Jefferson Health says it will terminate Lehigh Valley Health Network’s contracts with UnitedHealthcare next year, stating United, the nation’s largest health insurer, is paying less than their negotiated rates, Jefferson said Monday.
The contracts will remain in effect until Jan. 26 for Medicare Advantage patients and until April 25 for patients with commercial insurance through their employer. In the last 18 months, Lehigh Valley Health facilities treated 70,000 people with United insurance, Jefferson said.
“Like all health systems, we are facing significant headwinds as costs rise faster than reimbursement,” Mark Whalen, Jefferson’s chief strategy and transformation officer, said in an email.
“When reimbursement falls substantially below negotiated levels, it threatens our ability to fulfill our mission of providing exceptional care to all patients.”
Whalen said Jefferson will continue working to secure a better deal with United, as it has for more than two years.
United said in a statement that its most recent proposal went to Lehigh Valley in April. “We have yet to receive a counter proposal from the health system, whose last proposal was provided in December 2024 and included a near 30% price hike in the first year of our contract,” the statement said.
Jefferson countered with a statement saying that its dealings with United are not part of a normal contract renegotiation. “This ongoing dispute is caused by United Healthcare’s implementation of a multiyear 30% price decrease that was not agreed to, not accepted and is not sustainable, Whalen said.
The timing of the United announcement is noteworthy. Medicare Advantage open enrollment is underway until Dec. 7 for plans that take effect Jan. 1.
The potential termination of United’s Medicare plans on Jan. 26 puts United’s customers who depend on Lehigh Valley for health services in a quandary. Should they stick with United or switch to another plan, such as those offered by Jefferson’s insurance arm?
United said Jefferson’s decision to make its announcement during open enrollment looked like “a negotiating tactic.”
The Minnesota company has about 27,500 Medicare Advantage enrollees in the main counties served by Lehigh Valley Health doctors, according to federal data from September.
The impasse does not affect Philadelphia-area Jefferson patients with insurance from UnitedHealthcare.
Insurance regulations require notice to patients before contracts end.
In March, Jefferson went out-of-network with Cigna Health for a few weeks during a similar impasse in negotiations. Jefferson and Cigna quickly reached a deal after the termination.
The worst of the coronavirus pandemic that started nearly six years ago is well in the past, but Philadelphia’s biggest nonprofit health systems are still contending with the financial disruption unleashed by the virus that led to thousands of deaths in the area.
Operating conditions for hospitals started improving in 2023, but “the slope of the recovery is a bit more shallow than a lot of health systems had planned for,” said Mark Pascaris, a senior director at Fitch Ratings, one of three major credit ratings agencies.
Patients have returned, but the pandemic led to a resetting of expensesfor labor and supplies at a higher level, Pascaris said. “That’s been the challenge over the last two or three or four years now, trying to manage through a very challenging expense situation,” he said.
To show how the financial landscape has changed, The Inquirer compiled financial data for the region’s six biggest health systems that have fiscal years ending June 30 each year. The analysis compared average operating profits in three years before the pandemic (fiscal years 2017-19) to the results in most recent three years (fiscal years 2023-25).
All six systems showed a substantial drop in a measure of earnings that excludes certain accounting expenses and interest costs. This slice of financial results is known as earnings before interest, depreciation, and amortization. Abbreviated as EBIDA, it’s a primary indicator watched by influential credit ratings agencies.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
The experience of Children’s Hospital of Philadelphia clearly illustrates what has happened: The organization’s aggregate revenue in the most recent three fiscal years was 58% higher than it was in the three years that ended June 30, 2019, but its EBIDA climbed only by half a percentage point.
“Hospitals and healthcare systems across the country continue to face significant headwinds, driven by reimbursement challenges, increased supply and labor costs, uncertain governmental pressures, and the continued ripple effect of the pandemic,” CHOP said in a statement.
Officials at ChristianaCare, Main Line Health, and Temple University Health System echoed CHOP’s remark.
“Margins were far better prior to the pandemic, largely due to lower supply and labor costs,” Main Line’s chief financial officer Leigh Ehrlich said. “Those costs rose sharply during the pandemic and continue to rise.”
ChristianaCare’s CFO Rob McMurray noted: Not only have Medicare and Medicaid rates not kept up with inflation, but more people have those government forms of insurance for people 65 and older and for low-income people.
The nonprofit is expanding from its base in northern Delaware to Southeastern Pennsylvania and is expanding alternative formats, such as hospital-care-at-home and micro hospitals, to reduce costs, McMurray said.
A significant worry for Temple University Health System is the impact of the 2025 budget reconciliation bill, sometimes called the One Big Beautiful Bill Act. The North Philadelphia nonprofit estimates that Medicaid cuts in that law will cost it $519 million over the next 10 years, said Jerry Oetzel, the system’s CFO.
Have you ever tossed and turned under a full moon and wondered if its glow was keeping you awake? For generations, people have believed that the Moon has the power to stir up sleepless nights and strange behavior — even madness itself. The word “lunacy” comes directly from luna, Latin for Moon.
The answer is, of course, more nuanced than folklore suggests. Research shows a full moon can modestly affect sleep, but its influence on mental health is much less certain.
I’m a neurologist specializing in sleep medicine who studies how sleep affects brain health. I find it captivating that an ancient myth about moonlight and madness might trace back to something far more ordinary: our restless, moonlit sleep.
What the full moon really does to sleep
Several studies show that people really do sleep differently in the days leading up to the full moon, when moonlight shines brightest in the evening sky. During this period, people sleep about 20 minutes less, take longer to fall asleep, and spend less time in deep, restorative sleep. Large population studies confirm the pattern, finding that people across different cultures tend to go to bed later and sleep for shorter periods in the nights before a full moon.
