It’s official. Medicare costs will eat up much of older Americans’ Social Security cost-of-living increase next year.
The standard monthly premium for Medicare Part B, which covers outpatient care, doctors’ services, durable medical equipment and preventive service, will be $202.90 in 2026, the Centers for Medicare and Medicaid Services said on Nov. 14. That’s up $17.90, or nearly 9.7%, from $185.00 in 2025.
It’s smaller than the $21.50 increase the Medicare Trustees had forecast earlier but still the second largest dollar jump in program history behind 2022’s $21.60 gain and almost 3.5 times the 2.8% Social Security raise for next year. That means seniors will probably see a drop, again, in their standard of living, experts said.
Seniors were the only ones who saw an increase in poverty in 2024. All other age groups saw a decrease or stayed the same.
“The public is likely to perceive this Part B increase as taking a significant chunk of or even most of their COLA,” said Mary Johnson, independent Social Security and Medicare policy analyst. “In other words, another continuation in relentless cost increases battering consumer finances.”
Monthly Social Security checks will rise $56, on average, starting in January because of the 2.8% COLA, the Social Security Administration said. After the $17.90 increase in Medicare Part B, the average monthly COLA increase is cut to $38.10.
Hold-harmless provision
Such a large increase in Medicare Part B will likely trigger the hold-harmless provision for Social Security recipients with a Social Security benefit of $640 or less, Johnson said.
The Medicare hold-harmless provision prevents the Part B premium increase from being larger than the Social Security COLA. If a premium increase is higher than the COLA, the rule prevents the beneficiary from paying the full increase. The portion of the increase those beneficiaries don’t pay is spread out among others who aren’t protected by the rule.
For those people with a Social Security benefit of $640 or less, the 2.8% COLA next year would mean just less than an $18 per month increase in their Social Security checks. Without the hold-harmless rule, the Part B premium increase would swallow the entire COLA.
In 2022, only about 1.5% of Medicare beneficiaries had their Part B premiums limited by the hold-harmless provision, government data showed. Part B rose $21.60 to $170.10 in 2022 while the average monthly COLA increase boosted Social Security checks by $92.
In 2017, when Medicare premiums jumped 10%, or $12.20, to $134.00 and far outpaced the 0.3%, or $5 average, monthly COLA increase, 70% of Medicare Part B enrollees paid a lower-than-standard Part B premium due to the hold-harmless provision.
Hold-harmless rule isn’t panacea for all costs
The hold-harmless provision can protect seniors from Part B premium surges, but other costs may bite, Johnson said.
“If individuals have other automatic deductions such as for Medicare Advantage or Part D premiums, increases in those premiums could reduce Social Security benefits,” Johnson said. The optional Part D covers prescription drugs.
Some Part D plans are increasing premiums by as much as $50 in 2026, the maximum allowed under a Part D Premium Stabilization Demonstration Program, according to the nonprofit, nonpartisan research organization KFF.
“To complicate things, there are fewer stand-alone Part D plans to choose from,” Johnson said. The total number of prescription drug plans has dropped by half since 2024, KFF said.
Is everyone eligible for hold harmless?
Those who aren’t eligible for the hold-harmless provision include:
New Medicare enrollees
People who aren’t receiving Social Security benefits
High-income earners
What about deductibles?
In addition to higher premiums, higher annual deductibles next year will make health insurance even more expensive for Medicare enrollees.
The annual deductible for all Medicare Part B beneficiaries before insurance covers costs will be $283 in 2026, up $26 from $257 in 2025, CMS said.
Could it have been worse?
The Part B premium could have been higher, CMS said.
“If the Trump Administration had not taken action to address unprecedented spending on skin substitutes, the Part B premium increase would have been about $11 more a month,” CMS said. “However, due to changes finalized in the 2026 Physician Fee Schedule Final Rule, spending on skin substitutes is expected to drop by 90% without affecting patient care.”
Skin substitutes are materials like biologic, synthetic or biosynthetic products that mimic human skin and are used to cover and treat chronic wounds, such as diabetic foot ulcers. The Trump administration reclassified these bandages so they aren’t billed separately. CMS estimates the change would reduce Medicare spending on these products by nearly 90% in calendar year 2026.
Medicare Trustees also estimated earlier this year the standard monthly Part B premium would rise $21.50 to $206.50 in 2026 from $185 in 2025. That would have been more than the $17.90 increase to $202.90 in 2026.
For more than three decades, Marion Nestle has been telling people what to eat.
In the late 1980s, she edited the first Surgeon General’s Report on Nutrition and Health, then went on to cowrite the federal government’s Dietary Guidelines for Americans and cofound New York University’s influential food studies program.
Nestle, now an emerita professor at NYU, says her time in government opened her eyes to the multi-billion-dollar food industry’s enormous influence over Congress. By the early 2000s, she became a critic of the food industry and an advocate for major food reforms, which she made the case for in best-selling books.
In 2002, Nestle published Food Politics, an exposé that argued that the food industry is at the root of many of the country’s nutritional problems. The industry rakes in ever-growing profits by churning out highly processed foods laden with additives, Nestle wrote, and then aggressively markets those foods to children and adults while lobbying against regulations and trying to co-opt nutrition experts.
Over the years, Nestle’s blunt nutrition advice, sharp criticism of food companies, and frequent media appearances made her one of the most recognizable names in nutrition. In 2006, she published one of her most popular books, What to Eat, which showed consumers how to navigate supermarkets and improve their health by deciphering food labels.
At age 89, Nestle, who lives in New York City and Ithaca, is still going strong. In November, she published her latest book: What to Eat Now: The Indispensable Guide to Good Food, How to Find It, and Why It Matters.
We wanted to know how Nestle’s knowledge of nutrition and the food industry affects her daily food decisions. So we caught up with her to find out what she eats in a typical day, which foods she loves and avoids, which “junk foods” she can’t resist, and whether she takes supplements or has advice on how to navigate grocery stores. This interview has been edited for length and clarity.
Q: What’s your general approach to food?
A: I follow Michael Pollan’s famous mantra: Eat food, not too much, mostly plants. And I define food as being unprocessed or as minimally processed as possible. Not ultra-processed. I really think that takes care of it. That doesn’t mean I’m perfect. I’m an omnivore. I eat everything. I just don’t eat very much in part because metabolism drops with age, and I don’t have much metabolism left.
I eat pretty healthy, but I don’t obsess about it. If I have a bad day of eating, I don’t worry about it. By this time, it’s pretty clear I’m not going to die prematurely. Obviously, what I’m eating is working for me because I’m 89 and I’m still here.
Q: What do you eat for breakfast?
A: I start with coffee between 8 and 9 a.m. I’ll have a couple cups of weak coffee with milk, no sugar. And then I’m at work. That’s when I do my writing. I don’t get hungry until about 10:30 or 11 a.m. That’s when I’ll usually have oatmeal or unsweetened Post Shredded Wheat cereal. It basically has one ingredient: wheat. I like the texture of Shredded Wheat and the way that it tastes. I add a little brown sugar, not much. I use a lot less sugar than what’s in presweetened cereals. And then I’ll add blueberries or whatever fruit is in season. That combination to me is really appealing.
I’ve never believed any of the research on breakfast being the most important meal of the day. Most of that was sponsored by cereal companies.
Q: What about lunch?
A: My lunches are totally irregular. Sometimes I’ll have a salad for lunch. Or if I’m having lunch with someone then I’ll eat whatever is in the restaurant. If I’m at home in New York City, I’ll harvest whatever is growing on my terrace. The peaches, cherries, raspberries, and blueberries that I was growing are long gone. But I’ve still got some lettuce and tomatoes, so I’m going to go out and pick those. I might cut up some cheese or have it with peanuts. And I might have some bread with that.
