estrogen drugs approved for breast cancer.
More than 70% of cases of the most common type of ovarian cancer express estrogen receptors, making them theoretically a good target for hormone therapy, if the p53 problem can be fixed.
Solving the mystery
In her first professor job at Temple’s Fox Chase Cancer Center in 1998, Murphy chose to study the tumor suppressor protein p53, with a focus on genetic variants in women of African and Ashkenazi Jewish descent that put them at risk of cancer.
Decades later, Murphy expanded her focus at Wistar to look at hundreds of genetic variants of the protein found in the general population, in an effort to predict people’s risk of cancer.
Murphy started to wonder whether mutant p53 controlled the function of the estrogen receptor, and how it might affect the response of tumor cells to hormone therapy.
That led her team to look atovarian cancer because of its high prevalence of p53 mutations. They used cell lines and a lab model to mimic stage 3 and 4 tumors.
The researchers found that when mutant p53 was bound to the estrogen receptor in these models, it inhibited part of the estrogen receptor’s activity, driving resistance to hormone therapy.
By simply removing the mutant protein, tumors “responded great” to the hormone therapy, Murphy said.
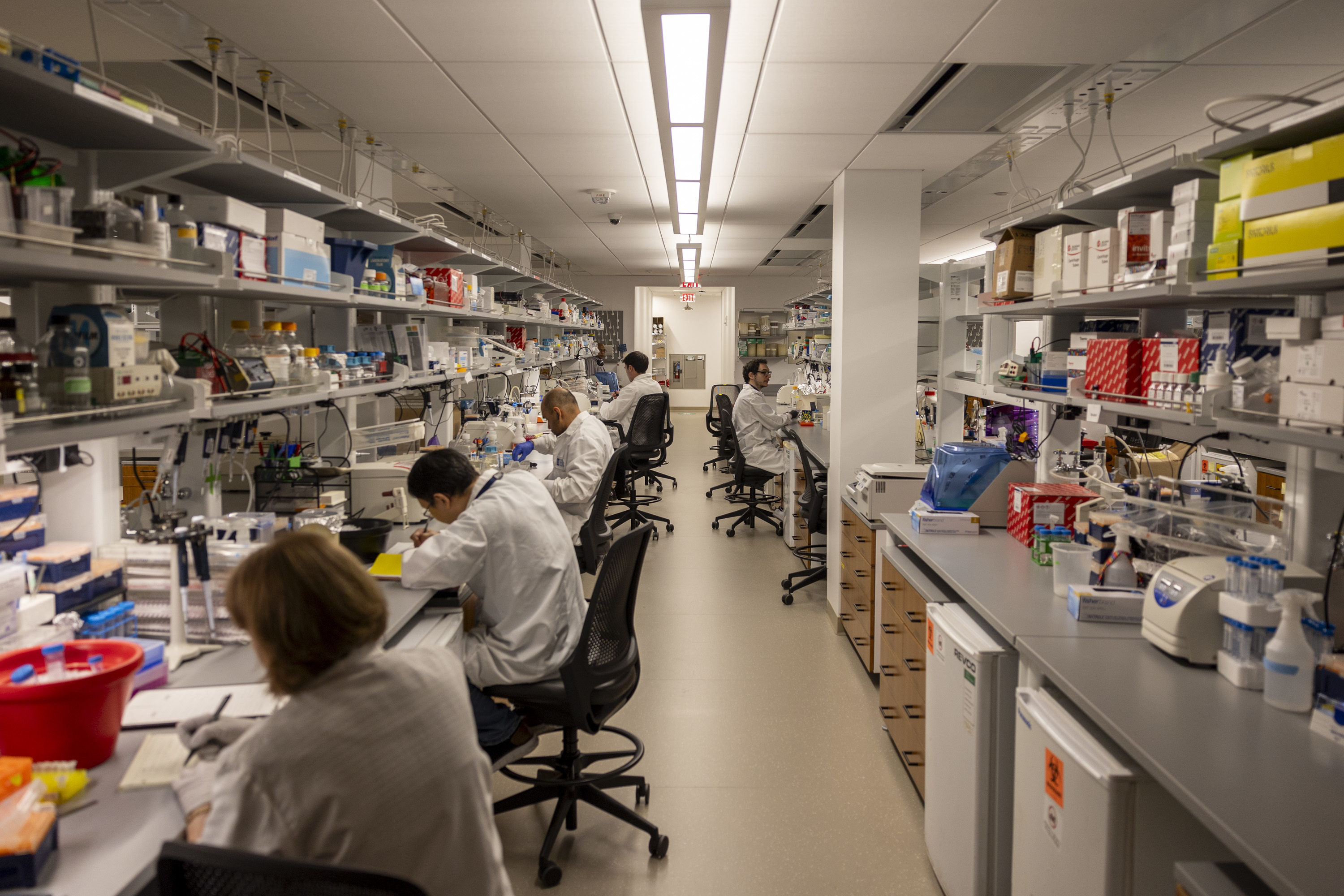
A lab at the Wistar Institute in Philadelphia.
