Montgomery County health officials on Saturday warned residents of a possible measles exposure at two locations in the county, after confirming another case of the highly contagious disease.
A person infected with measles visited a car dealership and a convenience store in Royersford and Limerick earlier this week, officials said.
The case is connected to another in the county that was confirmed earlier this month, said Richard Lorraine, the medical director of the Montgomery County Health Department.
The original measles case was linked to a larger outbreak centered on a college in Florida, Lorraine said. A person infected with measles connected to that outbreak then traveled to Montgomery County and visited an urgent care center in Collegeville on Jan. 29, he said.
Later, two people in their household, who live in Montgomery County, contracted measles; they were already quarantining by the time they developed symptoms, Lorraine said.
The latest case, announced on Saturday, was in an adult who had visited the Collegeville urgent care clinic at the same time as the original patient, Lorraine said. That person developed symptoms about 20 days after exposure to the virus, Lorraine said. The virus can incubate for up to 21 days before symptoms appear.
All of the Pennsylvania residents who have contracted measles so far this year, including the Montgomery County cases, were not vaccinated against the disease.
What to do if you were exposed to measles
People who were at the following Montgomery County locations during the following time periods may have been exposed to the virus, which can linger in the air for up to two hours, officials said.
Nissan 422 of Limerick at 55 Autopark Blvd. in Royersford:
Wawa at 579 N. Lewis Rd. in Limerick:
People are generally considered protected from measles if they were born in 1957 or earlier or have had two doses of the measles, mumps, and rubella (MMR) vaccine, or the recommended number of doses based on their age, health officials said.
People are also considered protected if they have undergone lab testing that confirms they have already had the disease or have immunity to it.
People who are not fully vaccinated or do not have immunity to measles and were exposed to the virus should call their doctor or the county public health office. The office can be reached at 610-278-5117 or after hours at 610-635-4300.
Lorraine said that county health officials are working to track anyone who worked at or visited the Wawa and the car dealership earlier this week.
Once health officials identify people who passed through those locations, he said, they check to ensure they are vaccinated for measles. People with two doses of the MMR vaccine are of little concern, since the vaccine is about 98% effective at preventing disease, Lorraine said.
The county can also test residents without documentation of vaccination for measles immunity. People without immunity can get an MMR vaccine within about 72 hours of exposure to the virus that can prevent them from contracting measles, Lorraine said.
“For those folks who don’t have an immune status, and don’t get the MMR, they do need to quarantine for up to 21 days afterward, because that’s how long the incubation period is,” he said.
People without immunity who were potentially exposed to the virus should observe themselves for symptoms during that period. Symptoms include fever, an unexplained rash, a cough, congestion or a runny nose, and red, watery eyes.
Health officials said people who develop measles symptoms should stay home and call a doctor immediately. They should also call ahead to any healthcare providers they plan to visit to protect staff and other patients from the disease.
Measles in the Philadelphia area
As of Saturday, Pennsylvania health officials said they have confirmed 11 cases of measles in state residents, a Pennsylvania Department of Health spokesperson wrote in an e-mail.
Seven Lancaster County residents had been infected, as well as three in Montgomery County and one in Chester County. Two more cases were identified in out-of-state residents who visited the area: one in Montgomery County and one in Chester County.
Chester County health officials did not immediately return a request for comment Saturday.
Lorraine said it is imperative for area residents to get vaccinated against measles, which can cause severe complications including pneumonia and brain infections. About 1 to 3 of every 1,000 children who contract measles will die, according to the Centers for Disease Control and Prevention.
Infants and children under 5 years old, adults over 20, pregnant women, and people with weakened immune systems, including patients with leukemia or HIV, are at particular risk for complications from the disease, according to the CDC.
“Like every other illness, measles can be mild, it can be severe. But that’s the reason why we want to immunize: We want to mitigate the possibility of severe illness. We really don’t want to even take a small chance on that,” Lorraine said.
Almost 250 years ago, George Washington created America’s first mass immunization mandate, relying on science to protect public health.
Oh, how times have changed.
Back then, smallpox had just helped end the Continental Army’s invasion of Canada. Despite making it all the way to Quebec, thousands of soldiers contracted the disease. Washington feared the same would happen to his own troops, fresh from their surprise victories at Trenton and Princeton. As Washington wrote at the time, “Necessity not only authorizes but seems to require the measure, for should the disorder infect the Army, in the natural way, and rage with its usual Virulence, we should have more to dread from it, than from the sword of the enemy.”
The inoculation methods of Washington’s time were crude. No genuine vaccine existed. Instead, scabs or pus were taken from someone infected with smallpox and then placed into scratches or small wounds. Another option was to inhale it. Either way, those who experienced variolation inevitably developed fevers, rashes, and other symptoms of smallpox. At least 1% of those who received it died. Still, without his tough choice, the Continental Army might have failed entirely, and America with it.
These days, safe vaccines are available for diseases that ravaged our ancestors. Forms of influenza, hepatitis, chickenpox, polio, rubella, mumps, measles, and many other diseases can now be prevented. The smallpox virus that Washington dreaded has been eradicated.
The quality and availability of vaccines are a modern miracle, one that all humanity should be proud of.