Q: What about dinner?
A: It depends. I just don’t eat that much. But I do really like salads. I can have salads twice a day. If I’m at home, I might have an egg. I might have crackers and cheese with that. I kind of like making meals based on what I have available. So, it depends on what I bought, what’s in the house, or what’s on the terrace. That’s my favorite way of cooking. We have a garden in Ithaca, there’s a garden on my terrace, and there’s a farmers market not very far from here.
I also go to a lot of neighborhood restaurants. I’m going to Mark Bittman’s restaurant this week — the kitchen that he started in the East Village where people pay according to their income. I’ll eat whatever they’re serving. One restaurant that I like a lot is il Buco Alimentari & Vineria. I love going there. They have a particular salad that I adore. It’s always so crisp, and they have wonderful pasta dishes.
Q: What are some foods that you love?
A: Fortunately, I like a lot of very simple foods. I like vegetables. I like eggs. I like cheese. I do eat some ultra-processed foods. But not a lot of them. I don’t like ultra-processed foods that have a long list of ingredients. Most of those don’t taste good to me. I do really like vegetables. I like the crunch, the flavors, and the colors. That makes it easy to eat healthy.
But I recognize that I’m privileged. I weigh basically what I weighed when I was in high school. I don’t have a weight problem. And I have an enormous amount of sympathy for people who do. I consider myself extremely fortunate. Is it genetics? I have no idea. My father died of a heart attack at the age of 47. He was an obese three-pack-a-day smoker. It’s hard to know where genetics fits into this.
Q: Do you have any favorite treats or desserts?
A: Ice cream. When I’m at home in New York City, I try to find ginger ice cream, which I like very much. It’s hard to find. But when I find it, I buy it. And then my partner and I make homemade vanilla ice cream in Ithaca. It’s only three or four ingredients. It’s ruined other ice creams for me because a lot of commercial ice creams have all these emulsifiers in them that keep the ice cream sticking together. Real ice cream completely falls apart if it’s left at room temperature and not eaten right away. It separates and liquefies. But I like that. I think it tastes better and has a better texture than the commercial ice creams that have emulsifiers. I like ice cream without the emulsifiers.
Q: What about snacks?
A: I like corn chips. Not too salty. Some corn chips are ultra-processed, although most are not. The ones I like are Wegmans. They only have a few ingredients — just corn, oil, and salt basically. I also like candy, particularly See’s Candies. The one See’s candy store in New York is just a couple blocks away from me. I normally get the peanut brittle. Sometimes the lollipops. I can have these things in the house and not feel like I have to eat all of them all at once. Not everyone can do that.
Q: Can you tell us about your new book?
A: It’s called What to Eat Now. It’s the updated edition of What to Eat, which was published 20 years ago. It’s a completely rewritten book. I thought it was going to be a six-month project, and it ended up taking me four years because so much has changed in grocery stores. There’s been a huge turnover in products. For example, “functional waters” that contain vitamins, minerals, cannabis, supplements, and other things have replaced Coca-Cola and plain water. Plant milks are new. The only plant milk that existed 20 years ago was soy milk. Now there are tons of others. Plant-based meats did not exist 20 years ago — at least not in the way that they do now.
Q: What is one takeaway from the book?
A: It’s not a book about personal diets. It’s a book about how to think about food issues. I think what to eat now boils down to eat food, not too much, mostly plants.
Q: Do you take any supplements?
A: I don’t take supplements because I eat a healthy diet. I don’t think I need them. But two out of three Americans take supplements. They make people feel better — and it’s hard to argue with that. Life is tough. If all it takes is a supplement to make you feel better, then I’m not going to argue with that. I used to be much more upset about supplements. But now it’s clear to me that they make people feel better. Whether that’s because they’re doing something or because they’re a placebo, it’s hard to know.
But I don’t trust what’s in them. There’s so much evidence that what the label says isn’t what’s actually in them. Many studies have found that a remarkable percentage of supplements do not actually contain what’s listed on their labels. I don’t want to put something in my body if I don’t know what’s in it. And there are things in supplements that are not supposed to be there — that’s what so many studies have found. It’s not true of all supplements. But it’s very hard to know which ones are OK and which ones are not. So I don’t take any of them.
Q: Do you have any advice for our readers?
A: Eating healthfully in today’s society is very difficult because you’re fighting an entire food industry on your own— and that industry is trying to sell you the most profitable, least healthy foods available. But one thing you can do is read food labels. There’s a lot of information on them. If you’re looking at a packaged food and you can’t recognize the ingredients, or if you can’t purchase the ingredients at a supermarket, then it’s ultra-processed. There are certain ingredients that are indicators of ultra-processed foods. That would be color additives, flavor additives, and emulsifiers such as mono and diglycerides, polysorbates and carrageenan, and texturizers such as agar. I always read food labels. If something has a lot of artificial additives and ingredients that I don’t recognize, then I’m not going to eat it.
Marathon weekend is finally here and while the races are unquestionably the main event, runners and spectators alike look forward to seeing fun signs along the route.
However, there are some exceptions. “There are two signs people hate,” said Gary Brown Jr., founder and co-leader of the local running group Chasing Trail Philadelphia, “‘You're almost there’, especially when you're at, like, you know, Mile 13, and then ‘Worst parade ever’.”
As a city, let’s not add to Gary’s list. Use our sign generator to get some ideas.
What kind of sign are you going for?
What type of sign do you want to make?
story continues after advertisement
If you have other ideas or see a particularly creative sign, drop us a line at interactives@inquirer.com.
Marathon weekend can look chaotic — thousands of runners, crowds along the Parkway, and traffic everywhere — but it can also be one of the most fun, kid-friendly days in Philadelphia.
Between the Nemours Children’s Run, the Health and Fitness Expo, easy cheering spots, and plenty of stroller-friendly food stops, there’s a lot for families to enjoy without getting overwhelmed.
Here’s how to navigate the Philadelphia Marathon with kids in tow.
📍 Eakins Oval (22nd St. & Benjamin Franklin Parkway)
Kids run age-specific, short-distance dashes along the Parkway and get an event T-shirt, a finisher medal, and special goodies.
Nothing is timed, so the emphasis is fun. Children may only run in their age group, and each child is limited to one race. A parent or guardian must be present, but adults can’t run with the kids.
Come early. Before the races, kids can enjoy:
sports zone (football, baseball, basketball, soccer)
Runners on Walnut Street in Center City during the 2024 Philadelphia Marathon Sunday, Nov. 24, 2024.
Best viewing spots with kids
The marathon route stretches across Center City, Fairmount, and Manayunk. These spots are easiest for families:
Chestnut Street at Mile 1: High-energy, big crowds, and runners come through early — good for short attention spans. There’s room on side streets for stroller parking.
34th Street / University City (around Mile 5 and Mile 13): Wide sidewalks, walkable from the Parkway, and you can catch runners twice here if you hustle.
Manayunk’s Main Street (Miles 19–21): The loudest, most festive part of the race — think music, costumes, cowbells. Great for older kids; may feel crowded for toddlers.
Kelly Drive (Miles 22–24): Quieter stretch with room to spread out. Better for small kids and families who want to avoid packed sidewalks.
Cheering tip for kids: Have them call out runners’ names from their bibs — runners light up when a kid yells their name.
Getting Around: Transit, biking, and parking for families
Getting to the start/finish near the Art Museum is doable — especially with public transit.