The changes are modest. Most people lose only 15 to 30 minutes of sleep, but the effect is measurable. It is strongest in places without artificial light, such as rural areas or while camping. Some research also suggests that men and women may be affected differently. For instance, men seem to lose more sleep during the waxing phase, while women experience slightly less deep and restful sleep around the full moon.
Modern science adds an important twist. Research is clear that sleep loss itself is a powerful driver of mental health problems. Even one rough night can heighten anxiety and drag down mood. Ongoing sleep disruption raises the risk of depression, suicidal thoughts, and flare-ups of conditions like bipolar disorder and schizophrenia.
But here’s the catch: When researchers step back and look at large groups of people, the evidence that lunar phases trigger psychiatric crises is weak. No reliable pattern has been found between the Moon and hospital admissions, discharges, or lengths of stay.
But a few other studies suggest there may be small effects. In India, psychiatric hospitals recorded more use of restraints during full moons, based on data collected between 2016 and 2017. In China, researchers noted a slight rise in schizophrenia admissions around the full moon, using hospital records from 2012 to 2017. Still, these findings are not consistent worldwide and may reflect cultural factors or local hospital practices as much as biology.
In the end, the Moon may shave a little time off our sleep, and sleep loss can certainly influence mental health, especially for people who are more vulnerable. That includes those with conditions like depression, bipolar disorder, schizophrenia, or epilepsy, and teenagers who are especially sensitive to sleep disruption. But the idea that the full moon directly drives waves of psychiatric illness remains more myth than reality.
The gravitational forces that move oceans are far too weak to affect human physiology, and studies of geomagnetic and atmospheric changes during lunar phases have yielded inconsistent or negligible results. This makes sleep disruption from nighttime light exposure the most plausible link between the Moon and human behavior.
Why the myth lingers
If the science is so inconclusive, why do so many people believe in the “full moon effect”? Psychologists point to a concept called illusory correlation. We notice and remember the unusual nights that coincide with a full moon but forget the many nights when nothing happened.
The Moon is also highly visible. Unlike hidden sleep disruptors such as stress, caffeine, or scrolling on a phone, the Moon is right there in the sky, easy to blame.
Lessons from the Moon for modern sleep
Even if the Moon does not drive us “mad,” its small influence on sleep highlights something important: Light at night matters.
Our bodies are designed to follow the natural cycle of light and dark. Extra light in the evening, whether from moonlight, streetlights, or phone screens, can delay circadian rhythms, reduce melatonin, and lead to lighter, more fragmented sleep.
In our modern world, artificial light has a much bigger impact on sleep than the Moon ever will. That is why many sleep experts argue for permanent standard time, which better matches our biological rhythms.
So if you find yourself restless on a full moon night – and you’ll have a chance to test this come Nov. 5 – you may not be imagining things, because the Moon can tug at your sleep. But if sleeplessness happens often, look closer to home. It is likely a culprit of the light in your hand rather than the one in the sky.
It was magical. I clicked the record button on my cell phone, placed it on the exam room desk, turned away from the computer, and began a conversation with my patient. After we completed the visit, I went back to my office and opened her electronic record — and found a clear, concise narrative description of our encounter, complete with my physical exam findings and a numbered problem list, plus assessments and follow up plans.
I did not write these medical notes — an artificial intelligence scribe called DAX (Dragon Ambient eXperience) Copilot did. And it was nearly perfect.
AI scribes are new, but not brand new. I am actually a little late to the game. You may have already noticed that some of your own doctors are using this technology during office visits. DAX was developed by an AI and speech recognition company called Nuance that was acquired by Microsoft in 2022. First, clinical conversations are recorded using a cell phone mobile app. AI then processes the recording and generates a progress note, minimizing computer distraction and allowing clinicians to focus more attention on our patients.
In the last couple of years, I have read everything I can find about AI, a new frontier that will be a growing presence in clinical medicine. Until now, I’ve also done a great job convincing myself not to use an AI scribe — one of the most accessible current AI tools.
By typing brief notes with lots of abbreviations, I worked hard to make sure chart documentation was not interfering with my ability to develop rapport and engage with patients. I also thought any time saved with DAX would be erased by time that I would have to spend reviewing and editing the AI generated notes. Not so. The AI notes are concise and amazingly accurate. They are a truer representation of what actually occurred during the visit. My truncated notes, or those written or dictated hours after the visit, often missed essential information, patient perspective, or did not capture the nuanced rationale for my medical decisions.
The scribe notes are not word-for-word transcriptions. This AI has been trained using millions of hours of real-world clinical encounters and medical dictation. The program then takes recorded conversations and converts them into clinical notes, based on what it has learned about how these notes are structured.
Patients and clinicians have raised some concerns: Where does this data go? Are there privacy concerns? In fact, the data is sent securely from the clinician’s cell phone app to a Nuance company server for processing. Once a note is created, sent to, and stored permanently in the patient’s electronic health record, the data is deleted from the mobile app and servers to comply with privacy standards. Of course, your clinician should always obtain your consent before using DAX or other comparable tools.
AI scribes are a game changer — in my view, an all-around win. They free clinicians to engage more with patients in the exam room, capture a real-time, accurate synopsis of the visit, and create something cogent and readable. They help your doctor, while better honoring your medical story.
DAX was an opportunity that stood in front of me for some time before I recognized it as such. Like University of Pennsylvania Wharton School professor Adam Grant writes in his insightful book, Think Again, “anchor your sense of self in flexibility rather than consistency.” How ironic that an AI tool — algorithmic and predictable — taught me a lesson in changing my ways.