Yet, according to data from the Centers for Disease Control and Prevention, vaccination rates for measles in the U.S. are declining, and the number of cases is climbing. More and more parents are opting against vaccination for their children, which gives these diseases room to spread.
Pennsylvania, New Jersey, and Delaware have all slipped below the 95% vaccination rate the CDC says is necessary to keep measles outbreaks at bay. Despite being nearly eliminated in 2000, rates have reached their highest levels in decades.
A sign is seen outside a clinic with the South Plains Public Health District in February 2025, in Brownfield, Texas.
According to CDC data, more than 90% of infections occur in people who are either unvaccinated or have unknown inoculation status. Given this group makes up less than 10% of the overall population, that’s a staggering concentration of sickness. It also isn’t a surprise — the vaccines work.
Parents offer a range of justifications for refusing vaccinations. Some cite religious faiths that discourage inoculation. Others feel that the schedule of shots is too concentrated. A number of them mention debunked fears of shots “causing autism.”
In some cases, existing health issues may lead to medical professionals advising against vaccination. (These children rely on what scientists call herd immunity for protection, and are endangered by rising rates of voluntary refusal.)
It doesn’t help matters that Health and Human Services Secretary Robert F. Kennedy Jr. is a leading skeptic of both vaccines and modern medicine. Kennedy has strong opinions about public health based on no formal medical training.
This is the kind of privileged ignorance that can only thrive in a post-vaccine world, where mass immunization has dramatically changed life for the better.
In 1900, 30% of all U.S. deaths occurred in children under the age of 5. In 1915, the infant mortality rate was 100 out of every 1,000 live births. As late as 1952, a polio outbreak killed more than 3,000 people.
Unfortunately, rising vaccine refusal rates may bring some of this suffering back. While city health officials urge calm in the wake of a possible exposure at Philadelphia International Airport earlier this month, these events will only increase as vaccination rates continue to fall. So will unnecessary deaths among children.
Instead of turning back the clock, our leaders and parents must learn from Washington’s example. Necessity requires that we vaccinate our children.
People visiting the emergency room at Nemours Children’s Hospital in Wilmington on Wednesday might have been exposed to measles, according to the Delaware Division of Public Health.
Officials are working on contact tracing to notify those who could be affected, and to verify their vaccination status, provide educational resources, and recommend quarantine if needed.
A highly contagious illness, measles can infect 90% of exposed unvaccinated people. Delaware residents can check their vaccine status at the DelVAX Public Portal or through their healthcare provider.
The Delaware Division of Public Health recommends a dose of the measles, mumps, and rubella vaccine within 72 hours of exposure. Pharmacies and primary care providers can help access the vaccine.
As an airborne virus, measles can be spread through coughs, sneezes, and saliva particles. Those particles can linger in the air and nearby surfaces for more than two hours, exposing anyone who might have been in the room.
Officials urge people to keep a 21-day watch on their symptoms — which could include high fever, cough, runny nose, and a red rash — until March 11.
Measles can be particularly dangerous for immunocompromised people, such as organ-transplant and chemotherapy patients, people living with HIV/AIDS, and children under 5.
No matter their vaccination status, pregnant people who might have been exposed are encouraged to go to the emergency room as soon as possible for a checkup and possible treatment.
Delaware is not the only state dealing with a measles comeback.
Last week, a possible measles exposure was detected at Philadelphia International Airport. And on Feb. 5, five cases were confirmed in Lancaster County, according to the Pennsylvania Department of Health. All patients were young adults and school-age children, marking the first outbreak of the year.
Meanwhile, South Carolina is currently dealing with a large outbreak that doctors call the worst in 30 years, Reuters reported.
The University of Pennsylvania Health System had an operating profit of $189 million in the first six months of fiscal 2026, up from $117 million in the same period a year ago, the nonprofit reported to bond investors Friday.
Operating income increased, even after Penn put $43 million put into reserves for medical malpractice claims. Two years ago, Penn had recorded charges totaling $90 million for the same purpose.
Here are more details on Penn’s results:
Revenue: Penn had $6.76 billion in total revenue, up nearly 12% even adjusting for the inclusion of Doylestown Health in fiscal 2026. Penn acquired Doylestown last April.
“We’ve had good volume growth over the prior year, particularly in our outpatient activity,” the health system’s chief financial officer, Julia Puchtler, said in an interview.
The system has also had an increase in the acuity level on the inpatient side, she said. That translated into more revenue.
Expenses: The $43 million malpractice charge boosted overall malpractice expenses through December to $125 million, from $69 million in the same period a year ago.
It’s not that Penn is seeing more claims, Puchtler said. “It’s really the average reserve per claim that we’re seeing accelerate,” she said.
Notable: Excluding Doylestown, Penn saw a 5.9% increase in patient volumes, Puchtler said. “That’s mostly outpatient,” she said. “Outpatient surgery, endoscopy, and some of our other infusion therapy are all increased over the prior year.”
Editor’s note: This article has been updated to reflect an additional medical malpractice charge in 2024, bring the total to $90 million.
Sometimes it’s a fall that brings a broken hip and a loss of mobility. Or memory problems that bubble into danger. Or the death of the partner who was relied upon for care.
The need to move to a nursing home, assisted living facility, or another type of care setting often comes suddenly, setting off an abrupt, daunting search. It’s likely something no one ever wanted, but knowing what to look for and what to ask can make a big difference.