SEPTA (big perk for parents)
Children 11 and under ride free with a fare-paying adult. Buses that usually stop near the Parkway (7, 32, 33, 38, 43, 48, 49) may be detoured. Check SEPTA’s System Status before you head out.
Regional Rail is helpful if you’re heading to Manayunk to cheer between Miles 19 and 21.
Driving & parking
Road closures are extensive, so expect detours and delays. If you plan to drive with kids, park early.
Amanda Carter and her children, Quinn, 3, and Cameron, 5, pose for a photo at 16th and Arch Streets at the start of the 2024 Philadelphia Marathon Sunday, Nov. 24, 2024. The kids had masks with dad Ron Carter’s face. They’re from New York City and this is Ron’s first marathon. Amanda who had done three, says “’m usually the one running.”
Kid-friendly sign ideas
If your kid needs inspiration, try:
You’re super fast! Like superhero fast!
Don’t stop! You’re almost at the snacks!
Run like you’re chasing the ice cream truck!
Go Birds! (And go YOU!)
My arms are tired from holding this sign!
My mom trained for months — I made this sign in five minutes!
Or have them tap through our Sign Generator for more options.
The gyros platter from Moustaki.
Where to eat with kids along the route
Whether you need a quick warm-up or a post-race reward, we rounded up 10 family-friendly places along (or just off) the course — from dumplings and giant slices to pancakes, burgers, and big dining rooms made for strollers.
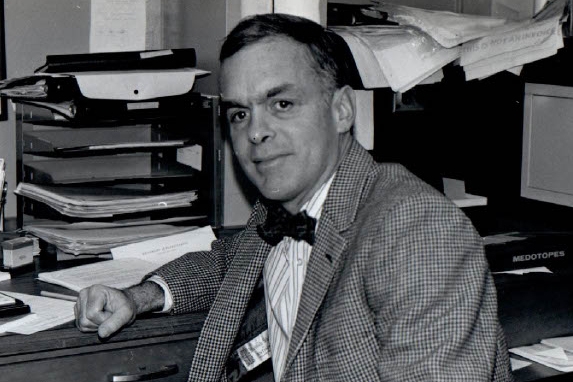
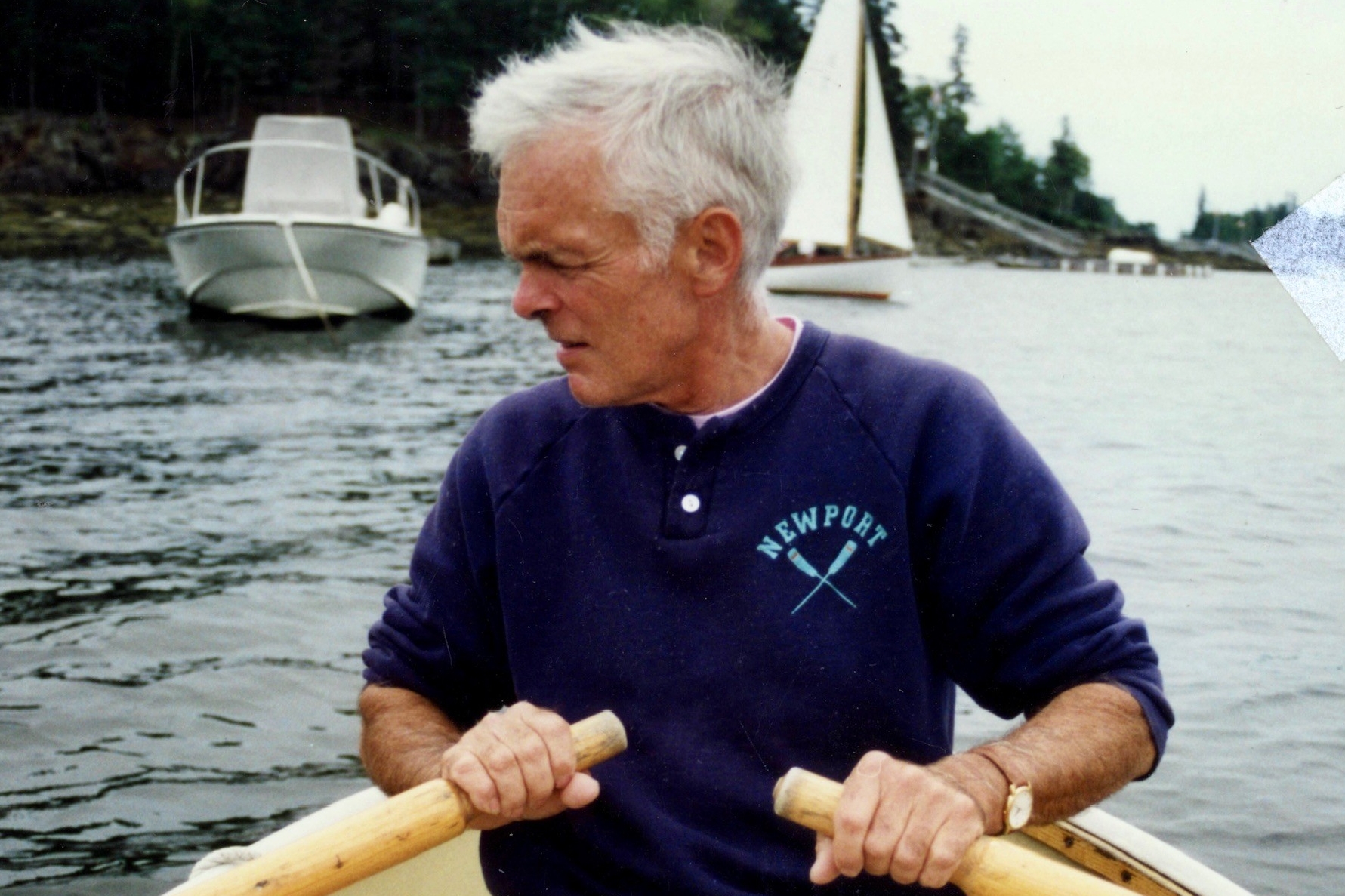
William L. Elkins, 93, of Coatesville, pioneering research immunologist at what is now the University of Pennsylvania’s Perelman School of Medicine, associate professor emeritus of pathology and laboratory medicine, innovative longtime Angus cattle rancher in Chester County, avid sailor, and veteran, died Tuesday, Nov. 11, of complications from pneumonia at Chester County Hospital.
The great-great-grandson of Philadelphia business tycoon William Lukens Elkins, Dr. Elkins fashioned his own distinguished career as a scientist, medical researcher, and professor at Penn from 1965 to 1985, and owner of the Buck Run Farm cattle ranch in Coatesville for the last 39 years.
At Penn, Dr. Elkins conducted pioneering research on how the human immune system fights infection and disease. He collaborated with colleagues in Philadelphia and elsewhere around the country to provide critical new research regarding bone marrow transplants and pediatric oncology.
His work contributed to new and more effective medical procedures at Penn, Children’s Hospital of Philadelphia, and elsewhere, and he instructed students and residents at Penn. But his lifelong love of the fields and rolling hills he roamed as a boy in Chester County never faded, he told Greet Brandywine Valley magazine in 2023.
Dr. Elkins was a lifelong outdoorsman.
“Farming is in my blood,” he said. “So even when I went to medical school and all that, the enthusiasm never left, and I wanted to go back to it.”
So he retired from medicine at 53, and he and his wife, Helen, bought nearly 300 acres of the old King Ranch on Doe Run Church Road in Coatesville. She kept the books and looked after the business. He became an expert on breeding cattle and growing the high-energy grass they eat.