Jeffrey Millstein is an internist and regional medical director for Penn Primary and Specialty Care.
Phoenixville Hospital was not cited by the Pennsylvania Department of Health for any safety violations between August 2024 and July of this year.
The hospital, located in Phoenixville, is owned by Tower Health.
Here’s a look at the publicly available details:
Sept. 12, 2024: Inspectors followed up on two citations from May and June, and found the hospital was in compliance. In May, the hospital had been cited for discharging a patient to another facility without proper transfer orders. In June, the hospital was cited for using physical restraints on two patients without documenting that staff had first tried less restrictive ways to subdue them.
Feb. 18, 2025: Inspectors came to investigate two complaints but found the hospital was in compliance. Complaint details are not made public when inspectors determine it was unfounded.
April 17: The Joint Commission, a nonprofit hospital accreditation agency, renewed the hospital’s accreditation, effective February 2025, for 36 months.
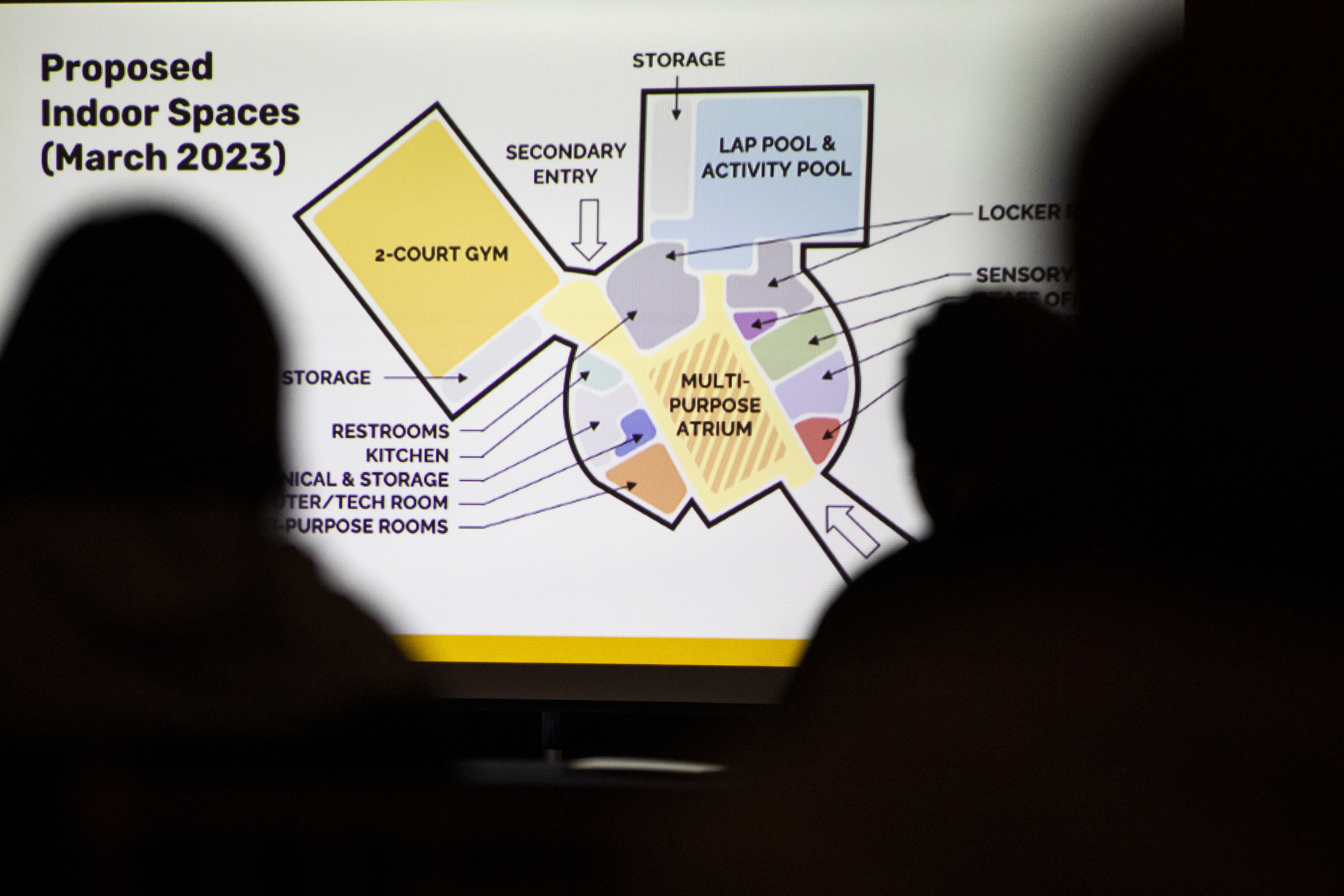
In March 2023, Kathryn Ott Lovell, then Philadelphia’s parks and recreation commissioner, announced that the plan to build a new Carousel House in West Philly was finally coming together.
The city’s only recreation center dedicated to people with disabilities had closed its doors temporarily in 2020 during the coronavirus pandemic, then permanently in 2021. City officials said years of deferred maintenance had made it unsafe.
“I’m excited to stop talking and start doing,” Ott Lovell said during the 2023 presentation at the Please Touch Museum.
The city’s disability community was also excited to reunite at Carousel House. To many, the rec center on Belmont Avenue had become like a second home, with dances, movies, swimming, arts and crafts, and summer camp.
