Most of us have heard the adage “Feed a cold, starve a fever.”
It comes from an outdated theory that a cold makes your body cooler and eating can help warm it up, and that a fever makes your body warmer and fasting can help cool it down. The premise itself is flawed: While fevers do raise your body temperature, colds don’t make your body cold. You might even get a fever when you have a cold.
As for whether you should eat more or less, in most cases, there’s no convincing evidence thatlimiting food intake when you’re sick plays a meaningful role in recovery, experts said.
There may be a more accurate approach. “Feed a cold. Feed a fever, too,” said Roy Gulick, the chief of the infectious-disease division at Weill Cornell Medicine and an attending physician at New York-Presbyterian Hospital.
Experts recommend staying hydrated and eating healthy foods — at least when your stomach will allow it — to support your body when you’re sick. The advice holds true whether you’re dealing with a cold, which is an upper-respiratory infection that can be caused by more than 200 viruses, or a fever, which can be caused by viral and bacterial infections, autoimmune issues, and reactions to medications, among other things.
“If you are truly not feeling hungry, you don’t necessarily have to eat more than you feel like eating,” said Geeta Sood, an assistant professor in the infectious-disease division at Johns Hopkins University.However, you do want to make sure you’re getting enough calories, protein, and nutrients — and hydration — to help support your body as it heals, she said.
What does the research show?
Research in this area is limited — and mostly in animals. For example, in a 2016 study, mice were infected with either a bacterium that causes gastrointestinal illness or a virus that causes influenza. In mice with the bacterial infection, fasting was protective while nutritional supplementation was detrimental, the authors found. The pattern was reversed in mice with the flu and viral sepsis.While interesting fodder for further research, these results can’t be applied directly to humans, experts said.
In humans, researchers who conducted a 2021 review concluded that there is some evidence that nutrients such as vitamins and minerals can help support the body’s immune response and help fight infections in general. And a 2024 review that included newer studies that were conducted duringthe pandemic suggested that nutritional needs may depend on the specific pathogen you’re fighting and other variables, such as the duration and severity of your illness — not simply on whether it’s a bacterium or virus.
The reality is that most studies on how nutrition affects infections have looked at only a handful of pathogens, said David Schneider, a professor of microbiology and immunology at Stanford University. To further complicate matters, when you’re experiencing symptoms such as a runny nose or fever, you may not know whether you’re sick with a bacterium or virus, he said. Both of these things make it difficult to give generalized recommendations about what might be best for every cold or every fever, he said.
Why do I lose my appetite when I’m sick?
There is some rationale to the adage, because it’s common to lose your appetite when yourbody is fighting off an infection. As your immune system ramps up, it releases chemical messengers, known as cytokines, to rally immune cells to fight infection, and those same signals also tell the brain that eating isn’t a priority, said Sharon Bergquist, an internal medicine physician and associate professor at the Emory University School of Medicine.
While not well understood, one theory states that a drop in calorie and protein intake triggers a process called autophagy, which helps recycle damaged cell parts and may play a role in immune defense, she said.
That said, the process of fighting an infection is “metabolically really costly,” Bergquist said, explaining that although you can skip food for a day if you aren’t hungry, going longer than that may leave you without adequate nutrition. “It takes so much energy and calories that there’s a rationale for us needing to increase our food and our hydration during times of illness so that we can support our immune system,” she said.
What can I do if I have an infection?
Vaccines are the first-line defense to help prevent and lessen the severity of some viral infections, including COVIDand the flu. If you get sick, however, you can try some medications that may help you recover faster.
Antibiotics target specific kinds of bacteria such as those that cause strep throat, pneumonia, or urinary tract infections.
Antiviral medications can help treat certain viral infections, including the coronavirus and influenza. Three antivirals — Paxlovid, remdesivir, and molnupiravir — are available by prescription to treat COVID in people who are at high risk of serious complications, and four antivirals are approved to treat the flu.
There are also a few other things you can do to help support your body.