Hope for hormone therapy?
While it’s easy to take away p53 in the lab, it’s not as easy in a patient.
There is, however, a promising drug currently being tested in clinical trials. Called rezatapopt, it can convert mutant p53 into a normal-functioning version of the protein.
It works for one particular mutation, Y220C, found in roughly 4% of ovarian cancers.
Murphy’s team foundadministering rezatapopt alongside hormone therapy led to 75% shrinkage of ovarian tumor models, versus 50% shrinkage when the hormone therapy was given alone.
This finding lined up with rezatapopt’s early data from clinical trials.
“For reasons we didn’t understand, women with ovarian cancer were responding best to this drug,” Murphy said.
Nineteen out of 44 women treated with rezatapopt alone saw their tumors shrink, with one even having a complete response, according to recent interim results from a phase 2 trial.
Murphy hopes this paper will prompt clinical trials to test rezatapopt in combination with anti-estrogen therapy.
However, since rezatapopt only targets one p53 mutation, this approach is limited to a small subset of patients. Murphy hopes that more drugs can be developed thatfix other mutant forms of p53 seen in ovarian cancer.
Murphy’s findings make sense conceptually and present a “promising avenue for future clinical trials,”said Tian-Li Wang, the head of the Molecular Genetics Laboratory of Female Reproductive Cancer at Johns Hopkins University, who was not involved in the Wistar study.
A caveat is that the study looked at a limited number of cell lines, she said.
She thinks the results should be confirmed in cases of ovarian cancer that have other types of p53 mutations to see if it could be applied more broadly.
“[I’m] really interested to see if the approach can benefit patients,” Wang said.
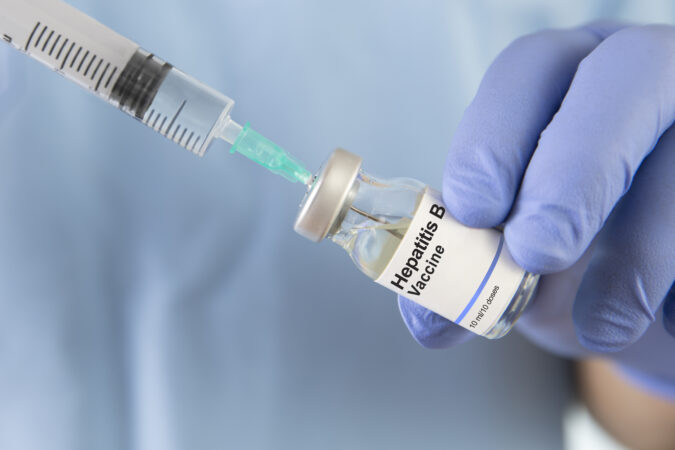
The nation’s top vaccine advisory panel is expected to debate whether to delay the first dose of the hepatitis B shot on Thursday.
The immunization, developed in Philadelphia and long recommended for all U.S. infants at birth, protects against a disease that can do permanent damage to the liver, and for which there is no cure.
The shot is widely considered safe and effective, but who should receive it, and when, has come under scrutiny by President Donald Trump’s administration.
The Advisory Committee on Immunization Practices (ACIP), an independent panel of experts reconstituted this past summer to include several vaccine skeptics, had tabled a vote on this topic in September. It is now scheduled to spend Thursday discussing the vaccine, according to a draft agenda of the group’s two-day December meeting.
Vaccine experts and patient advocates have previously advocated against delaying the birth dose, citing concerns that unvaccinatedchildren could be at risk of contractingthe highly contagious virus.
Starting in 1991, the first dose of the hepatitis B vaccine has been universally recommended for all newborns within 24 hours of birth. Rates of infection among children and teens have since dropped by 99%.
Prior to the universal birth dose recommendation, about half of infections in children were acquired from mothers infected with the virus, the Centers for Disease Control and Prevention found.
The virus spreads through contact with blood and other body fluids.
The virus can be transmitted from mother to baby, as well as through a variety of household sources, such as personal items like toothbrushes and razors that become contaminated with blood.
The virus cannot be spread through casual contact such as hugging, touching, or sharing utensils, but it can be spread through open wounds.
Patients can take antiviral treatments to help control the virus, but there is no cure.
The panel has previously considered delaying the birth dose until one month of age.
ACIPpreviously debated delaying the first dose of the vaccine until one month of age for most babies.
Some members had suggested the dose for newborns should instead be given only to the populations most at risk.
The ACIP considered recommending doctors vaccinate only those newborns whose mothers test positive for the virus, and having the other babies wait a month for their first dose.
Trump separately stated in a news conference, without citing scientific evidence, that he thinks newborns should no longer universally receive the shot and children should wait until age 12. Experts criticized Trump for incorrectly suggesting that hepatitis B is only transmitted sexually.
Experts are concerned about a potential change to the guidelines.
Experts worry that delaying the vaccine could affect its ability to prevent transmission of the virus from mother to baby. “If you wait longer than 24 hours, then the vaccine doesn’t work as well,” Chari Cohen, president of the Hepatitis B Foundation, told The Inquirer in an interview earlier this fall.