The city’s youth wheelchair basketball team was looking forward to returning to its home base. Since the rec center closed, the squad has been practicing in New Jersey.
Two and a half years later, however, Ott Lovell has moved on to a new job, Mayor Cherelle L. Parker has replaced Jim Kenney, and the Carousel House plan is still in the design phase.
The new ribbon-cutting date: summer 2028.
“I know this is a point of pain for many people, the timeline associated with this project,” Aparna Palantino, a deputy city managing director, acknowledged at a meeting Tuesday night announcing the “relaunch” of the project.
The previous plan called for Carousel House to reopen this year.
Palantino, who heads the city’s capital program office, said the expected cost of the project had risen from $35 million to $40 million. The work will still be funded primarily with beverage-tax proceeds, but the city had to line up grants to cover the difference, as well as conduct additional environmental and structural analyses.
“The result of all that is this amazing space that will provide so many more opportunities than the former one did,” Palantino told an audience of several dozen.
Aparna Palantino, deputy managing director of Capital Program Office, speaks with attendees during the Carousel House Rebuild Community Relaunch at the Please Touch Museum on Tuesday, Oct. 21, 2025, in Philadelphia. The Carousel House project is estimated to be completed in Summer 2028.
The state-of-the-art rec center will preserve some parts of the iconic Carousel House building and include two basketball courts, a heated lap pool and an activity pool with a zero-entry sloping entrance, a computer lab, a gym, a sensory room, and other amenities.
That all sounds great to people like Mike Martin, who has used a wheelchair for the last 30 years and has been going to Carousel House since the late 1990s. Such a place is needed in Philadelphia, where an estimated 17% of residents have a disability.
But the lengthy delays in the project have Martin, 74, questioning whether he will ever see the vision become a reality.
Martin and others would have preferred for the city to fix the existing building four years ago, when rec centers were reopening after the COVID-19 shutdown. A 2021 “Save the Carousel House” protest failed to sway city leaders.
“The design is way more than I think we expected, not that we’re complaining at all,” said Martin, who serves on the Carousel House advisory committee. “We’ll see what kind of political will there is to push this through. I just don’t want to get my hopes up is what it comes down to.”
Once a model
Carousel House was considered a milestone when it opened in 1987: a city-funded rec center, specifically for people with physical and cognitive limitations, three years before the Americans with Disabilities Act would be signed into law.
The Carousel House is pictured in Philadelphia’s West Fairmount Park on Wednesday, June 2, 2021. The city said it was permanently closing the recreation center for disabled people due to the facility’s deterioration.
But in recent years, disability-rights advocates, both locally and nationally, have come to view that approach as outdated and even discriminatory. How is telling people with disabilities to go to one center, they ask, any different from designating centers for Black people, LGBTQ+ people, or other identity groups?
“People with disabilities shouldn’t have to go to one place. That’s segregation, no matter how you look at it,” Fran Fulton, the late Philadelphia disability-rights activist, told The Inquirer in 2022. “There is no doubt having people who know how to work with children and adults with different types of disabilities is an advantage. But it doesn’t have to be just Carousel House.”
Sadiki Smith (right) stands to dance as music therapist Madison Frank (left) with her guitar leads a music therapy session at Gustine Recreation Center Tuesday, November 29, 2022. Since the closing of the Carousel House, the city’s only rec center for people with physical and intellectual disabilities, many of the programs have moved to Gustine.
The city was already moving in that direction before the pandemic with its long-term Rec for All inclusion plan. The goal is to eventually make the city’s 150 rec centers accessible to all residents. The new Carousel House will be open to all people in the surrounding neighborhoods, not just those with disabilities.
That is welcome news for Lucinda Hudson, president of the Parkside Association of Philadelphia, who attended Tuesday’s meeting.
“It’s well needed, and I think the community is pleased with how it’s coming together,” Hudson said. “We need a facility to be inclusive for all, and to support the handicapped community.”
Worth the wait?
Palantino said that while the Carousel House project has faced significant delays, city officials have continued to work behind the scenes. It is the largest project in the city’s beverage-tax funded Rebuild program, which has so far committed or spent $470 million.
She believes the new building will be worth the wait.
“It will be a universal space, so an entire family can come here and enjoy the amenities. The former Carousel House was a little more restrictive in the population it served,” Palantino said in an interview. “This will be the flagship rec center in the city when it’s completed.”
Attendees look at blueprints during the Carousel House Rebuild Community Relaunch at the Please Touch Museum on Oct. 21.
Families that frequented the Carousel House, however, are running out of patience.
The Gustine Recreation Center in East Falls has continued some of the programs for people with disabilities, including music therapy, basketball, and social groups. But that center doesn’t have the space and amenities that Carousel House provided.
“It’s just not the same,” said Tamar Riley, whose 43-year-old son had been going to Carousel House since he was 12.
“Hopefully we can get this off the ground,” Riley, president of the advisory council for Carousel House, said of the plans presented this week. “It’s been a really long time. I know it’s going to be a beautiful place once the city gets it up and running.”
The closure of Carousel House also forced Katie’s Komets, Philadelphia’s team in the National Wheelchair Basketball Association, to move its weekly practices to RiverWinds Community Center in West Deptford, Gloucester County.
As a result, there is only one Philly player on the team, according to Joe Kirlin, who with his wife, Roseann, created a fund to support the team. The team is named after their late daughter.
“The problem is city kids just can’t get over there,” Joe Kirlin said.
Caroline Fitzpatrick (right), 14, of South Jersey, talks with friends during the Philadelphia Parks & Recreation’s 24th Annual Katie Kirlin Junior Wheelchair Basketball Tournament in Philadelphia on Sunday, Jan. 23, 2022. Fitzpatrick plays on Katie’s Komets team from Philadelphia.