Stay hydrated. Losing water and electrolytes through sweat when you have a fever, as well as through diarrhea and vomiting, can put you at risk for dehydration, so it’s important to drink plenty of water and make sure you’re getting enough electrolytes, Gulick said. Pediatric beverages and sports drinks with added sodium and potassium can help you stay hydrated, and warm liquids such as soups, broths, and caffeine-free herbal teas can help ease symptoms such as congestion, body aches, and chills, Sood said. Avoid alcohol and caffeinated drinks because they are diuretics and can make dehydration worse.
Eat, when possible. Listen to your body, but when you have an appetite, eat healthy, whole foods rich in vitamins, minerals, and antioxidants such as fresh fruits and vegetables. One strategy is to make smoothies or soups, Bergquist said. Avoid foods high in saturated fats and processed carbohydrates.
Get rest. Take time to rest as your body does much of its repair work while you sleep, Bergquist said. “Don’t push your body because you want to dedicate that energy to your immune system,” she said.
Take hot showers or baths. The steam can help break up congestion and clear airways.
Try zinc. Zinc may help shorten a cold by a day or two. In a 2024 review, researchers found some evidence that zinc might reduce the duration of symptoms by about two days compared with a placebo, though the mineral was associated with mild side effects such as nasal and oral irritation, problems with taste, stomach pain, constipation, diarrhea, and vomiting. Most other supplements have no real advantage for colds, including vitamin C, which, when started at the onset of symptoms, doesn’t help lessen the duration or severity, research shows.
Use honey for a cough or sore throat. Adults and children older than 1 year can add honey to warm tea or water to help soothe sore throats and calm coughs.
When Kelly McBride read Elizabeth Bruenig’s essay in the Atlantic about a child’s death from measles complications, she was moved and quickly shared the story on her Facebook account. She hadn’t realized that Bruenig’s family had been ravaged by virus and the well-known journalist had lost a child.
McBride, a media ethicist and senior vice president at the Poynter Institute, also didn’t realize the story was a hypothetical scenario — and the child a composite character based on the author’s research — until a friend alerted her to an editor’s note at the bottom of the story. Then, McBride felt duped.
“I feel deceived,” McBride said. “I spent all weekend talking about this story to my friends as if the reporter had experienced it.”
Bruenig’s stirring account of a mother’s experience learning her child will die of the long-term effects of measles has remained one of the Atlantic’s most read stories since it was published Thursday, receiving more than 700 comments. Written in the second person, some readers have called the essay a visceral and gut-wrenching exposéof the human impacts of the measles epidemic.
It has also generated controversy. Readers and media experts have condemned the story as breeching journalistic ethics by informing the reader that the story is fictionalized through a short editor’s note at the end of the 3,000-word essay. Some public health experts argued the story was a dangerous writing exercise that could evoke backlash and confusion as vaccine skepticism hits an all-time high across the country.
“Grateful to @ebruenig for sharing her and her family’s ordeal,” Gabby Stern, a former World Health Organization communications director, wrote on X shortly after the story published. “Friends, please ensure that your children receive vaccinations against preventable diseases like measles.”
She followed up soon after: “I missed the disclaimer at the bottom. Others did, too. You get to the end and you’re shattered, not looking for caveats and fine print. Disappointed in the magazine. The topic is too high-stakes for such shenanigans.”
Adrienne LaFrance, executive editor at the Atlantic, told The Washington Post in a statement that the magazine was “pleased that so many people are reading and praising Liz’s remarkable essay.”
“We trust our readers to understand all different kinds of writing and writerly devices,” she said. “And while we included a note about Liz’s methods for transparency’s sake, we’re finding that most readers already understand the second-person well enough to know that the ‘you’ referenced throughout the piece is not literally ‘you,’ the reader.”
The Atlantic, one of the most popular American magazines with 1.4 million subscribers, has become a destination for health reporting in recent years. The Atlantic is among a cohort of outlets that have reported on rising measles cases across the United States, as well as the role that misinformation and shifting government guidelines have on childhood vaccinations. Once eliminated in the country, outbreaks have led to the highest count of measles cases in more than three decades. Atlantic staff writer Tom Bartlett was first to find and interview the parents of a child who died of measles in Texas, the first such death in a decade.