Wearing floppy hats and riding a colorful ATV from field to field, Dr. Elkins worked his land for decades. He mended fences and tended daily to his 120 cows, heifers, and prize bulls.
He championed holistic regenerative farming and used new scientific systems to feed his cattle. He rejected commercial fertilizer and knew all about soil composition, grass growing, and body fat in cattle.
Dr. Elkins and his wife, Helen, married in 1966.
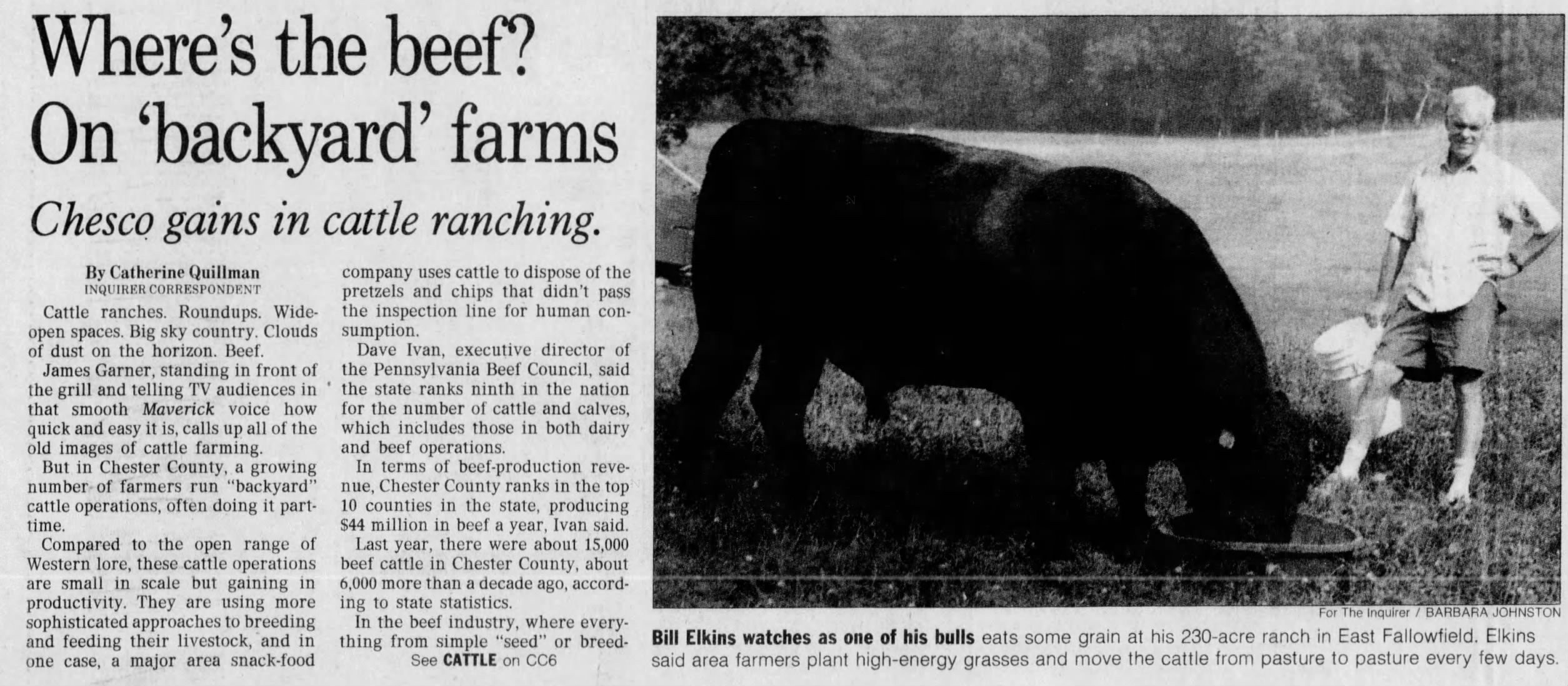
In a 1995 Inquirer story, he said: “Cattle are just like anyone else. If you just turn a few cattle out in a great big field, they will wander around, eat the grass they like best, and leave what they don’t want. That means the less desirable grasses tend to predominate.”
He traveled the country to confer with other cattlemen and helped found the Southeast Regional Cattlemen’s Association in 1994. He sold his beefsteaks, patties, jerky sticks, and kielbasa grillers to private customers online and to butchers and restaurants.
At least one local chef featured an item on the menu called Dr. Elkins’ Angusburger. Lots of folks called him Doc.
He earned his medical degree at Harvard University in 1958 and served two years in the Navy at the hospital in Bethesda, Md. He was a surgical intern in New York and discovered that he preferred the research lab. Before Penn, he worked at the Wistar Institute of biomedical research.
Dr. Elkins graduated from St. Mark’s School in Massachusetts in 1950.
Away from the lab, Dr. Elkins was an ocean sailor, expert navigator, and former boat club commodore. He was active with the Brandywine Conservancy, Natural Lands, and other groups, and was lauded by national organizations for his wide-ranging conservation and wildlife efforts.
He made his farm a haven again for the bobolink grassland songbird and other migratory birds and butterflies that had dwindled. “Buck Run Farm is more about growing grass and trees than beef,” he told Greet Brandywine Valley. “We’re blessed by the land.”
William Lukens Elkins was born Aug. 2, 1932, in Boston. He lived on the family dairy farm in Pocopson, Chester County, when he was young, went to boarding school in Massachusetts for four years, and earned a bachelor’s degree in biology at Princeton University.
He met Helen MacLeod at a party in Washington, and they married in 1966 and had a daughter, Sheila, and a son, Jake. They lived in Center City, Society Hill, and Villanova before moving to the farm. “He was easy to be with,” his wife said.
Dr. Elkins enjoyed sailing and fishing.
Dr. Elkins loved nature, fishing, and baseball, and he followed the Phillies, the Flyers, and other sports teams. “He had a wonderful bedside manner,” his daughter said. “He was a great listener. He really knew how to support people.”
His son said: “He was unassuming and direct. He spoke his mind. He connected with so many different people. He was curious about the world around him.”
His wife said: “He was thoughtful and always concerned about people. He had good humor. He was fun.”
In addition to his wife and children, Dr. Elkins is survived by five grandchildren and other relatives. A sister died earlier.
This article about Dr. Elkins and his ranch appeared in The Inquirer in 1995.
Tower Health’s preliminary financial report in August for fiscal 2025 showed a $5.9 million operating profit, a gain that came thanks for the sale of a shuttered hospital in Chester County.
But that apparent annual profit, the Berks County nonprofit’s first since 2017, turned into a $20.6 million loss when Tower released its annual audit.
Auditors from KPMG decided that Tower should boost medical malpractice reserves and give up on collecting millions owed by patients, Tower said in a statement.
“As part of our standard accounting process, the audited financials for the full year reflect increased malpractice insurance reserves and final adjustments to accounts receivable,” Tower said.
Most of the $26 million swing to a loss came from medical malpractice, but Tower also reduced what is called patient accounts receivable, representing unpaid bills, to $236.6 million from $251.6 million in August’s preliminary results, according to Tower’s audited financial statements that were published Friday.
Separately, Tower reported a $15.9 million operating loss for the three months that ended Sept. 30. That loss was a bit bigger than the $14.2 million loss in the same period last year. Tower’s revenue for the quarter was $501 million, up 4% from $479.8 million last year.
The results for the first quarter of 2026 did not include expenses for Tower’s layoff of 350 employees, or about 3% of its workforce, earlier this month. The cuts hit Pottstown Hospital particularly hard. Tower is eliminating 131 jobs there and eliminating some services.