He said wheelchair athletes in the city are missing out on potential collegeopportunities. This year, all three high school graduates on Katie’s Komets received scholarships to play college wheelchair basketball.
“That wouldn’t have happened if they didn’t start as kids playing wheelchair basketball,” Roseann Kirlin said.
Lorraine Gomez, a community activist and president of the Viola Street Residents Association in East Parkside, said after Tuesday’s meeting that she appreciated the city’s efforts to keep the surrounding neighborhoods informed about the project.
Gomez is looking forward to being able to use the indoor pool and walking track in the winter, and said people with disabilities also deserve “to have their space back.”
“This is what the community needs,” Gomez said. “It’ll be a place where we can stay in touch with each other.”
For Hudson, of the Parkside association, the most important thing now is to break ground.
“So many things get put on the books, but don’t happen,” Hudson said. “This has got to be built.”
Villanova professor Ana Santos Rutschman would describe the current state of vaccine policy as a game of chess.
When the federal government does something, some states — primarily Democratic-led states including Pennsylvania—respond immediately to counter.
A prime example followed the federal government’s move, through the Food and Drug Administration, in August to limit eligibility for the updated COVID-19 vaccine. Previously, the annual shot was recommended for all Americans 6 months and older. The new guidance was for people 65 or older and those at high risk of complications from COVID-19.
Pennsylvania’s regulatory body for pharmacists opened up access by allowing pharmacists to follow the broader recommendations of professional medical societies.
“It’s kind of [like] ‘Harry Potter’ chess. Remember when they climb on the gigantic pieces and then try to kill one another?” Rutschman said, referring to the fictional scene where chess pieces violently smash the opposing side’s pieces.
“There’s a certain violence to this from a political perspective,” she added.
States are allowed to diverge from the federal government on vaccine policy because our system of government, known as federalism, divides power between the federal government and the states.
With vaccines, states historicallyhave chosen to align in large part with the federal government’s recommendations.
Rutschman says recent actions byHealth and Human Services Secretary Robert F. Kennedy Jr. have ushered in a new era of what’s being called “vaccine federalism.” Kennedy is a longtime anti-vaccine activist now serving as President Donald Trump’s top health official.
Many states, especially those with Democratic governors, including Pennsylvania and New Jersey, saw recent changes under his leadership as a sign that they “need to do something in direct opposition to the federal government,” Rutschman said.
Now it’s a “head-on collision,” she added.
The Inquirer spoke with Rutschman, who researches vaccine federalism as a health law professor and director of the Health Innovation Lab at Villanova University, to learn more about this new era and its possible consequences in a conversation lightly edited for length and clarity.
What is vaccine federalism?
For vaccination and everything else, our system is split in two. You have the states and then you have the federal government.
There is room for tension between the federal level and the state level. Historically, that tension has been, I would argue, limited. It has existed, but it’s not been the defining feature. Now, particularly in the context of vaccines, it has become probably the most salient feature.
How are states allowed to differ from the federal government as far as vaccine policy?
States don’t have the power to authorize a new vaccine to come to market.
But then you have a lot of things that the Centers for Disease Control have done that are more informational. The federal government recommends which shots children or adults should get, and the time frame for most children to get these shots.
The federal government offers this kind of informational support, and then states set their own policy.
How has vaccine federalism played out in the past?
Examples from the past are not as salient or blatant as the ones you’re seeing right now.
There was a lot of variability around the country, but the overall message was harmonious. Everybody was trying to get, by and large, most of the population vaccinated past herd immunity.
What is happening now?
Now it’s a head-on collision.
States are saying, ‘We’re not going to implement requirements to restrict access to these vaccines.’ The Board of Pharmacy in Pennsylvania decided not to be bound by the CDC’s recommendations. This is a direct clash. We hadn’t had this before between the federal government and the states in the field of vaccines.
What are examples of this new era of vaccine federalism?
One example would be the formation of state clusters. These are a lot of neighboring states in agreement. They’re trying to share data and think of best practices, which is almost that informational function that traditionally fell to the [federal health agencies].
The states are saying, ‘Well, you’re not doing that, so we will.’
‘We will pull resources and information to come up with our own advisory role.’ That’s unprecedented.
You have sort of two speeds in the country. Some states are collaborating and very active in setting regional vaccine policy. And then you have a bunch of states that go completely the other way. You have the, for now, isolated case of Florida saying, ‘We’re going to just basically do away with all vaccination mandates,’ which is going further than the federal government.
Now it’s a much messier situation, legally, philosophically, politically, etc.
They are accomplishing something. You see fewer restrictions in access to vaccines in a place like Pennsylvania than other states.
Whereas states who are not part of these kinds of coalitions — typically excluding the likes of Florida — a lot of them are waiting to see what happens, because this has never happened in the history of vaccination in the United States.
In the meantime, there are a lot of people falling through the cracks who would have been indicated for a vaccine last year. Now they’re wondering what to do, and their providers are not entirely sure.
There’s a lot of confusion about what happens now that federal policy has taken a completely different direction.
What impacts do you see coming from this new era of vaccine federalism?
People hearing one thing out of the CDC and another one out of the state of Pennsylvania may think, ‘Who’s correct? Who should I listen to?’ You start aggregating all the people who might forgo vaccination just because they don’t understand what’s going on.
I think it continues to accelerate the overall phenomenon of vaccine mistrust, and we’re already seeing levels of herd immunity come down for many vaccine-preventable diseases.