Bruenig, a former Post opinion writer, has twice been a finalist for the Pulitzer Prize for feature writing, one of the industry’s top honors for narrative journalism. (This reporter worked for the Atlantic from 2017 to 2019.)
Bruenig wrote the essay in the second person, detailing a scenario where two unvaccinated children attend a birthday party and catch measles from an infected-but-asymptomatic child. “Your daughter behaves normally over the next week while the virus slowly spreads inside her, infecting immune cells that carry it to the lymph nodes, where it replicates and spreads at a rapid pace.”
It includes a short disclaimer at the bottom of the 3,000-word piece: “This story is based on extensive reporting and interviews with physicians, including those who have cared directly for patients with measles.”
Reported hypotheticals have been used in other grim chronicles such as Outside Magazine’s 1997 story “Frozen Alive,” about freezing to death; a passage of Kathryn Schulz’s 2015 New Yorker essay “The Really Big One” about the risks of a large earthquake; and the 2024 Annie Jacobsen book “Nuclear War: A Scenario,” about how nuclear warfare could transpire. The first two stories also are written in second person.
Many readers, including physicians, praised the Atlantic essay, writing that its evocative writing and storytelling forced readers to grapple with the impact of vaccine hesitancy. “Read this while holding my almost-one-month-old, and it absolutely wrecked me. What a powerful and important piece,” one commenter wrote. “Tragically realistic story exquisitely described by Ms. Breunig,” wrote another. “I’m a pediatrician who has never seen a case of measles but am awaiting my first one.”
Others, however, expressed their confusion in the essay’s comments. “The fact that readers in the discussion are unsure of whether this is a true story or fiction highlights a fundamental failure on the part of the author, and the editor,” one reader wrote.
“I know the internet is full of made up stuff, but I trusted the Atlantic,” another reader wrote. “I feel foolish that I told my husband about this as if it were the truth. Glad I didn’t share it with my sisters. We are all pro vaccines, and I’m concerned this story masquerading as a first person memoir will encourage people on the edge to blow off vaccines.”
Tom Rosenstiel, a professor at University of Maryland’s Philip Merrill College of Journalism and former executive director of the American Press Institute, felt the piece did the reader a disservice by not being fully transparent about they were about to read. He said the Atlantic needed to clearly explain the unusual choices in the story upfront, avoiding deception.
“Any time you’re answering questions about why you did something in the story after you’ve published it, you’re in a bad place,” he said.
Some physicians argued the uncertainty around the essay could fan distrust of vaccines. Angela Rasmussen, a virologist at the University of Saskatchewan who edits the journal “Vaccine,” said she found the essay scientifically sound but extremely confusing. She initially believed the essay was about Bruenig’s real child and felt the essay could backfire. “We need effective communicators like this,” she said. “But if that effective communication is being presented in such a way that it actually diminishes trust further, then we’re in real trouble.”
Rachael Bedard, a physician and writer, called herself an admirer of Bruenig, but expressed similar concerns in a series of posts on X.
“One of the things that people who have actually interacted [with] anti-vaxxers know is that they often think the liberal media is lying to them about how bad measles is,” she wrote, writing that the Atlantic’s presentation of this essay as anything other than fiction “affirms all of those concerns.”
Bruenig, in an interview with the website Nieman Lab, defended the structure of her essay. “It is a hypothetical account of a very real phenomenon based on careful reporting,” she said. “I would place it somewhere on the creative nonfiction spectrum.” She said that she interviewed doctors for her piece, and based the character of the mother on herself.
“I have no doubt that there are a lot of people out there who are unhappy with the story or reject its premises, and they are entitled to their interpretations. I get it,” she said. “But my job is to report the truth about the world — and I use all kinds of literary, and narrative devices to do that. I do it because telling the truth is important in its own right, whether or not anyone finds it persuasive.”