Here’s what to do when looking for a long-term care facility:
Start with government ratings
Regulation of assisted living facilities varies greatly from state to state, meaning there’s no centralized standards or source for information. If you’re looking for a nursing home, though, they are monitored by the federal government.
The Centers for Medicare and Medicaid Services maintains records on nursing homes, including data on who owns the facility, how robust its staffing is, and what types of violations it might have been fined for. It assigns homes a star rating, from one to five.
Sam Brooks, director of public policy for the National Consumer Voice for Quality Long-Term Care, says while the star rating “can be notoriously unreliable,” due to its reliance on self-reported data, it can still provide some clues about a home.
“One or two stars, expect it to be bad,” Brooks says.
Ratings can be a resource to rule out the worst options, but not necessarily to find the best. Still, Brooks suggests taking a closer look at four- and five-star facilities and to consider a home’s ownership, too. Nonprofit homes are often better staffed.
You could scour inspection reports and online reviews for clues, too, but eventually you’ll need to make a list of potential candidates and start making visits.
“The data,” Brooks says, “only goes so far.”
Look past the lobby
When visiting a home on your list, be careful not to be too swayed by decorative touches that might be designed to lure you in, like a lobby’s furniture, dangling chandeliers, or vases of flowers.
“When I tour a building, I listen first. Is it loud? Are call bells ringing nonstop?” says Mark Sanchez, CEO of United Hebrew, a nursing home in New Rochelle, N.Y.
After that, Sanchez says, switch your senses. Do you detect an odor? Do you see residents clustered around the nurses’ station, perhaps clamoring for help? Are staffers speaking respectfully to residents? Are they making eye contact? Are they rushed?
“Culture shows up in small moments,” Sanchez says, “and it matters.”
Seeking input from families of current residents can be insightful. Another resource may be your local long-term care ombudsman. Ombudsmen, funded by the federal Older Americans Act and present in every state, investigate long-term care residents’ complaints.
With all the available information on each home, it can be easy to feel like you’re drowning in data. So pay attention to how a place feels, too, and pair that with concrete facts.
When Jennifer Fink was making the “stressful, grief-inducing, hard, and scary” decision on what memory care community was right for her mother, she didn’t consult state databases or Google ratings. She went with her gut reaction and luckily, it was right.
“Trust your gut. Keep top of mind that the salesperson wants your loved one’s money,” says Fink, of Auburn, Calif. “If it’s giving you the ‘ick,’ then move on.”
Staffing matters most
More than any other single thing, experts on long-term care stress that a facility’s staffing is most important. That means both the quality of the care you witness workers giving residents during your visit and the average staffing levels shown in the reported data.
A home providing an average of three hours of nursing care to each resident each day may not look all that different on paper from one providing three-and-a-half hours. But those minutes matter dearly, meaning the difference between a person getting a shower, having help at mealtime, or being discovered if they’ve fallen.
During a visit, pay attention to how quickly call bells are answered and whether it seems like residents are engaged in activities. Ask staff how long they’ve worked there. A home that holds on to its workers for years may offer your loved one more continuity.
Evan Farr, an elder law attorney in Lorton, Va., who wrote The Nursing Home Survival Guide, says visiting a facility at night or on the weekend can be particularly revealing.
“These are the times when staffing is reduced and the true operation of the facility becomes apparent,” Farr says. “It is entirely possible to have a five-star rated facility that is woefully understaffed from 5 p.m. Friday until 8 a.m. Monday morning.”
Keep a long-range view
When faced with an urgent decision, it can be difficult to focus on anything beyond the factors in front of you. But it’s important to choose a home with a long-range view.
At the start, many long-term care residents are able to pay for the cost of their bill. But what happens if their money runs out? If it’s a nursing home that accepts Medicaid, how many beds are allocated to such residents? Would your loved one get that slot? If it’s an assisted living facility, do they even accept people on Medicaid?
Assisted living facilities often have complicated billing structures that require a bevy of questions to understand. Ask how costs may change as a person’s needs increase. Some places tack on separate charges for tasks like helping a person to the bathroom.
“Four-thousand dollars a month can become $8,000 overnight,” says Geoff Hoatson, founder of the elder law practice Family First Firm in Winter Park, Florida.
Another fact of long-term care that few understand is how often facilities seek to remove residents seen as undesirable, often due to a change in their financial circumstances or in their health. Dementia patients in particular — with challenging care needs and symptoms that can sometimes bring aggression — are targeted with orders to leave.
“Ask specifically what conditions would require transfer,” Hoatson says.
In the wake of the U.S. Bicentennial, in which Philadelphia was at the center of a yearlong celebration of the country’s 200th birthday, one of the city’s contributions to public health was put on the chopping block.
On Feb. 15, 1977, city officials confirmed that Mayor Frank Rizzo was closing Philadelphia General Hospital.
The poorhouse
Philadelphia General Hospital traced its lineage back to 1729, predating even therevered Pennsylvania Hospital, which was founded in 1751 andis generally considered the nation’s first chartered hospital.
Philadelphia General Hospital was originally established at 10th and Spruce Streetsas an almshouse, also known as an English poorhouse.