If I were a provider, I would be similarly confused and concerned, because nobody takes lightly the idea that from now on, ‘I’ll be doing something that’s in direct opposition to what the federal regulators are suggesting I should be doing.’ So I think there’s a fear factor and confusion.
Lastly, I think there’s an overall chilling effect with regard to vaccines. Yes, some vaccines make money, but they don’t make a whole lot of money to begin with. They’ve never been one of the preferred products for manufacturers. These are not the most profitable things they can be doing.
I think that we will see much less focus on vaccine development in years to come, because that’s the logical position for pharmaceutical companies, and for some funders even to take, which is unfortunate.
What do you think of Pennsylvania’s response?
I think it’s to Pennsylvania’s credit, and I think it’s to some degree reassuring for Pennsylvanians. Although it obviously makes me sad that we have sort of this two-speed mode in the country. Some part of this national fabric has ruptured.
For now, Pennsylvania has protected itself as it can, but states alone don’t control everything. You have Pennsylvanians going to other states where you may have an outbreak of a vaccine-preventable disease. We don’t have real borders. We cross them all the time.
Millions of Americans are already seeing their health insurance costs soar for 2026 as Congress remains deadlocked over extending covid-era subsidies for premiums.
The bitter fight sparked a government shutdown at the start of October. Democrats refuse to vote on government-funding legislation unless it extends the subsidies, while Republicans insist on separate negotiations after reopening the government. Now lawmakers face greater pressure to act as Americans who buy insurance through the Affordable Care Act are seeing, or about to see, the consequences of enhanced subsidies expiring at the end of the year.
Healthcare.gov — the federal website used by 28 states — is expected to post plan offerings early next week ahead of the start of open enrollment in November. But window shopping has already begun in most of the 22 states that run their own marketplaces, offering a preview of the sticker shock to come.
Premiums nationwide are set to rise by 18 percent on average, according to an analysis of preliminary rate filings by the nonpartisan health policy group KFF. That, combined with the loss of extra subsidies, have left Americans with the worst year-over-year price hikes in the 12 years since the marketplaces launched.
Nationally, the average marketplace consumer will pay $1,904 in annual premiums next year, up from $888 in 2025, according to KFF.
The situation is particularly acute in Georgia, which recorded the second-highest enrollment of any state-run marketplace this year and posted prices for 2026 earlier in October. About 96 percent of marketplace enrollees in Georgia received subsidies this year, according to the Center on Budget and Policy Priorities, a liberal think tank that supports extending the subsidies.
Now Georgians browsing the state website are seeing estimated monthly costs double or even triple, depending on their incomes, as lower subsidy thresholds resume.
“We have people saying they will have to choose between their monthly premiums and mortgage,” said Natasha Taylor, deputy director of Georgia Watch, a consumer advocacy group.
For example, a family of four earning $82,000 a year in Georgia could see their annual premium double to around $7,000 for a plan with midrange coverage, according to a CBPP analysis. If that family earned at least $130,000, they would have to pay the full cost of the annual premium, about $24,000 instead of $11,000.
It’s a similar story in other states, where people in higher income tiers will see especially big premium increases as they become ineligible for subsidies. A 60-year-old couple earning $85,000 may have to pay $31,000 for a plan in Kentucky, $28,000 for a plan in Oregon and $44,000 for a plan in Vermont, according to CBPP.
If Congress doesn’t extend the extra subsidies, Georgia could lose around 340,000 people from its 1.5 million-person marketplace, according to an estimate by nonpartisan advocacy group Georgians for a Healthy Future.
The enhanced subsidies had fully covered monthly premiums for millions of lower-income people in the marketplaces. Many of them will have to start kicking in some of their own money starting Jan. 1, while people with higher incomes will see their monthly subsidies shrink. People earning more than 400 percent of the federal poverty line will no longer be eligible for subsidies at all.
The political fallout in Georgia has already begun to reverberate. Rep. Marjorie Taylor Greene (R-Georgia) broke with her party to demand an extension of subsidies, noting her adult children’s premiums are set to double. Greene’s office didn’t respond to a request for comment.
Sen. Jon Ossoff, considered the most vulnerable Democratic incumbent in next year’s midterms, has seized on the issue of rising premiums. An Ossoff spokesman said the senator wants the subsidies extended, pointing to polling showing a majority of Georgians feel the same.
Republican Gov. Brian Kemp, who championed the state’s marketplace, didn’t respond to a request for comment.
Atlanta resident Jody Fieulleteau, 31, said she has been paying $160 a month for a subsidized plan on Georgia’s marketplace. She makes about $40,000 a year styling hair and providing behavioral therapy. She has yet to complete an application to see quotes for plans next year, but her monthly premium is likely to nearly double based on her age, income and Zip code.
Fieulleteau said she rushed to schedule a surgery next week for a problem related to menstruation because she’s concerned about having insurance.
“I’m feeling like I need to get everything done this year because I don’t know what next year is going to look like,” she said in a phone interview.
Taylor, of Georgia Watch, said she finds that consumers often don’t understand that their plans are subsidized, which makes it difficult to explain that the pricey plans they see now could become cheaper if Congress votes to extend the subsidies.
“For your average consumer, they look at the bottom line. What’s my out-of-pocket max,” Taylor said. “I don’t think they’re looking at the minutiae of why their premium is what it is.”
The rising insurance costshighlight the political difficulties faced by Washington lawmakers.
The Congressional Budget Office, the legislature’s nonpartisan bookkeeper, has estimated nearly 4 million fewer people will have marketplace plans a decade from now if the extra subsidies expire.