Johnson & Johnson plans to spend more than $1 billion to build a cell therapy manufacturing facility in Montgomery County near Spring House, the New Jersey pharmaceutical and medical supplies giant said Wednesday.
The Lower Gwynedd Township plant, part of an effort by the company to invest $55 million in the U.S. by early 2029, is expected to employ 500 people when fully operational in 2031, J&J said.
The facility at 1201 Sumneytown Pike will add to J&J’s capacity to make cell therapy treatments for cancer, with a focus on multiple myeloma. That’s a type of cancer that attacks white blood cells in the bone marrow. Cell therapy is the use of engineered immune cells to treat disease.
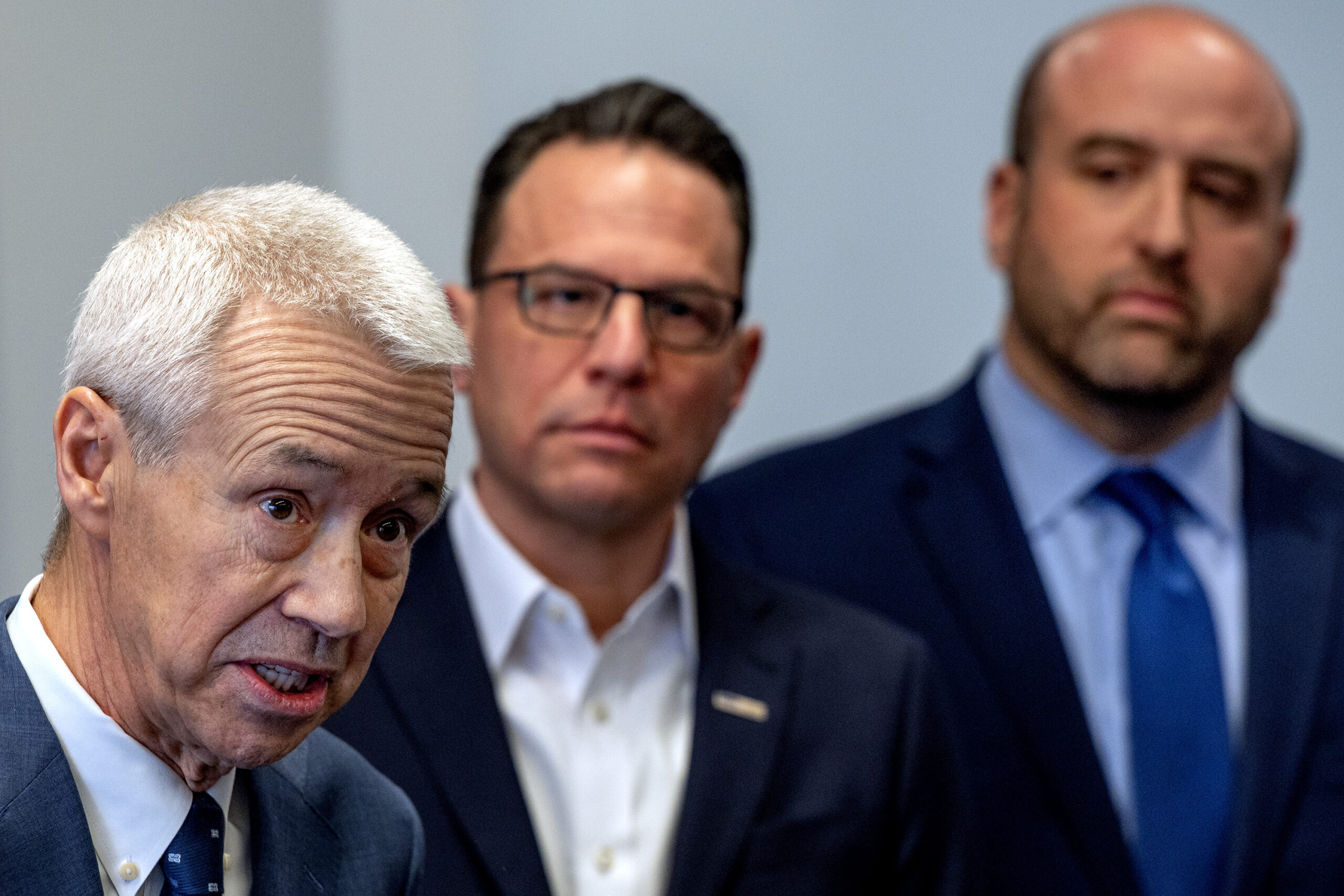
“Pennsylvania’s proud manufacturing legacy, from steel to today’s medicines and medical technologies and Johnson & Johnson’s roots here for seven decades, are part of why we are investing here.” Joaquin Duato, J&J’s chairman and CEO, said.