“The institution reflected the idea that communities assume some responsibility for those unable to do so themselves,” Jean Whelan, former president of the American Association for the History of Nursing, wrotein 2014.
The almshouse was used as housing for the poor and elderly, as well as a workhouse. It also provided some psychiatric and medical care.
It moved in the mid-1800s into what was then Blockley Township, atwhat is now 34th Street and Civic Center Boulevard, and began offering more traditional medical services. The Blockley Almshouse’s barrage of patients and their variety of maladies helped it naturally grow into a teaching tool for nursing and medical students.
And by turn of the 20th century, it had become a full-blown medical center, made official by its new name: Philadelphia General Hospital.
But it held onto its spirit.
Its doors were open to anyone who needed care, no matter that person’s race, ethnicity, class, or income.
Healthcare was a given. Workers saw it as a responsibility.
Even if it wasn’t always the best care.
Poor health
The hospital relied on tax dollars, and as a result was often short on staffing and low on supplies. It was a source of political corruption, scandal,and discord among its melting pot of patients.
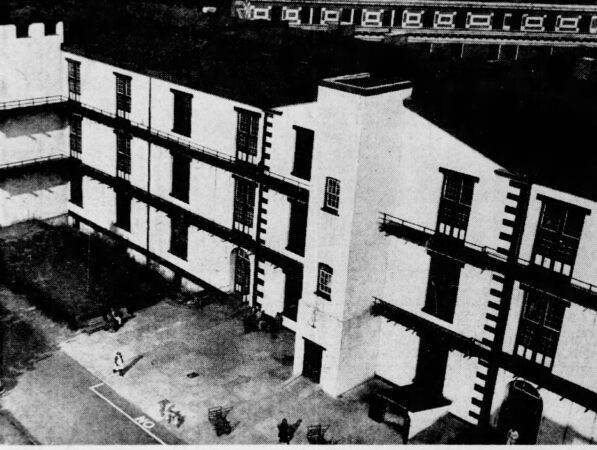
Patients in the hallways of Philadelphia General Hospital in the 1940s.
Eventually, it collapsed under the weight of its mission.
Its facilities became outdated, its services could not keep up, and its role as educator was outsourced to colleges and universities.
Philadelphia General Hospital’s closure left a gaping hole in available services in West Philadelphia. It was no longer there to help support the uninsured.
Before it officially closed in June 1977, it was considered the oldest tax-supported municipal hospital in the United States.
“There’s a common misunderstanding that PGH recently has become a poor people’s hospital,” said Lewis Polk, acting city health commissioner, in 1977. “It’s always been a poor people’s hospital. The wealthy never chose to go there.”
Its old grounds are now occupied by several top-rated facilities, including Children’s Hospital of Philadelphia and the University of Pennsylvania medical campus.
A historical marker there notes Philadelphia General Hospital’s nearly 250 years of service to the community.
STRAITS OF FLORIDA — At 2 a.m., oceanographer Ryan Smith was headed into his 12th hour of work with little sleep when trouble started.
From the rear deck of the University of Miami’s research boat, he guided the vessel’s winch to lower a cage containing 14 long, gray tubes, collectively weighing about 1,000 pounds, hundreds of meters deep into the Atlantic Ocean, to record the temperature, salinity and density of the water. But after running smoothly for the first two-thirds of the trip, the sensors now suddenly stopped transmitting data.
There was no time for a hiccup. With urgency mounting, Smith signaled to bring the cage to the surface.
At sea, there is no helpline to call for a broken instrument at this hour (or any hour). If the team couldn’t fix it, they would need to make a 12-hour slog back to Miami through the fast-moving Florida Current — the precise subject they were trying to measure.
For 43 years, scientists have been studying the strength of the water flow between Florida and the Bahamas to learn what drives its changes over time. The information could help scientists answer a pressing question: Is the Florida Current, one of the world’s fastest ocean currents, slowing down? If so, it could indicate weakening of the larger circulation system in the Atlantic Ocean — what scientists call the Atlantic Meridional Overturning Circulation (AMOC) — which could be disastrous.
Even Hollywood has imagined the harm that could result from a collapse of this system of currents, which acts like a conveyor belt as it transports water, nutrients, and heat through the Atlantic.
While scientists doubt the scenario sketched out in the 2004 movie The Day After Tomorrow, in which the AMOC’s failure prompts a calamitous ice age across the Northern Hemisphere, researchers say rain patterns could change or fail in Southeast Asia and parts of Africa, disease may spread to new populations, and temperatures would probably drop across Western Europe. Iceland has even declared that the risk of such a collapse is a national security threat.
But climate scientists are at odds over how soon, or whether, the circulation system may weaken. Researchers largely agree that the AMOC may weaken over this century as the world warms, but they differ on whether the system is already slowing down.
Direct observations of the AMOC’s and the Florida Current’s flow, velocity, temperature and salinity could help clarify this. The Florida Current, which helps shuttle water north, is a key component in calculating the system’s strength.