Republicans say the premium assistance — intended to help people be insuredduring the coronavirus pandemic — are just a Band-Aid for a failure of the Affordable Care Act to rein in the costs of plans. They also say the subsidies were so generous they incentivized fraud, pointing to a CBO estimate that 2.3 million enrollees improperly claimed a subsidy this year.
But 13 House Republicans who face competitive reelection campaigns next year wrote to House Speaker Mike Johnson (R-Louisiana)on Tuesday asking him to consider extending premium assistance.
“Millions of Americans are facing drastic premium increases due to shortsighted Democratic policymaking,” they wrote. “While we did not create this crisis, we now have both the responsibility and the opportunity to address it.”
Sen. Patty Murray (D-Washington) said in a news conference that she heard from families whose premiums are doubling as window shopping started in her state Tuesday. She said she heard similar stories from Idaho and Montana, noting most people who rely on premium assistance live in red states.
“Families are logging on, looking for health coverage for next year, and coming face to face with massive price hikes because Republicans downright refuse to work with us to do something about it,” Murray said.
Insurers have partially blamed the premium hikes on the expiration of the subsidies, saying they’ll cause healthy people to drop coverage, leaving a sicker, more expensive pool of customersbehind. Insurers have also cited higher drug and hospital prices, expensive weight-loss drugs and medical inflation as reasons for raising premiums.
But if Congress acts to extend the subsidies, even after open enrollment begins Nov. 1, some plans may be willing to lower premiums, said David Merritt, senior vice president of external affairs at the Blue Cross Blue Shield Association, whose memberplans are sold in all marketplaces. Adjusting rates lower would get more complicated after Dec. 31, he said.
Even if Congress does extend the subsidies, consumer advocates saydamage has already been done.
Many people will visit theinsurance marketplaces and decide to forgo coverage after seeing pricey 2026 plans, they said, and not revisit their decision even if subsidies are restored.
Amid persistently higher costs, three Philadelphia-area health systems have cut expenses over the last two years by changing how they account for investments in facilities and equipment. The change significantly boosted operating income in all three cases.
ChristianaCare and Main Line Health are now spreading the cost of buildings and building improvements over as many as 80 years, they said in their fiscal 2025 audited financial statements. That is double the maximum number of years they previously used to calculate what accountants call depreciation expense. Thomas Jefferson University made a similar change last year.
All three health systems use PricewaterhouseCoopers LLP as their auditor. The firm, which did not respond to a request for comment, also has Philadelphia health-system clients that have not extended their depreciation schedules.
The term depreciation expense refers to the way hospitals and other businesses allocate the cost of a building, a piece of equipment such as an MRI machine, or even software to manage patient records across the number of years the asset is likely to be used.
It’s a noncash expense because the money used to make the purchase is recorded elsewhere in the financial statements. Several financial and accounting experts said the change could be seen as cosmetic.
“It’s not affecting operations. It’s not increasing their revenues. It’s not decreasing their cash expenditures. It is purely a bookkeeping entry,” said Steven Balsam, a professor of accounting at Temple University’s Fox School of Business.
Main Line Health
At Main Line, the extended depreciation schedule reduced the expense by an estimated $37.5 million. That helped the system achieve a small, $4 million operating profit for the first time since fiscal 2021, when federal COVID-19 aid buoyed hospitals.
Without the depreciation savings, Main Line would have had an operating loss of $33.5 million in the year that ended June 30, compared to a $61 million operating loss in fiscal 2024.
Asked for comment, Main Line’s chief financial officer Leigh Ehrlich noted that the system’s financial performance had improved, thanks to “increased patient volumes and continued focus on expense management.”
Excluding noncash depreciation and amortization in each of the last two years, Main Line’s operating income improved to $127.8 million from $96.7 million.
ChristianaCare
ChristianaCare reviewed the depreciation schedules of fixed assets “as part of our ongoing commitment to maintain accurate and reliable financial reporting,” the nonprofit’s chief financial officer Rob McMurray said in an email. The result was a $24.4 million reduction in depreciation expense.
The review also resulted in a $9 million write-off of unspecified assets, which meant that in fiscal 2025 the benefit to operating income was $15 million, McMurray said.
ChristianaCare’s operating income in the year that ended June 30 was $35.5 million, or $20.5 million without the accounting change. The organization had $126.2 million in operating income in fiscal 2024.
Thomas Jefferson University
Last year, Thomas Jefferson University opened its $762 million Honickman Center in Philadelphia. Normally, taking a building like that into service would increase depreciation expense.
Instead, Jefferson’s depreciation expense fell by $68 million, according to its audited financial statement for the year that ended June 30, 2024. The decline happened after Jefferson opted to spread the cost of all buildings and building improvements over as many as 70 years, according to the depreciation schedule in its financial statement.
Even with the depreciation change, Jefferson’s operating income in fiscal 2024 was extremely narrow, at $1.34 million on nearly $10 billion in revenue that year.
The benefit of lower depreciation expense continued in fiscal 2025, as it will in future years for ChristianaCare and Main Line.
Depreciation expense at other local systems
Most Philadelphia-area health systems use a schedule for depreciating buildings and building improvements that maxes out at 40 years, an Inquirer review of financial statements found.
“You’re constantly modernizing your facilities to allow for the delivery of medicine based on current times,” Temple University Health System chief financial officer Jerry Oetzel said in an interview. “Who knows 15 years from now? We don’t have clear insight, but it’s probably going to be more home care.”
That’s why Temple hasn’t adopted a longer depreciation schedule. “It’s just a savings in operating expenses without the benefit of any cash behind it,” Oetzel said.