The closures include the combined intensive care/critical care unit, the Pottstown location of the McGlinn Cancer Institute, and the hospital’s endoscopy center.
Two unions that represent Pottstown employees, the Pennsylvania Association of Staff Nurses and Allied Professionals and SEIU Healthcare Pennsylvania have decried the cuts and called on management to engage in discussions on how to preserve jobs and services.
Sherri Horsey Darden has no family history of brain cancer, nor has she been having persistent headaches, seizures, or any other symptoms that could suggest a tumor.
But when she heard the Brain Tumor Foundation, a New York-based charity, was offering free magnetic resonance imaging (MRI) brain scans in Philadelphia, she made sure to get an appointment.
“A lot of times people have things and don’t know,” she said.
She received her scan at Triumph Baptist Church of Philadelphia in North Philadelphia, where the foundation was offering scans last week to the general public. She’ll receive her results within a couple weeks.
The foundation has hosted these screening events for more than a decade, with the goal of promoting early detection of brain tumors.
Using MRI scans for preventive health screening hasgrown increasingly popular in recent years, with celebrities like Kim Kardashian touting expensive whole-bodyscans on social media.
But many doctors worry that the risks outweigh the benefits. They say that screening MRIs of the brain could lead to unnecessary surgeries and anxiety, and that catching a brain tumor early wouldn’t always change a person’s outcomes. These scans are not typically covered by insurance if not ordered by a doctor, and can cost anywhere from $1,000 to $10,000.
“There, to date, is no data available at all that would suggest that this is a useful approach,” said Stephen Bagley, a neuro-oncologist at Penn Medicine’s Abramson Cancer Center.
In the best scenarios, preventive medical screening can help catch diseases early when they are most treatable, and give people peace of mind. But they can also lead to overdiagnosis, false positives, unnecessary stress, and costlyfollow-up procedures.
This is why expert panels carefully evaluate which screening tools should berecommended to the general public. Decisions by the U.S. Preventive Services Task Force, considered the gold standard for evidence-based preventive care, weigh the potential harms involved against the likelihood of improving outcomes.
Even the most common screenings for cancer, like mammograms for breast cancer and PSA tests for prostate cancer, have faced controversy and shifting guidelines regarding who should get them and how frequently they should be administered.
There is no medical evidence showingthat mass MRI screening is helpful. Still, all spots for the foundation’s multiday screening event at Triumph Baptist Church were claimed. Zeesy Schnur, executive director of the foundation, said they aim to scan 100 to 150 people in each city.
Juanita Young, her husband, and her friend all booked consecutive appointments last week. Though she hasn’t had any symptoms that would make her think she had brain cancer, she signed up “just wanting to know,” she said.
Juanita Young, her husband, and her friend all booked consecutive appointments to get screened.
Philadelphia visit
The idea for the early detection campaign came from Patrick Kelly, a now retired neurosurgeon who started the foundation in 1998.
He was frustrated to see the majority of his brain cancer patients die from the disease, and felt that treatment would be more effective if the tumors were found earlier, explainedSchnur, who has been at the foundation since 2000.
Kelly envisioned a future where, similar to going through the scanners at an airport security checkpoint, people could get a full scan of their body, “and then this piece of paper would pop out and say, ‘Hey, you have a problem here,’” Schnur recalled.
The foundation offers brain MRIs for free at their events, covering the cost of administering the scan and having a radiologist read it. They use a portable MRI machine that only scans the brain and takes approximately 15 minutes.
The foundation has chauffeured its machine all over the country through its “Sponsor-A-City” program, which allows people to donate the funds needed to bring the unit to a city of their choice. They usually pick cities that are demographically diverse.
The event in Philadelphia was sponsored by Alexandra Schreiber Ferman, who lives in the area, through the more than $50,000 she raised from running the New York City Marathon.
Schreiber Ferman’s paternal grandfather died from glioblastoma and was a patient of Kelly’s. Her family has been involved with the foundation since its inception.
Schreiber Ferman got her first scan five or six years ago, after she had been having headaches. She pressured her parents to get her in for an MRI when the foundation’s unit was in Brooklyn.
“Thankfully, everything was OK. I just was stressed out,” she said.
Having a family history of the cancer makes her and her family more alert when it comes to headaches and other symptoms. Schreiber Ferman received her second scan Tuesday morning at the screening event.
Alexandra Schreiber Ferman sponsored the Brain Tumor Foundation’s event in Philadelphia.
She said her family and people at the foundation feel that these scans should be “something that’s routine,” like mammograms and skin checks.
“My goal would be that getting a brain scan becomes just a routine part of aging,” she said.
Her father, who serves as chairman of the foundation, wants other people to have the chance to get screened and has helped sponsor past city visits.
However, he himself has only gotten one screening since the program first started, and no longer wants any more.
“My dad is adamant that he does not want to get a scan. I think for him, ‘ignorance is bliss,’” she said.
What doctors say
Screening tests have to meet certain criteria in order to become standard practice, explained Richard Wender, chair of family medicine and community health at Penn and former chief cancer control officer for the American Cancer Society.
A national leader in cancer screening, he would not recommend that people undergo MRIs to screen for brain cancer.
The first criteria for a screening tool to be recommended for the general population is that the disease is common, he said. The disease must also come with a high risk of harm or death and must have stages, so that it can be found before it causes symptoms.
Lastly, available treatments for the disease have to be able to reduce the risk of serious outcomes.
Brain cancer is unlikely to ever meet that criteria, Wender said, mainly because it isn’t common enough. There also isn’t sufficient evidence that finding a brain cancer earlier reduces the risk of a person dying from it.
For example, the most common malignant brain tumor, glioblastoma, is so aggressive and invasive from the start, it is always considered a grade four tumor, noted Bagley, who serves as section chief of neuro-oncology at Penn.
These cancers grow so quickly that the time between the tumor developing and someone showing up to the emergency room with symptoms is typically on the order of months, he said.
“You cannot cure it, no matter when you find it,” Bagley said.
A subset of brain tumors called grade two gliomas are slow-growing enough that catching them earlier could give a patient a better outcome. However, “it’s so rare, you’d have to do so many of these MRIs to find those tumors,” he said.
Another issue with screening the general population is that there will inevitably be false positives.
Some abnormalities in the brain might look like possible tumors on MRIs but turn out to be harmless.
Yet, the person would have to undergo a medical procedure, such as a brain biopsy, to prove that it isn’t cancer.
“You end up putting the patient through invasive brain procedures, lots of anxiety, and existential distress for what ends up to be nothing,” Bagley said.
The same goes for benign brain tumors like meningioma, the most common type of brain tumor in adults. Roughly 39,000 cases are reported each year in the United States. A “very tiny percentage” of these ever become malignant, and it’s unknown if catching them early would help the patient in the long run, Bagley said.
It might just mean the patient has to get MRIs every year for the rest of their life, or get surgery to remove a tumor that probably never would have been become a problem.
Some of these patients have ended up seeking follow-up care fromRicardo Komotar, a neurosurgeon who directs the University of Miami Brain Tumor Initiative in Florida, after finding out they had benign tumors from screening MRIs. He tells these “super nervous” patients that it’s nothing to worry about, but now that they’ve found it, he has to follow it.
As of right now, there is no good screening mechanism when it comes to the brain, Komotar said. He recommends only imaging a person’s brain if there’s a reason, such as a seizure, weakness, or migraines, or an injury, such as in a car accident.
“Brain MRIs as screening have not been proven to help and, in my experience, they only hurt,” Komotar said.
More research needed
Ethan Schnur checks on James Brown as he has his early detection brain tumor screening at the Brain Tumor Foundation event in Philadelphia.