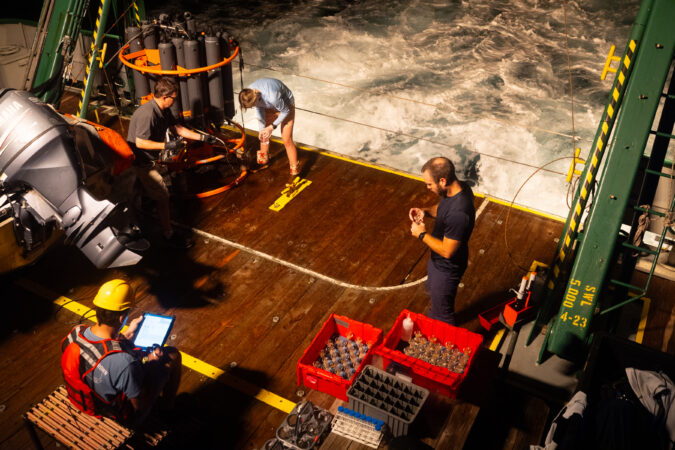
Traveling between Miami and the Bahamas, a crew from the University of Miami and the National Oceanic and Atmospheric Administration homed in on the Florida Current, the world’s longest nearly continuously observed ocean current. Over 36 sleep-deprived hours, six researchers and seven crew members traversed the ocean, dove underwater, and collected gigabytes of measurements. These expeditions gather data that generations of scientists can use to better understand the state of our oceans — and humanity’s future.
Tyler Christian, a marine scientist, takes a photo of a waterspout during a research trip to collect data on the Florida Current.
The AMOC debate
For more than four decades, scientists have almost continuously measured water flow across the Florida Current, largely with the help of a decommissioned AT&T telecommunications cable running from West Palm Beach to Grand Bahama Island.
The telephone line wasn’t intended for ocean research, but NOAA scientists noted that it picked up tiny voltages induced by seawater flowing across the Florida Straits, which changed depending on the current’s flow.Using direct measurements of the waterway from research cruises, scientists can convert the voltages into the volume of water carried each second through the strait.
In 2005, British oceanographer Harry Bryden tapped these cable measurements and the limited available ship measurements in a seminal paper that suggested a possible slowdown in the AMOC between 1957 and 2004. Using data across the Atlantic Basin today, scientists have found that the AMOC varies, daily and seasonally, yet it also appears to have experienced a slight weakening over the past two decades.
But is it on a long-term decline because of human-induced planetary warming? Debatable.
At about 4 a.m., oceanographer Denis Volkov, right, checks in on Jay Hooper, who helps the team with data management
The Florida Current is one of the main forces that make up the western boundary of the AMOC. The warm Florida waters feed into the mighty Gulf Stream, which merges with the warm North Atlantic Current headed toward Europe. As the current reaches the Arctic, air temperatures cool the water, which becomes denser. The water sinks and moves south toward the equator, where it is again warmed by the sun and returns north.
“The role of the AMOC in the climate is it carries a huge amount of heat from the equator towards the poles,” said Denis Volkov, who is a co-principal investigator of NOAA’s Western Boundary Time Series project along with Smith.
But scientists say a warming world is throwing off this balance. As Arctic ice melts, freshwater enters the North Atlantic — making the ocean water less dense, so it is less likely to sink. As a result, scientists propose thatit cannot power the ocean conveyor belt as well, so less salty, warm water is getting transported northward.
A major shift in the Atlantic Ocean’s circulation could create severe drought in some areas and damaging floods in others. Sea level could rise by a foot or more along the U.S. East Coast if it collapsed.
Scientists have typically used data that indirectly hints at the current’s movement — such as sea surface or air temperature — to reconstruct the oceans in models and track whether the overall system is weakening, but they have reached mixed conclusions.
For instance, a 2018 study plugged sea surface temperatures into computer models to show that the AMOC is weakening. Then, a paper released last January reported no evidence of weakening over the past 60 years after examining data on heat exchanges between the air and the ocean called air-sea fluxes.
The dive boat takes scientists to a site to collect data on the Florida Current.
Volkov and his colleagues are helping approach the puzzle with observations. In 2024, they reassessed the cable data from the Florida Current, adjustingfor changes from Earth’s geomagnetic field. First, they found that the current had remained stable over the past four decades. Then, they updated calculations of the AMOC in this region, which has been monitored for only 20 years or so, with the corrected data and found that the AMOC wasn’t weakening as much as previously calculated at this latitude.
“But there is a caveat that observational data is very short,” said Volkov. He said scientists would need another 20 years of AMOC observations to determine if the small decline is a robust feature and not part of natural variability.
And the AMOC can still weaken even if the Florida Current remains strong, he said, since it is the sum of currents across the basin. But long-term changes in the Florida Current can serve as an indicator of trouble for the rest of the system.
One snag, said Volkov: The serendipitous cable that provided data for more than 40 years malfunctioned in 2023 — perhaps broke. Until it’s fixed, researchers are ramping up their diving operations to recover data from underwater acoustic barometers on the ocean floor.
Volkov, left, and Smith watch as a sampling instrument drops into the water.
The expedition
When the research vessel departed from the university’s dock around 4 a.m. on Sept. 3, the sun and most of the science staff were down for the night. A few shipmates gazed at the illuminated cityscapes from the stern deck, next to the diesel engine’s deep rumble. After traversing rocking waves, the crew reached scenic Bahamian waters eight hours later.
The green F.G. Walton Smith, 96 feet long, and its crewmake this overnight trip about six times a year, traveling 93 nautical miles diagonally from Miami toward the Little Bahama Bank. From there, they go west and collect data at nine sites from the boat and dive underwater at two others.