Editor’s note: This article has been updated to remove a reference to American Hospital Association guidelines.
The Children’s Hospital of Philadelphia called new evidence presented by President Donald Trump’s administration weak and untrustworthy in a blistering legal response to federal efforts to investigate its doctors providing gender-affirming care.
CHOP’s response, filed late Monday in federal court in Philadelphia, came in defense of accusations by the U.S. Department of Justice that it’s investigating “fraudulent billing practices“ at the hospital.Federal officials say they’re looking into whether CHOP doctors were fudging or lying about diagnoses to get private and public health insurance companies to cover off-label drug prescriptions used to treat patients with gender dysphoria — a medical condition in which a person’s body does not match their gender identity.
In its filing, CHOP lawyers called the DOJ’s allegations “unreliable,” and urged U.S. District Court Judge Mark A. Kearney to disregard claims that are “threadbare, of dubious origin, and so heavily qualified and caveated as to offer the court no meaningful information.”
CHOP and the DOJ are locked in a legal battle over a sweeping federal subpoena sent to the hospital in June. The subpoena seeks patient names, Social Security numbers, addresses, diagnoses, and treatment notes, in addition to doctor emails and encrypted text messages.
In July, CHOP filed a motion to limit the scope of the subpoena to protect patient privacy. Judge Kearney is now weighing CHOP’s motion.
In the latest filing, CHOP’s lawyers argued the DOJ’s “new evidence” against the hospital was unfairly “shoehorned” into a separate but related case filed last month by a group of CHOP patients and their families who also want Kearney to block the release of private medical records to the DOJ.
“That new evidence should not be considered because it is not before the Court in this case and is unreliable in any event,” CHOP lawyers wrote in the filing. “The government (still) cannot establish that its need for extraordinarily sensitive and personal patient information outweighs the highest-order privacy interests on the other side of the ledger.”
The DOJ did not immediately respond Tuesday to a request for comment.
Feds seek patient information from CHOP
In April, U.S. Attorney General Pam Bondi issued a memo, entitled “Preventing the Mutilation of American Children,” in which she tasked the DOJ with enforcing measures targeting gender-affirming care for youth.
About two months later, the DOJ sent subpoenas to CHOP and at least 19 other hospitals nationally that are under scrutiny for treating transgender youth. The subpoenas sparked legal opposition playing out in federal courts in Pennsylvania and across the nation.
The DOJ’skey focus is how doctors are prescribing puberty blockers and hormones “off-label,” meaning for a condition not specifically approved by the U.S. Food and Drug Administration.
Once a drug is approved by the FDA, it is legal for doctors to prescribe it to treat other conditions that could benefit from the medication. Off-label prescribing is a common and widely accepted medical practice, especially in pediatrics.
Gender-affirming care for children and adolescents has been deemed medically appropriate by the American Academy of Pediatrics and other major medical and mental health organizations. Research shows young people with gender dysphoria suffer higher rates of suicide, self-harm, depression, and anxiety.
CHOP’s Gender and Sexuality Development Program, created in 2014, is one of the nation’s largest such clinics and provides medical care and mental health support to hundreds of new families each year.
CHOP’s legal fight for patient privacy
Late last month, families and patients joined in CHOP’s fight against the federal subpoena by filing a separate motion to protect their privacy rights. That motion was filed on behalf of five parents with transgender children and one adult who received care at CHOP.
In response to that case, the DOJ filed a “Declaration,” or sworn statement, from Lisa Hsiao, acting director of the DOJ’s Enforcement and Affirmative Litigation Branch, formerly known as the Consumer Protection Branch. In it, Hsiao said the government has new evidence “particular to CHOP that raises concern that federal healthcare offenses may be occurring there.”
Hsiao said the government analyzed CHOP’sinsurance claims and found that between 2017 and 2024, CHOP providers diagnosed 250 minors with central precocious puberty at age 10 or older, “including numerous teenagers aged 14 to 18.”
“This is well beyond the age at which children are typically diagnosed with precocious puberty,” Hsiao stated. The government, she said, suspects doctors are improperly using the precocious puberty diagnosis to get insurance coverage for treatment of gender dysphoria.
In Monday’s court filing, CHOP lawyers accused the DOJ of attempting to “shoehorn its new evidence into CHOP’s case” through the other case.
CHOP also argued Hsiao’s declaration provides nothing to support its contentions surrounding precocious puberty diagnosis.
“Moreover, the government fails to contextualize the findings of its rudimentary analysis, offering no comparator for the use of the code for precocious puberty at peer hospitals, let alone hospitals that, like CHOP, have providers who specialize in treating endocrine disorders,” CHOP lawyers wrote.
The source of “the data set is entirely unknown,” CHOP’s lawyers noted, addingthe declaration never says how many patients were treated for gender dysphoria during that time frame.
The CHOP lawyers also criticized Hsiao for writing in her sworn declaration that the government was aware of a lawsuit filed against CHOP that alleges doctors hastily prescribed puberty blockers and hormones to a minor who later regretted it.
Hsiao later refiled the declaration to remove any reference to a lawsuit after learning that it hadn’t been filed.
CHOP lawyers wrote they believe the lawsuit reference came from a news article about a former CHOP patient. The article said the patient “was suing the hospital.” However, CHOP was unaware of any such lawsuit.
“The similarities between the report and the allegations in the Hsiao Declaration — including the reference to a lawsuit — raise suspicions that, in looking to justify its investigative interest in CHOP, the government simply searched the internet for stories fitting its narrative and presented the one it found as fact without adequately scrutinizing its veracity.”