Duato spoke during an event at the company’s Spring House research and development campus, where 2,500 scientists work in 70 laboratories. The Montgomery County site is J&J’s largest R&D center and it’s “where most of our discovery efforts start,” Duato said.
The company based in New Brunswick, N.J., employs 5,885 people at 10 Pennsylvania facilities, according to the office of Gov. Josh Shapiro. The Shapiro administration has offered $41.5 million in state support for the J&J project.
“With this investment, we are further cementing our place as a leader in life sciences,” Shapiro said. He said his administration’s efforts to cut red tape are among the reasons companies like J&J “are choosing to double down on their investments” in Pennsylvania.
Eli Lilly & Co. last month announced plans to build a $3.5 billion pharmaceutical plant in the Lehigh Valley to expand manufacturing capacity for next-generation injectable weight-loss medicines.
GSK said in September that it will build a biologics factory in Upper Merion Township, but did not specify how much it would spend there. That project is part of GSK’s plan to spend $1.2 billion on advanced manufacturing facilities.
Johnson & Johnson chairman and CEO Joaquin Duato (left), was joined by Gov. Josh Shapiro and Pa. Dept. of Community and Economic Development Secretary Rick Siger (right) on Wednesday when J&J announced it will spend $1 billion on a cell therapy plant on its campus in Lower Gwynedd Township.
Merck, another New Jersey-based drug giant, last year announced plans for a $1 billion factory and lab near Wilmington. Merck also has major operations in Montgomery County, which is among the top-ranked counties nationally for pharmaceutical manufacturing jobs.
J&J has a long legacy in the Philadelphia region. Among its major acquisitions here was the 1959 purchase of McNeil Laboratories, which later developed Tylenol. The pain reliever is still made at a plant in Fort Washington.
Other major Philadelphia-area J&J deals include the 1999 purchase of Centocor, one of the country’s first biotech companies, and the 2012 deal for Synthes Inc., a Swiss medical device maker with its North American headquarters and major operations here.
Separately from the new cell therapy manufacturing facility, J&J has two expansion projects planned for the Spring House R&D site.
One is a new cell engineering and analytical sciences facility. The other is focused on CAR-T testing and manufacturing during research and development, with the goal of creating personalized therapies more quickly and efficiently. The company did not disclose the cost of those projects.
A millionaire’s private island filled with luxury goods, gourmet food, and fine wine seems like a reality a million miles from yours, so what can Philadelphia-area parents learn from the Epstein files?
Plenty.
There are people like Jeffrey Epstein everywhere. He just had a bigger field.
Epstein started small. In her memoir Nobody’s Girl, the late Virginia Roberts Giuffre, abused and trafficked by Epstein starting at age 16, describes how Epstein told her that as a teacher, he traded sex for grades. Alumni of New York’s elite Dalton School have described inappropriate conduct toward girls. Yet he was dismissed from the school simply for “poor performance.”
Back in the 1970s, when Epstein taught, sex abuse prevention programs were primarily directed at kids. Teaching kids to recognize “good touch/bad touch” would have done nothing for teenage girls, likely targeted for their insecurity, for whom attention from a cute, popular new teacher felt like affection and status. Today, the most effective school-based sex abuse prevention programs involve the entire school helping faculty and staff recognize and respond to inappropriate behavior. Policies explicitly identify acceptable and unacceptable behaviors around issues from touching to communicating with students outside of school. Ongoing prevention programs empower everyone to act if they see a breach. Parents are included as partners to reinforce healthy messages at home. One great example is Safety STARS — Enough Abuse.