The team’s goal is to determine the amount of water flowing north through the Florida Current per second through a series of underwater instruments, from the boat and from satellites. They also collect temperature, salinity, density and velocity data; velocity and temperature, for example, can be combined to calculate the amount of heat transported across an area.
Chomiak, left, and Zach Barton, a technician and engineer, return from diving to the seafloor to place a data-collection instrument.
At the first dive site, a remora — a long, torpedo-shaped suckerfish — circled the two scuba divers less than a mile from the boat. The slender fish is known for a unique fin on its head that suctions itself to sharks, whales, and turtles to feed off their detritus. And for a quick moment, it latched onto Leah Chomiak’s head. And her thigh.
Chomiak focused on the barometer in front of her. Her bulky gloves made it harder to use a screwdriver 50 feet below the Bahamian surface. She and her fellow diver held onto the long tubes that had been recording data every five minutes for the previous two months, since the last time divers brought the instruments to the surface and downloaded the data.
“Now we decided to service them more frequently, because, at the moment, this is the only source of data for our Florida Current transport estimates,” Volkov said. The scientists can use the pressure data to help calculate the amount of water flowing through the area.
Next, the ship arrived at the first of nine hydrographic stations andlowered a cage of sensors known as a CTD-rosette sampler (CTD stands for conductivity, temperature and depth, although it measures many more properties). Researchers can use the temperature and salt concentrations of a particular mass of water to infer where it came from and how it reaches other parts of the world.
Christian takes a quick nap in the galley as the vessel travels back to Miami.
Jay Hooper, who has been on these trips for 10 years and helps with data management, sat at the ship’scomputer station.
“Ready whenever you are,” he said into his headset.
From the top deck, the captain lowered the rosette into the water, dropping 60 meters each minute. As the instruments approached the bottom at 486 meters, Hooper said to slow down.
Lines of various colors — representing salinity, temperature, and density — squiggled down on Hooper’s computer screen as the sensors dropped. Temperature decreased and density increased as the instruments descended. Seventeen minutes later, the rosette was brought back onto the boat.
After hours of gathering data, Hooper and Smith hit a snag at the seventh station. The rosette now wasn’t sending any information to the computer. Was it human error? Did the instrument break?
The two tried different solutions as the other scientists slept. Then they replaced the sensors’ cable, andas they lowered the rosette, data filled the computer screen.
The boat stopped for the last dive near the Florida coast to retrieve the second set of underwater acoustic barometers. But the water was so cloudy, thick and green that the divers couldn’t see their hands, so they decided they would try on the next trip.
Captain John Cramer pilots the vessel back to the university.
For the next 12 hours, the boat fought against the Florida Current to take the crew home. Some aboard mustered up energy to sing “Happy Birthday” to one of the crew members.
The next morning, Smith and his colleagues processed the data to upload to NOAA’s Atlantic Oceanographic & Meteorological Laboratory website. There were no notes about a cable malfunction, encounters with remoras or sleep deprivation.
The Excel spreadsheet had a single note for each station it recorded: “Profile looks good; use these data.”
About 300,000 Pennsylvania residents risk losing Medicaid next year when new eligibility rules take effect, and advocates worry that too few people are aware.
More than 100 public health workers, community advocates, and medical providers gathered Thursday to strategize how to spread the word about forthcoming changes to Medicaid.
The nonprofit Community Behavioral Health organized the eventat its Center City offices as a first step toward rallying the stakeholders tasked with helping people navigate the new rules in order to maintain access to critical health services. The city contracts with CBH to provide mental and behavioral health services for Philadelphians with Medicaid.
New federal rules taking effect in January 2027 require certain adults to meet work requirements and reapply for Medicaid every six months, instead of the current once a year. The changes were ordered under Republicans’ 2025 spending bill and signed into law by President Donald Trump. They are part of the largest cut in recent history to Medicaid, the publicly funded health coverage program for low-income families and individuals, and people with disabilities.
States will be expected to verify eligibility for millions of people twice as often, a major administrative burden. For now, who will be exempt remains unclear. For instance, the law suggests that “medically frail” individuals will not need to meet work requirements or reapply every six months, without detailing who would qualify.
The federal government expects to release more details in June.
Public health leaders say they cannot wait for the additional guidance to begin talking about the forthcoming changes, in order to minimize the number of people who lose coverage.
“It needs to be consistent and ongoing,” Donna E.M. Bailey, CEO of CBH, said of the group’s outreach efforts. “It really is a Philadelphia responsibility.”
The coming Medicaid changes
Roughly three million Pennsylvania residents are covered by Medicaid. About a quarter of them — roughly 750,000 people, including 180,000 in Philadelphia — qualify because the 2010 Affordable Care Act expanded access to low-income parents and childless adults. This so-called expansion group saw the bulk of the Medicaid cuts in last year’s Republican spending bill.
Beginning next year, most people in this group will need to provide monthly proof that they spent at least 80 hours working, volunteering, or participating in job training. Every six months, they will need to reapply for the program. Some experts have compared this process to filing taxes because of the extensive paperwork and documentation required.
Pennsylvania has estimated that about 300,000 people will lose Medicaid because they cannot navigate the new requirements — even though many remain eligible.