When the foundation first started offering scans, they were finding potential abnormalities in one out of every 100 people they screened. Those included anything from a brain tumor, to silent stroke, to an aneurysm.
One example was a man from Staten Island who had no symptoms, but through the scan, found out he had a nonmalignant brain tumor. He got surgery to remove it.
“He called us afterward to thank us,” Schnur said.
Their stance is that these MRIs should be part of standard of care, so that anyone who wants one has the option.
The foundation has partnered with Weill Cornell Medicine and NewYork-Presbyterian in New York City for a formal research study using data from their screening events.
John Park, the lead researcher and chief of neurosurgery at NewYork-Presbyterian Queens Hospital, said the study will help assess whether screening MRIs for a general populationcould be useful. They aim to screen up to thousands of patients.
“We don’t know if it will be effective or not,” Park said.
If the study were to suggest the scans are effective, there would still need to be a large randomized trial to validate those conclusions, Wender said.
Park’s team will also look at demographic information in an effort to identify risk factors for brain tumors and other abnormalities.
Research into risk factors could help justify whether certain populations should get routine screeningMRIs, Bagley said. He noted that patients with Li-Fraumeni syndrome, a rare genetic disease that predisposes people to developing cancer, are already recommended to get whole-body MRI scans yearly because they’re known to be at such high risk.
Other than those patients, “we don’t really have any way to say this large group of patients is at high risk for this type of brain tumor,” Bagley said.
A handful of patients have ended up seeking care at Penn from Bagleyafter paying for a whole-body MRI from a private company. These are people who were “completely fine” before happening to find a brain tumor on their scans, he said.
One of them was diagnosed with glioblastoma.
He isn’t sure yet whether being diagnosed earlier will actually extend the patient’s survival time. It might just mean the patient gets a few months’ head start on treating the tumor.
“It’s totally unclear if he did himself any justice by finding this terrible brain cancer any earlier. It’s incurable either way,” Bagley said.
A 47-year-old man from New Jersey died within hours of eating a hamburger at a barbecue in the summer of 2024.
He had no major medical problems prior, nor did his autopsy find a cause of death.
But several months later, researchers at the University of Virginia pieced together a diagnosis: severe anaphylaxis linked to alpha-gal syndrome. It was a tick-related red meat allergy the man didn’t know he had.
He would turn out to be the first documented death from anaphylaxis related to the red meat allergy, according to a study published Wednesday in the Journal of Allergy and Clinical Immunology: in Practice.
In most cases of alpha-gal syndrome, the culprit is a Lone Star tick, which can transmit a sugar molecule called alpha-gal to a person during a bite. This can trigger the person’s immune system to react to the molecule, also found in meat from mammals, including beef, pork, and lamb, and in dairy and gelatin products.
The man had received 12 to 13 bites around his ankles earlier that summer from what his wife had thought were “chiggers.”
However, the bites were likely from the larvae of Lone Star ticks, which look similar to chiggers.
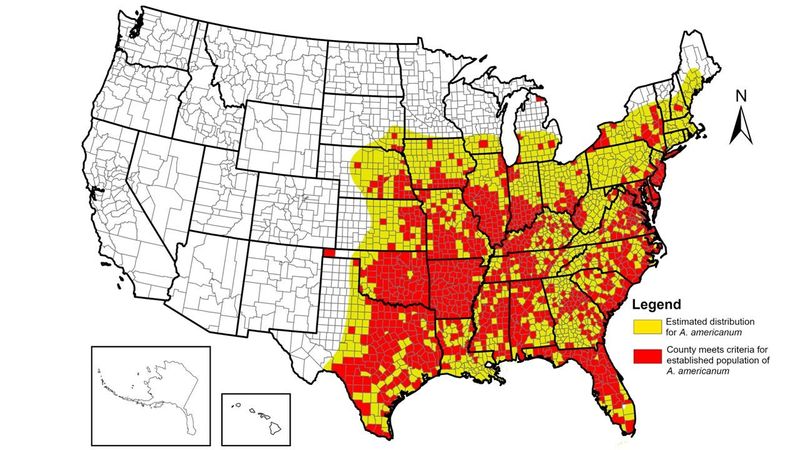
Lone star ticks are native to the eastern United States, but were traditionally limited to southern states because of deforestation in early America. Forest regrowth and climate change have helped the ticks reclaim their territory and expand.
Lone star ticks have been found in Pennsylvania since 2011, including in Bucks, Chester, Delaware, and Philadelphia Counties. A 2008 Rutgers study found them in every South Jersey county.
The man who died was not identified in the newly published case study, nor was it revealed where he lived in New Jersey.
The Centers for Disease Control and Prevention says nearly a half-million people are suffering from alpha-gal syndrome nationwide.
Although this is the first deadly case documented that’s linked to the red meat allergy, reactions to the alpha-gal sugar in the targeted cancer therapy cetuximab have led to other deaths, however this is rare.
Researchers say the man’s case calls for increased awareness of the symptoms of anaphylaxis, which go beyond hives and trouble breathing.
“If you get the worst abdominal pain in your life, you need to consider the possibility of an allergic reaction,” said Thomas Platts-Mills, an allergist and immunologist at the University of Virginia and lead author on the study.
A map shows the estimated area in which Lone star ticks are found in America.
What happened
The 47-year-old airline pilot had gone on a camping trip in an unidentified location with his wife and children back in summer 2024. They spent the whole day outside, followed by a meal of beef steak at 10 p.m. It was an unusual choice for the family, who normally ate chicken.
Four hours later, the man woke up with abdominal pain that became so severe that he “was writhing in pain,” according to the study’s recount of the events. That was paired with diarrhea and vomiting.
After a couple of hours, his symptoms improved, and he fell back asleep.
The next morning, he rose feeling well enough to get a five-mile walk in before breakfast.
He thought about consulting a doctor, but ultimately decided against it, unsure what he would say happened. Separately, he told one of his sons that he thought he was going to die during the episode.
Two weeks passed, and the family, now home in New Jersey, attended a barbecue where the man ate a hamburger at around 3 p.m. He went home and spent an hour mowing the lawn.
A few hours later, his son found him unconscious on the bathroom floor, surrounded by vomit.
His son called 911 at 7:37 p.m. and initiated resuscitation until the paramedics arrived, but even after his father was transferred to the hospital, doctors could not save the man.
An autopsy found no obvious problems with his heart, lungs, brain, or abdomen, and concluded it was a “sudden unexplained death.”
The man’s wife, however, asked her friend, a pediatrician, to review the autopsy report. Suspecting the man could have had alpha-gal syndrome, the pediatrician contacted Platts-Mills, who first identified the syndrome back in 2007.
Solving the mystery
When Platts-Mills heard that the postmortem report gave no cause of death, he thought, “You can’t leave this lady losing her 47-year-old husband for no reason. That’s impossible.”
He arranged for a sample of the man’s blood to be sent to his lab for testing.
When they received it in April, their first move was to screen for a protein called immunoglobulin E, which the immune system releases during allergic reactions. They wanted to know whether his body was sensitive to anything it shouldn’t have been.
Unsurprisingly, the test came back positive for rye grass and ragweed, two common seasonal allergens.
But so did two other substances: alpha-gal and beef.
While this helped establish his allergy to alpha-gal, their next step was to confirm whether he had anaphylaxis when he died. They sent the sample to be tested for an enzyme called tryptase, which the body releases during severe allergic reactions. High levels could indicate that he died from severe anaphylaxis.
Not long after, a scientist called Platts-Mills to apologize and tell him they had to redo the test.
Platts-Mills thought, “Oh my god, was it negative?”