What are the lessons for parents? I can count at least four:
1. Learn what sexual abuse prevention program is offered in your school or district and participate in the parent component. Confirm that it follows best practices, such as requiring a code of conduct for faculty, staff, and students, and commitment from administration to continuous monitoring of adherence to the policies.
Almost 20 years ago, Epstein was convicted of trafficking children for sex but escaped serious punishment in a now widely criticized plea deal. Defense attorneys at the time used the phrase “underage women” to soften how his acts against children sounded. I urge parents and all adults to more accurately call his crimes “child rape.” This helps challenge the social norm that it is somehow acceptable to have sex with minors who may be dressed up to appear older than they truly are.
2. For decades, social scientists have distinguished a pedophile — someone primarily attracted to prepubescent children — from ephebophiles, people attracted to older adolescents and teens. Either way, acting on such attractions is a crime against children.
Adults who target older youth may be more subtle in how they approach their targets, and that’s why parents should monitor all their teens’ relationships with adults, both virtual and in real life. A 17-year-old may look grown, and may balk at this supervision. But their brain still has nearly a decade before it can consistently make mature decisions.
Adolescence is a time of deep insecurity, when teens are highly sensitive to others’ opinions. As Giuffre noted in her memoir, people like Epstein are adept at “reading a room.” They can intuit what a vulnerable teen needs, and offer it, exacting their price later.
3. Even as maturing teens pull away, parents must work harder to stay connected and know what is happening in their teens’ lives. Set special times — driving to school can be ideal — to ask questions that require more than a yes-no answer. Take the time to learn the names of their friends, teachers, and coaches, so they know you’re really interested. Leave a surprise note on their bed telling them you’re proud of something they did. Teens need steady validation of their worth — not only for achievements, but simply for who they are. Keeping their self-esteem “cup” as full as possible is an important protective factor.
Predators are master manipulators. They can patiently work their way into an adolescent’s confidence, shoring up fragile self-esteem. That’s why it’s so critical for parents to be their children’s consistent support. Predators don’t just live on private islands and roam the world in private jets; they can run the social hierarchy as the “alpha” in a high school, or orchestrate hazing in a college fraternity or sorority.
4. Use the Epstein news as a moment to remind kids what a bully really is: someone who repeatedly uses their power to hurt, scare, or control a more vulnerable person. It is also a crucial chance to talk about sexual health and safety. Explain how youth of any age can be vulnerable to exploitation, and be explicit that sex should never be traded for anything.
A colleague raising teens put it starkly when I asked how she was handling the Epstein stories: “Kids are watching how we handle this as adults, and they are not impressed.” The children of this attorney are likely not the only ones who wonder why Epstein went so lightly punished, or why our culture seems to condone sexualized images of teens.
Ask your children what they’ve read and heard, what they think it means, and listen. Then share your thoughts and values. All adults can show the young people in our lives that we can do better — by talking openly about abuse, bullying, harmful media messages and whatever else is troubling our children. We can show them that we stand behind them and will advocate for safer policies in schools and communities.
Janet Rosenzweig MS, PhD, MPA is author of the book “The Sex-Wise Parent,” a senior policy analyst at The Institute for Human Services, and a member of the board of directors of The National Coalition to Prevent Child Sexual Abuse and Exploitation.
Republicans think patients should be shopping for better healthcare prices. The party has long pushed to give patients money and let consumers do the work of reducing costs. After some GOP lawmakers closed out 2025 advocating to fund health savings accounts, President Donald Trump introduced his Great Healthcare Plan, which calls for, among other policies, requiring providers and insurers to post their prices “in their place of business.”