“It’s hard to imagine with all these changes that it’s just going to be smooth,” said Mike Nardone, a former director of Pennsylvania’s Medicaid program, who spoke during the CBH event. “We’re going to have people who lose coverage, and we’re going to have to understand why that happens.”
Early and frequent communication is the best strategy for minimizing the number of people who lose Medicaid, public health advocates said at Thursday’s event.
“We need to start now. This isn’t something that can wait,” said Joan Erney, CBH’s former chief executive.
The dozens of medical providers, social workers, and community advocates in attendance were urged to work together to develop strategies for helping people to understand what new steps to take to keep their Medicaid coverage.
“We always need the voice of those of you on the ground,” said Leesa Allen, a former Pennsylvania Medicaid director, who spoke during the panel.
The event was the first in a series planned by CBH, which will expand outreach with similar events throughout Philadelphia designed for families and individuals to ask questions and learn more about the new Medicaid rules.
Jennifer Udler has been a practicing therapist for 25 years. A little over a decade ago, she started training for a marathon, running with a group near her home in Montgomery County, Maryland.
“I noticed that people were more comfortable, less inhibited, opening up and talking during our group training runs,” Udler said. “And I started to wonder if there was a way to do a practice where people are moving.”
Udler sees children and adolescents as well as adults, and she suspected that her younger clients especially might feel more comfortable talking while walking on a nature trail rather than sitting in a therapist’s office. She decided to try it with one of her young clients with his mom’s permission.
“We met at a park, and we walked around, and he was a different kid,” Udler said. “He was running around, and he was showing me stuff in nature. And he talked.” She said they made more progress in one session outside than they had in two years meeting in her office.
“That was in the snow in February,” she added. “So I was like, it’s only going to get better.”
Udler started reading more about outdoor therapy, which is also known as walk-and-talk or nature-informed therapy. At that time she couldn’t find any formal training or certification programs, but she did learn that other therapists had tried it and found many of the same benefits she had.
“You’ve got the movement, you’ve got nature, which is extremely grounding and stabilizing for people, and you have the co-regulation, walking side-by-side,” Udler said. For her younger clients or anyone uncomfortable with therapy, it also helped to be walking while talking about difficult topics because they didn’t always have to make eye contact with her.
She wrote her own informed consent for her clients, establishing the additional risks of outdoor therapy and how confidentiality would work in a public park. She started a practice called Positive Strides, specializing in walk-and-talk therapy sessions outdoors in nature.
“As I did the work and saw different types of people with different kinds of mental health issues, I realized how amazing it is,” Udler said.
Trading the couch for the great outdoors
In March of 2020, when many therapists moved their practices online, a smaller number brought their practices outside. The benefits were not felt only by the clients. Nature acts as a sort of “buffer against burnout,” said Heidi Schreiber-Pan, the executive director and founder of the Center for Nature Informed Therapy, where she trains clinicians in how to bring their practices outdoors.
“What we’re hearing from people is that they can see more clients when they have outdoor sessions or nature-informed sessions,” Schreiber-Pan said.
The American Psychological Association put out new guidelines this past fall for how clinicians can implement walk-and-talk therapy into their practice.
The number of therapists working outside is still small. Shreiber-Pan believes that’s in part because therapists don’t realize that nature is all around us. One of the first questions she asks in her trainings is: When you think of nature, what comes to mind?
“They talk about, like, these beautiful national parks or the mountains or the ocean,” Shreiber-Pan said. “And where is your therapy office? Not there.” She said that part of the training is helping practitioners recognize that nature is all around us — even in a city park.
Miki Moskowitz is a clinical psychologist who practices in a primary care setting, which means she sometimes sees a patient only a couple of times.
“We’re trying to make a difference, even in one single session,” she said.
For Moskowitz, practicing outside has improved her own mental health and increased her capacity, but she also sees the immediate impact for her patients.
“What I’ve seen that’s so encouraging is that sometimes just that first session we go for the walk, and patients are, like: ‘Wow, I didn’t know this trail was here. This is so beautiful. This feels so great. This is totally something I can do on my own,’” Moskowitz said. “That is so much more powerful than if we’re sitting in my office, which has no windows, just talking about the idea of going outside.”
The brain benefits of getting outside — even when it’s freezing
When Marc Berman was doing research at the University of Michigan, he helped devise a study to look at the brain benefits of time in nature. Participants did a challenging task testing their memory and attention, and then they were sent on a walk either through downtown Ann Arbor or in the area arboretum. Those who walked in nature showed a 20% improvement in their short-term memory, while those who walked in an urban environment did not.
Berman and his colleagues did this experiment in June and January. In the winter, the nature walk was less enjoyable — but just as beneficial.
“That was pretty cool because it suggested that you didn’t have to enjoy the nature walk to get these cognitive benefits. There was something deeper going on,” Berman said.
One explanation for why nature is so good for our brains is called the attention restoration theory. The idea is that our ability to pay attention is finite, and spending time in nature can replenish our capacity. Nature is also “softly fascinating” — it captures our attention without overwhelming our senses.
“I can kind of mind-wander and think about other things when I’m looking at a waterfall,” Berman said. “I can’t really mind-wander or think about other things when I’m in Times Square.”