Instead, the scientist would tell him the levels of tryptase were bafflingly high.
At over 2,000 nanograms per milliliter, there was so much tryptase in his system that they needed to dilute the sample and retake the value. That number astonished Platts-Mills, who himself had never seen levels surpass 200 nanograms per milliliter.
“It absolutely says that he died of anaphylaxis,” Platts-Mills said.
It is unclear why he had such a severe case of anaphylaxis. While the study listed some factors, such as his drinking beer with his burger and being exposed to ragweed pollen, that potentially could have influenced his outcome, Platts-Mills said these “probably weren’t really the reasons why his anaphylaxis was more severe.”
Anaphylaxis very rarely causes death. One study found only 0.3% of cases in the emergency room are fatal.
One of the takeaways from the man’s experience is not to ignore abdominal pain, Platts-Mills said. While many people know to look out for more common signs of anaphylaxis, such as hives and difficulty breathing, having abdominal pain without other symptoms can be a dangerous form of the reaction.
In most cases, this pain takes three to five hours to show up after eating red meat. Had the man known his previous episode of abdominal pain was anaphylaxis, he could’ve avoided eating the burger.
“That’s the tragedy from my point of view,” Platts-Mills added.
Sam Moore suffers from Alpha-gal syndrome, which is brought on by an invasive tick bite. He is shown here at his cranberry farm in Tabernacle, N.J. in August 2023.
Living with alpha-gal syndrome
Samuel Moore, a cranberry farmer in Shamong, deep in the New Jersey Pinelands in Burlington County, has had many close calls and a handful of hospital visits due to alpha-gal. He was diagnosed several years ago and knows a handful of other locals who’ve been bitten and diagnosed.
So far, Moore said there’s been no treatment that’s helped.
“The only treatment,” he said,” is vigilance.”
That means exhaustive label reading at the grocery store, rarely, if ever, dining out, and getting to know local deli owners personally. Moore said he could have a flare-up due to proteins left over on a lunchmeat slicer.
“I’ve come to the point where I’ve felt anaphylaxis coming on and my throat closing up,” he said. “It’s not just breaking out in hives.”
Moore recently celebrated his 52nd birthday at a plant-based restaurant in Haddonfield, where he was able to eat anything on the menu.
“And I’ll tell you, I was still a little nervous,” he said.
One of Moore’s friends, Albertus “Chippy” Pepper, also contracted alpha-gal syndrome. Like Moore, he’s a cranberry farmer, often outside in the bogs or clearing brush. His new diet has become a little bland.
“I eat chicken, chicken, chicken, and more chicken,” he told The Inquirer in 2023.
Editor’s note: The story has been updated to clarify that cetuximab is a targeted cancer therapy.
Pennsylvania’s new budget has $5 million in supplemental payments for the two Delaware County Hospitals that have seen significant increases in patient volumes since Crozer-Chester Medical Center and Taylor Hospital closed in the spring.
Main Line Health’s Riddle Hospital, near Media, is getting $3 million. The amount for Trinity Health Mid-Atlantic’s Mercy Fitzgerald Hospital, in Darby, is $2 million, according to budget documents.
The $5 million will be doubled by a federal match, said Democratic State Sen. Tim Kearney, who represents part of Delaware County. The $5 million is from a fund used to help hospitals the serve a large number of patients with Medicaid and used to go to Crozer Health, Kearney said Friday.
“Since Crozer’s shutdown in April, Riddle’s Emergency Department has experienced an unprecedented surge — 46% more patients than the same period last year, an increase of nearly 4,000 overall,“ the nonprofit said.
Main Line, which also owns Lankenau Medical Center, Bryn Mawr Hospital, and Paoli Hospital, said it has seen 55,000 patients from the Crozer market — a 15% increase over the same time period last year. That figure includes 8,000 patients who went to a Main Line facility for the first time, the health system said.
Trinity Health did not respond to a request for comment.
Shuttered hospitals in limbo
While Riddle and Mercy Fitzgerald have scrambled to accommodate patients who used to rely on Crozer Health, efforts are underway to bring healthcare services back to at least Taylor Hospital in Ridley.
A group from New Jersey called Chariot Allaire Partners LLC has agreed to pay $10 million for the former Crozer-Chester Medical Center in Upland but has not disclosed its plans. That facility served as a key safety provider for a low-income area of Delaware County.
A partnership of Restorative Health Foundation and Syan Investments won an auction for Springfield Hospital for $3 million, but it does not have support from township officials.
Delaware County legislators also obtained $1 million from the state to buy emergency department equipment if one of the closed hospitals, such as Taylor, reopens, Kearney said.
Editor’s note: This story has been updated with additional detail on the funding.
This suburban content is produced with support from the Leslie Miller and Richard Worley Foundation and The Lenfest Institute for Journalism. Editorial content is created independently of the project donors. Gifts to support The Inquirer’s high-impact journalism can be made at inquirer.com/donate. A list of Lenfest Institute donors can be found at lenfestinstitute.org/supporters.
Philadelphia will host its largest marathon yet this year, as about 15,000 runners take on the 26.2-mile race through the city’s scenic and historic neighborhoods.
The Philadelphia Marathon Weekend runs Nov. 21-23 and includes a half marathon (13.1 miles) and an 8K race. The first marathon was held in 1994 with just 1,500 participants; this year, organizers expect roughly 30,000 athletes across all races.
With that many runners and spectators, expect road closures, parking restrictions, and heavy traffic.
“We want to make sure people give themselves ample time to get there,” said race director Kathleen Titus. “We have new security screenings that will speed things up, but if you’re waiting until 15 minutes before the race, you might be standing in a line for about an hour.”
Runners on Walnut Street in Center City during the 2024 Philadelphia Marathon on Sunday, Nov. 24, 2024.
Titus said the marathon has a new website and updated app. The app allows runners to schedule packet-pickup times at the expo to cut down on lines, track live race results, and receive weather and safety alerts.
Race start times and locations for the Philadelphia Marathon
All races follow the same course layout as in previous years and — except for the Nemours Children’s Run — start at 22nd Street and Benjamin Franklin Parkway, near the Philadelphia Museum of Art. The Nemours Children’s Run begins at Von Colln Memorial Field, 2276 Pennsylvania Ave., adjacent to Eakins Oval.
Each race follows a unique route, with the marathon and half-marathon winding through Center City, Chinatown, Old City, Queen Village, Rittenhouse, and University City, with significant portions covering Fairmount Park, Kelly Drive, and the Benjamin Franklin Parkway.
The Expo is filled with vendors showcasing apparel, shoes, gear, free product samples, and educational booths on health and fitness. Friday and Saturday bring a speaker series to the Expo and meet-and-greets with some of the country’s top runners. On Friday evening, there will be activities for children.
For spectators of the Philadelphia Marathon
Spectators are welcome to line the race routes to cheer on runners but will be restricted from the starting lines and in secure running areas until after 8 a.m. on Saturday and Sunday to ensure smooth race starts.
Large umbrellas, coolers, and animals (except ADA service dogs) are not allowed. The marathon also discourages bringing large blankets, backpacks, or cameras.
William Loevner of Pittsburgh is embraced by his wife, Emma Loevner, after finishing first in the mens in the 2024 Philadelphia Marathon on Sunday, Nov. 24, 2024.