The idea echoes a policy implemented during his first term, when Trump suggested that requiring hospitals to post their charges online could ease one of the most common gripes about the healthcare system — the lack of upfront prices. To anyone who’s gotten a bill three months after treatment only to find mysterious charges, the idea seemed intuitive.
“You’re able to go online and compare all of the hospitals and the doctors and the prices,” Trump said in 2019 at an event unveiling the price transparency policy.
But amid low compliance and other struggles in implementing the policy since it took effect in 2021, the available price data is sparse and often confusing. And instead of patients shopping for medical services, it’s mostly health systems and insurers using the little data there is, turning it into fodder for negotiations that determine what medical professionals and facilities get paid for what services.
“We use the transparency data,” said Eric Hoag, an executive at Blue Cross Blue Shield of Minnesota, noting that the insurer wants to make sure providers aren’t being paid substantially different rates. It’s “to make sure that we are competitive, or, you know, more than competitive against other health plans.”
Not all hospitals have fallen in line with the price transparency rules, and many were slow to do so. A study conducted in the policy’s first 10 months found only about a third of facilities had complied with the regulations. The federal Centers for Medicare & Medicaid Services notified 27 hospitals from June 2022 to May 2025 that they would be fined for lack of compliance with the rules.
The struggles to make healthcare prices available have prompted more federal action since Trump’s first effort. President Joe Biden took his own thwack at the dilemma, by requiring increased data standardization and toughening compliance criteria. And in early 2025, working to fulfill his promises to lower health costs, Trump tried again, signing a new executive order urging his administration to fine hospitals and doctors for failing to post their prices. CMS followed up with a regulation intended to up the fines and increase the level of detail required within the pricing data.
So far, “there’s no evidence that patients use this information,” said Zack Cooper, a health economist at Yale University.
In 2021, Cooper co-authored a paper based on data from a large commercial insurer. The researchers found that, on average, patients who need an MRI pass six lower-priced imaging providers on the way from their homes to an appointment for a scan. That’s because they follow their physician’s advice about where to receive care, the study showed.
Executives and researchers interviewed by KFF Health News also didn’t think opening the data would change prices in a big way. Research shows that transparency policies can have mixed effects on prices, with one 2024 study of a New York initiative finding a marginal increase in billed charges.
The policy results thus far seem to put a damper on long-held hopes, particularly from the GOP, that providing more price transparency would incentivize patients to find the best deal on their imaging or knee replacements.
These aspirations have been unfulfilled for a few reasons, researchers and industry insiders say. Some patients simply don’t compare services. But unlike with apples — a Honeycrisp and a Red Delicious are easy to line up side by side — medical services are hard to compare.
For one thing, it’s not as simple as one price for one medical stay. Two babies might be delivered by the same obstetrician, for example, but the mothers could be charged very different amounts. One patient might be given medications to speed up contractions; another might not. Or one might need an emergency cesarean section — one of many cases in medicine in which obtaining the service simply isn’t a choice.
And the data often is presented in a way that’s not useful for patients, sometimes buried in spreadsheets and requiring a deep knowledge of billing codes. In computing these costs, hospitals make “detailed assumptions about how to apply complex contracting terms and assess historic data to create a reasonable value for an expected allowed amount,” the American Hospital Association told the Trump administration in July 2025 amid efforts to boost transparency.
Costs vary because hospitals’ contracts with insurers vary, said Jamie Cleverley, president of Cleverley and Associates, which works with healthcare providers to help them understand the financial impacts of changing contract terms. The cost for a patient with one health plan may be very different than the cost for the next patient with another plan.
The fact that hospital prices might be confusing for patients is a consequence of the lack of standardization in contracts and presentation, Cleverley said. “They’re not being nefarious.”
“Until we kind of align as an industry, there’s going to continue to be this variation in terms of how people look at the data and the utility of it,” he said.
Instead of aiding shoppers, the federally mandated data has become the foundation for negotiations — or sometimes lawsuits — over the proper level of compensation.
The top use for the pricing data for healthcare providers and payers, such as insurers, is “to use that in their contract negotiations,” said Marcus Dorstel, an executive at price transparency startup Turquoise Health.