Even if the ACIP were to recommend vaccinating only babies whose mothers have the virus, some cases could be missed. Universal testing for the virus has been recommended since the 1990s, but 15% to 16% of women still do not get tested.
Such a policy also would not account for other exposures. Su Wang, a New Jersey physician who treats patients with hepatitis B and herself has the disease, told The Inquirer earlier this year that she likely caught hepatitis B as a child living with her grandparents. Her parents tested negative. “There are a lot of exposures that we aren’t testing for,” she said.
The vaccine is a Philadelphia success story.
The hepatitis B virus was first discovered by Baruch Blumberg, a scientist at Fox Chase Cancer Center, in 1967.
He went on to win a Nobel Prize for that work, and later cocreated and developed the vaccine,which continues to be manufactured in and around the region.
The Hepatitis B Foundation is also locallybased, in Doylestown.
Philadelphia didn’t take home any Nobel Prizes this year, but work illuminating how babies respond togarlic-flavored breast milk at Monell Chemical Senses Center did get recognized by its satirical counterpart, the Ig Nobel Prize.
Julie Mennella, a longtime scientist at the center in West Philadelphia, and Gary Beauchamp, Monell’s former director, won the prize earlier this fall for their 1991 study published in the academic journalPediatrics that disproved popular folklore around breastfeeding.
Their study examined whether eating garlic would flavor a mother’s breast milk and, if so, how a nursing baby would react to it.
At the time, breastfeedingwomen were often told to eat bland foods, for fear their babies would reject strong flavors. However, the study’s results showed the opposite: Babies savored the garlic-flavored breast milk.
“That simple, elegant study really showed how one of the first ways we learn about foods is through what our mothers eat,” Mennella said.
These early life experiences shape food preferences and influence cultural food practices around the world, she emphasized. Babies whose mothers come from cultures in which garlic is a defining flavor would have experienced garlic long before their first meal.
Mennella spoke with The Inquirer about the implications of her Ig Nobel Prize-winning work and her decades of research on flavor sciences and early nutritional programming.
The following conversation has been lightly edited for length and clarity.
What did you discover in your Ig Nobel Prize-winning study?
We found in this study that not only did the milk get flavored with garlic, but contrary to a lot of the folklore, the babies actually liked it. They nursed longer when the milk was garlic-flavored than when it was bland and devoid of garlic.
We went on to show that when women eat garlic, the flavor of amniotic fluid also gets altered.
Through these first exposures, babies are learning about what mom is eating, what mom has access to, and what mom likes before their own first taste of solid food.
What is the takeaway for breastfeeding mothers?
Eat the healthy foods that you enjoy because your baby’s going to learn about the food. Food is much more than a source of calories. In many cases, it defines who we are as a people.
What other flavors have you studied?
A wide variety of flavors, from vanilla to even alcohol if a woman drinks it, get transmitted and flavors the milk. If women smoke, the tobacco flavor does, too. So it’s not only what you eat, but what you breathe.
Why is it important for babies to learn about food this way?
There’s a great story about the European rabbit (an animal that nurses), where they tagged the mother’s diet with juniper berry. What they were able to show is that in a group where the mothers ate juniper berry during either pregnancy or lactation, once those young rabbit pups left the nest, they were more likely to forage on juniper berry.
So, she’s telling them, ‘These are the foods that are out there. I’m eating them. They’re safe.’ It’s really a very elegant, sustainable behavior, how moms transmit this information about the foods in the environment. She’s teaching her young and giving them an advantage early on.
How long do these flavors last in the milk?
Depending on the size of the chemical, some will get in fast. Garlic gets in a couple hours after the mom eats it, and then if she stops eating, it’s out of the milk like four or five hours later. The sensory experience of that baby is changing throughout the course of the day, day to day, depending on what she eats.
What research have you been up to since?
I’ve gone into so many different directions of looking at not only early flavor learning, but also nutritional programming. I also looked at the taste of medicine in children, looking at individual differences because taste is the primary reason for noncompliance. Children have a harder time because they can’t encapsulate the bad taste in a pill or tablet, so liquid medicines are particularly difficult.
One study where we looked at variation in the taste of pediatric Motrin (among adult participants) was really interesting. Some people experience a tingle when they taste it. Others don’t. It makes you think that how one child tastes Motrin isn’t like how another does. If you don’t experience the tingle, or this burning sensation, all you taste is a sweet liquid, and those are the children that may be at risk of over-ingestion.
What is your favorite project that you have worked on since the garlic study?
I serendipitously found that another flavor that gets transmitted is alcohol, and that became a whole new area of research.
We found that when women just have the equivalent of one or two glasses of wine or beer, not only did the alcohol get transmitted, but it flavored the milk. That became a lead article in theNew England Journal of Medicine.
At that time, there was talk about a folklore that women should drink when they’re breastfeeding, so they would make more milk. And contrary to that folklore, they actually made less milk.
How did it feel to win an Ig Nobel?
It was so nice to celebrate science. That’s really what that award does: It uses humor to teach about science.