Road closures
All-weekend closures
Saturday, Nov. 22, through 5 p.m. Sunday, Nov. 23
Benjamin Franklin Parkway (all lanes) between 22nd Street and Eakins Oval
Kelly Drive (inbound) closed at 25th Street, with local traffic permitted to Anne d’Harnoncourt Drive
Spring Garden Street Bridge and MLK Drive (inbound) traffic detoured onto 24th Street
Spring Garden Street
Saturday, Nov. 22
2 a.m. closures
2000—2400 Benjamin Franklin Parkway (inner and setup areas as posted)
Spring Garden Street, from Pennsylvania Avenue to Benjamin Franklin Parkway
23rd Street, from Pennsylvania Avenue to Benjamin Franklin Parkway
22nd Street, from Winter Street to Park Towne Place (local access to Park Towne Place maintained)
21st Street, from Pennsylvania Avenue to Winter Street
4 a.m. closures
Interstate 676 off-ramp at 22nd Street (westbound)
Interstate 76 off-ramp at Spring Garden Street (eastbound)
6 a.m. closures
17th Street, from Arch Street to Vine Street
18th Street, from Arch Street to Callowhill Street
19th Street, from Arch Street to Callowhill Street
20th Street, from Arch Street to Callowhill Street
21st Street, from Arch Street to Spring Garden Street
22nd Street, from Arch Street to Spring Garden Street
Benjamin Franklin Parkway, from 16th Street to 20th Street
Market Street, from Sixth Street to 16th Street
Chestnut Street, from Fifth Street to Eighth Street
Sixth Street, from Market Street to Chestnut Street
Fifth Street, from Chestnut Street to Race Street
South Penn Square
Juniper Street, from Chestnut Street to Market Street
John F. Kennedy Boulevard, from Juniper Street to 17th Street
15th Street, from Race Street to Chestnut Street
16th Street, from Chestnut Street to Race Street
Race Street, from Sixth Street to Columbus Boulevard
Columbus Boulevard (southbound lanes), from Vine Street to Washington Avenue
Interstate 95 southbound off-ramp at Washington Avenue
Washington Avenue, from Columbus Boulevard to Front Street
Front Street, from Washington Avenue to South Street
South Street, from Front Street to Seventh Street
Sixth Street, from Bainbridge Street to Locust Street
Lombard Street, from Fifth Street to Broad Street
13th Street, from Bainbridge Street to Chestnut Street
Walnut Street, from 12th Street to 34th Street
34th Street, from Chestnut Street to Girard Avenue
Spring Garden Street, from 32nd Street to 34th Street
Girard Avenue, from 33rd Street to 38th Street
33rd Street, from Girard Avenue to Cecil B. Moore Avenue
Reservoir Drive, from 33rd Street to Diamond Drive
Mt. Pleasant Drive
Fountain Green Drive
Kelly Drive
Access and reopening
Local access for residents and businesses will be maintained at police-controlled points.
Access to the Philadelphia Museum of Art will be available via Spring Garden Street (Bridge and Tunnel) to Anne d’Harnoncourt Drive.
Police will allow traffic through intersections when possible, depending on runner flow.
All streets (except Eakins Oval and the Parkway) are scheduled to reopen by 2 p.m. Saturday; many Center City roads will reopen earlier as they are cleared and serviced.
Sunday, Nov. 23
As part of enhanced security for the AACR Philadelphia Marathon, “No Parking” regulations will be strictly enforced. Vehicles on the race route will be relocated beginning at 1 a.m. Sunday.
2 a.m. closures
2000—2400 Benjamin Franklin Parkway
Spring Garden Street, from Pennsylvania Avenue to Benjamin Franklin Parkway
23rd Street, from Pennsylvania Avenue to Benjamin Franklin Parkway
22nd Street, from Winter Street to Park Towne Place (local access maintained)
21st Street, from Pennsylvania Avenue to Winter Street
4 a.m. closures
Interstate 676 off-ramp at 22nd Street (westbound)
Interstate 76 off-ramp at Spring Garden Street (eastbound)
6 a.m. closures
17th Street, from Arch Street to Vine Street
18th Street, from Arch Street to Callowhill Street
19th Street, from Arch Street to Callowhill Street
20th Street, from Arch Street to Callowhill Street
21st Street, from Arch Street to Spring Garden Street
22nd Street, from Arch Street to Spring Garden Street
Benjamin Franklin Parkway, from 16th Street to 20th Street
Arch Street, from Third Street to 16th Street
Fourth Street, from Arch Street to Vine Street
Race Street, from Sixth Street to Columbus Boulevard
Columbus Boulevard (southbound lanes), from Vine Street to Washington Avenue
Interstate 95 southbound off-ramp at Washington Avenue
Washington Avenue, from Columbus Boulevard to Front Street
Front Street, from Washington Avenue to South Street
South Street, from Front Street to Seventh Street
Sixth Street, from Bainbridge Street to Market Street
Chestnut Street, from Sixth Street to 15th Street
15th Street, from Chestnut Street to Walnut Street
Walnut Street, from Broad Street to 34th Street
34th Street, from Chestnut Street to Girard Avenue
Lansdowne Drive, from Girard Avenue to South Concourse Drive
South Concourse Drive, from Lansdowne Drive to West Memorial Hall Drive
East Memorial Hall Drive, from South Concourse Drive to Avenue of the Republic
Avenue of the Republic, from East Memorial Hall Drive to Catholic Fountain
Belmont Avenue, from Montgomery Drive to Parkside Avenue
States Drive, from Lansdowne Drive to Girard Avenue
Girard Avenue Bridge, from Lansdowne Drive to 33rd Street
33rd Street, from Girard Avenue to Reservoir Drive
Reservoir Drive, from 33rd Street to Edgley Drive
Edgley Drive, from Reservoir Drive to Fountain Green Drive
Fountain Green Drive, from Edgley Drive to Kelly Drive
Kelly Drive
Falls Bridge
Ridge Avenue, from Schoolhouse Lane to Manayunk Avenue
Main Street (Manayunk), from Ridge Avenue to Conarroe Street
Access and reopening
Local access for residents and businesses will be maintained at police-controlled points.
Access to the Philadelphia Museum of Art will be available via Spring Garden Street (Bridge and Tunnel) to Anne d’Harnoncourt Drive.
Expect delays at crossings along the course; police will allow traffic through when possible.
All streets (except Eakins Oval and the Parkway) are scheduled to reopen by 3 p.m. Sunday; many Center City roads will reopen earlier as they are cleared and serviced.
Transportation to the races
🚌 Bus
Lines 7, 32, 38, 43, 48, and 49 drop riders within a two-minute walk from the Art Museum. But, due to the race, there will most likely be detours. Check SEPTA’s system status for the latest schedules.
The race’s starting line is within a 10-minute ride from the City Hall area and subway stop and other locations. Check the map of Indego bike share stations to rent bikes and return them at a station near the Art Museum.
16th & Race St. (Sheraton Hotel), Standard Parking, (215) 196-0293
1815 JFK Boulevard, Central Parking System, (215) 568-8030 (Entrance on 1850 Cuthbert St.)
1901 JFK Boulevard, Central Parking System, (215) 557-3821 (Entrance on 19th Street)
1700 Benjamin Franklin Parkway, the Windsor Suites, (215) 569-0899
36 S. 19th St., Central Parking System, (215) 561-1187
Where does the money go?
Revenue earned and money raised from the Philadelphia Marathon goes to various charities and nonprofits, including local ones like B Inspired Philadelphia and the Mazzoni Center.
Naomi Peker (left) and Srivki Weisberg (right) jump to celebrate their finish in the 2024 Philadelphia Marathon on Sunday, Nov. 24, 2024. They run with a club in Suffern, N.Y., and this was Peker’s first marathon.
Awards & prize money
Monetary prizes range from $225 to $10,000 depending on the race, with the Philadelphia Marathon’s Elite Division being the most competitive.