Berman is now a psychology professor at the University of Chicago and author of the new book Nature and the Mind: The Science of How Nature Improves Cognitive, Physical, and Social Well-Being.
How to make the most of time outdoors
Whether or not you are in therapy, your brain can benefit from a dose of nature, especially during the colder months when many of us are inclined to stay indoors. Here are some science-backed tips for how to get the benefits.
Nature can be found anywhere. You just have to look for it. Research has shown that noticing nature and paying attention to it can have positive effects even in an urban environment. Psychologists recommend noting the bird song you hear on the walk to your car, looking at the leaves on the trees and the clouds in the sky, and just taking a moment to appreciate nature’s beauty — even if it’s just a small plant poking through the sidewalk.
You don’t have to like it.Nature can be an acquired taste, especially when it’s cold. But you don’t have to be a backpacker or love camping to benefit from time outside. Berman and others have found in their research that we get the brain benefits whether or not we enjoy a walk in the woods.
Try a mindfulness exercise. Many people struggle to sit still and meditate, despite its benefits — but Moskowitz said that mindfulness practices can come more easily outside. “Just look up at the treetops and notice what you see, notice what you hear,” Moskowitz said. “Look for something that’s moving, and watch the branches sway in the breeze. Look at something close up, or look at something far away. You’re doing a mindfulness practice, and you’re tuning into your senses, and you are focusing your attention, but it’s not hard work.”
Bring nature inside.If you aren’t able to get outside as often as you would like, you can still get some of the benefits. Put a plant in your office — even a fake one — or look at pictures of beautiful landscapes. Listen to bird songs at your desk. “It’s not as strong as the real thing, but you can get benefits from the simulated nature,” Berman said.
Embrace the winter.When it’s cold and snowy outside, our impulse is to stay inside. But less time outside can contribute to seasonal depression. Schreiber-Pan recommends following the Scandinavian practices of “friluftsliv” — or “open-air living,” getting outside no matter the weather — and hygge, or embracing the cozy indoors when you come back in. “The happiest people on this planet are the Scandinavians,” Schreiber-Pan said. “They also have the longest winters.”
At least 1,100 dead or sick birds, mostly Canada geese, have been reported across New Jersey in an outbreak that started on Valentine’s Day, according to state officials.
At least 50 geese have died at Alcyon Lake in Pitman, Gloucester County. Officials have closed the lake and the adjoining Betty Park out of precaution.
The fish and wildlife division within the New Jersey Department of Environmental Protection (DEP) and the U.S. Department of Agriculture are tracking them as suspected cases of highly pathogenic avian influenza (H5N1), or bird flu.
Bird flu is not new. But it began to spread in the U.S. in January 2022 and has infected wild and domestic birds in every state.
While bird flu can infect humans, the U.S. Centers for Disease Control and Prevention has said it is primarily a threat to animals and poses little risk to the public.
State officials say large numbers of dead geesemay be concentrated in areas where birds gather to look for open water as ice melts. They said that the 1,100 dead or sick wild birds were reported between Saturday and Monday.
Where have dead geese been found?
The DEP says it has received reports of dead Canada geese in South Jersey, including in Hainesport, Burlington County; Sicklerville, Camden County; and Pitman.
Annmarie Ruiz, Gloucester County’s health officer, said the dead geese were noticed in Pitman on Tuesday. She said that there were probably more than 50 at Alcyon Lake, but that there were reportsof dead geese elsewhere in the municipality.
“Right now, we have to presume that it is bird flu based on the signs the birds were exhibiting,” Ruiz said.
The New Jersey Department of Agriculture took some of the birds for testing. The results could take weeks, she said.
“Right now, we’re just erring on the side of caution,” Ruiz said.
Ruiz said workers use face shields and gloves when handling the birds, which are triple-bagged before being disposed.
She said people can report sick or dead wild birds to Gloucester County animal control at 856-881-2828 or the DEP at 877-927-6337.
A lifeless bird lays on the ice at Alcyon Lake in Pitman, N.J. on Wednesday, Feb. 18, 2026. Two adjacent parks, Betty Park (in background) and Alcyon Park (not in photo) are closed as a result of the mysterious birds deaths.
Caryelle Lasher, Camden County’s health officer, said there have been only a small number of reports of dead birds in the county.
Those were concentrated in the lake off Mullen Drive in the Sicklerville section of Gloucester Township, she said.
Overall, however, the county has not seen a spike in reports, she said.
Ruizand Lasher — as well as state officials — stress that people should not touch sick or dead wildlife of any kind. And they should keep pets away.
Even though the risk is low, the potential for human infection exists.
H5N1 is a respiratory bird disease caused by influenza A viruses. Wild birds, such as ducks, gulls, and shorebirds, can carry and spread these viruses but may show no signs of illness, according to the DEP.
The disease can kill domestic poultry such as chickens. Typical symptoms include diarrhea, nasal discharge, coughing, sneezing, and incoordination.
It continues to infect not only birds, but also mammals.
Tips to prevent infection:
Do not touch sick or dying animals, or bring them into your home.
Keep pets away from them, as well as away from droppings.
Wash hands frequently if you are near wildlife.
Do not eat undercooked eggs, poultry, or beef.
Prevent cross-contamination between cooked and raw food.