Turquoise Health assembles price data by grouping codes for services together using machine learning, a type of artificial intelligence. It is just one example in a cottage industry of startups offering insights into prices. And, online, the startups’ advertisements hawking their wares often focus on hospitals and their periodic jousts with insurers. Turquoise has payers and providers as clients, Dorstel said.
“I think nine times out of 10 you will hear them say that the price transparency data is a vital piece of the contract negotiation now,” he said.
Of course, prices aren’t the only variable that negotiations hinge on. Hoag said Blue Cross Blue Shield of Minnesota also considers quality of care, rates of unnecessary treatments, and other factors. And sometimes negotiators feel as if they have to keep up with their peers — claiming a need for more revenue to match competitors’ salaries, for example.
Hoag said doctors and other providers often look at the data from comparable health systems and say, “‘I need to be paid more.’”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
The University of Pennsylvania is getting $7.8 million over the next two years to study an overlooked aspect of human health: the lymphatic system.
Often described as the body’s sewer system, its main job is to maintain the body’s balance of fluid and filter out waste. Millions of Americans live with dysfunction in the system, often unknowingly.
The time to diagnose some lymphatic disorders is at least five years, said Maxim Itkin, an interventional radiologist who directs Penn’s center specializing in lymphatic disorders.
He’s even had a patient who experienced unexplained symptoms for 50 years before getting treatment.
“Right now, most healthcare providers simply aren’t equipped — or trained — to recognize lymphatic dysfunction, and the tools they need are virtually nonexistent,” said Kimberley Steele, a program manager at the Advanced Research Projects Agency for Health (ARPA-H), the federal agency organizing the research effort.
That’s why the government, through ARPA-H, is investing $135.7 million toward research headed by 11 institutions in the U.S. and Canada, including Penn, to improve detection of issues in the lymphatic system.
With its slice of funding, the team at Penn will develop ways to image the network and identify hidden signs of disease.
An inside look
Similar to plumbing, fluids in the lymphatic system can be flowing, obstructed, or leaking.
Doctors are able to “close” these leaks and even “open” obstructed areas, but the problem is knowing when those procedures are needed.
Existing contrast agents — substances used to increase visibility of tissues during imaging — for the lymphatic system are largely considered obsolete and offer poor resolution, said Itkin, who is leading the Penn project, which started last October.
When he began researching the system 20 years ago, he “started to realize that it’s of enormous importance, and it’s forgotten primarily because nobody can image [it] and do interventions,” he said.
Maxim Itkin, an interventional radiologist at the Hospital of the University of Pennsylvania, found a way to track the flow of lymphatic fluid using X-ray imaging equipment.
Itkin and his team have come up with ways of imaging by injecting dye into lymph nodes and tissues and tracing the dye’s location. This has enabled him to diagnose hidden conditions and develop new treatment methods.
The ARPA-H funding will allow them to go even further, developing imaging agents that focus on the parts of the lymphatic system in the liver and gut — organs that generate the majority of the network’s flow in the body.
These will be used for CT (computed tomography) and MRI (magnetic resonance imaging) scans.
One of the imagingcandidates is designed to be swallowed and absorbed in the intestine, so doctors can see the lymphatic system in the gut. The second imaging agent will be administered via IV to show the system in the liver.
“It was my dream to see the lymphatic system from inside by itself,” Itkin said.
They’ll be using an approach called AI-driven multi-omics, where AI will analyze samples for unique molecules being excreted by the lymphatic system in the liver.
Penn and several other funded groups are working with the New York-based nonprofit Lymphatic Education and Research Network to help with research and patient recruitment.
Current funding is for two years, with the potential to extend for another three years.
Itkin says seeing the lymphatic system in the liver will be a thrill.
Before 1751, sick Pennsylvanians had few healthcare options other than often expensive home visits from doctors. That changed when Benjamin Franklin and physician Thomas Bond established a medical institution to treat the physically and mentally ill for free.
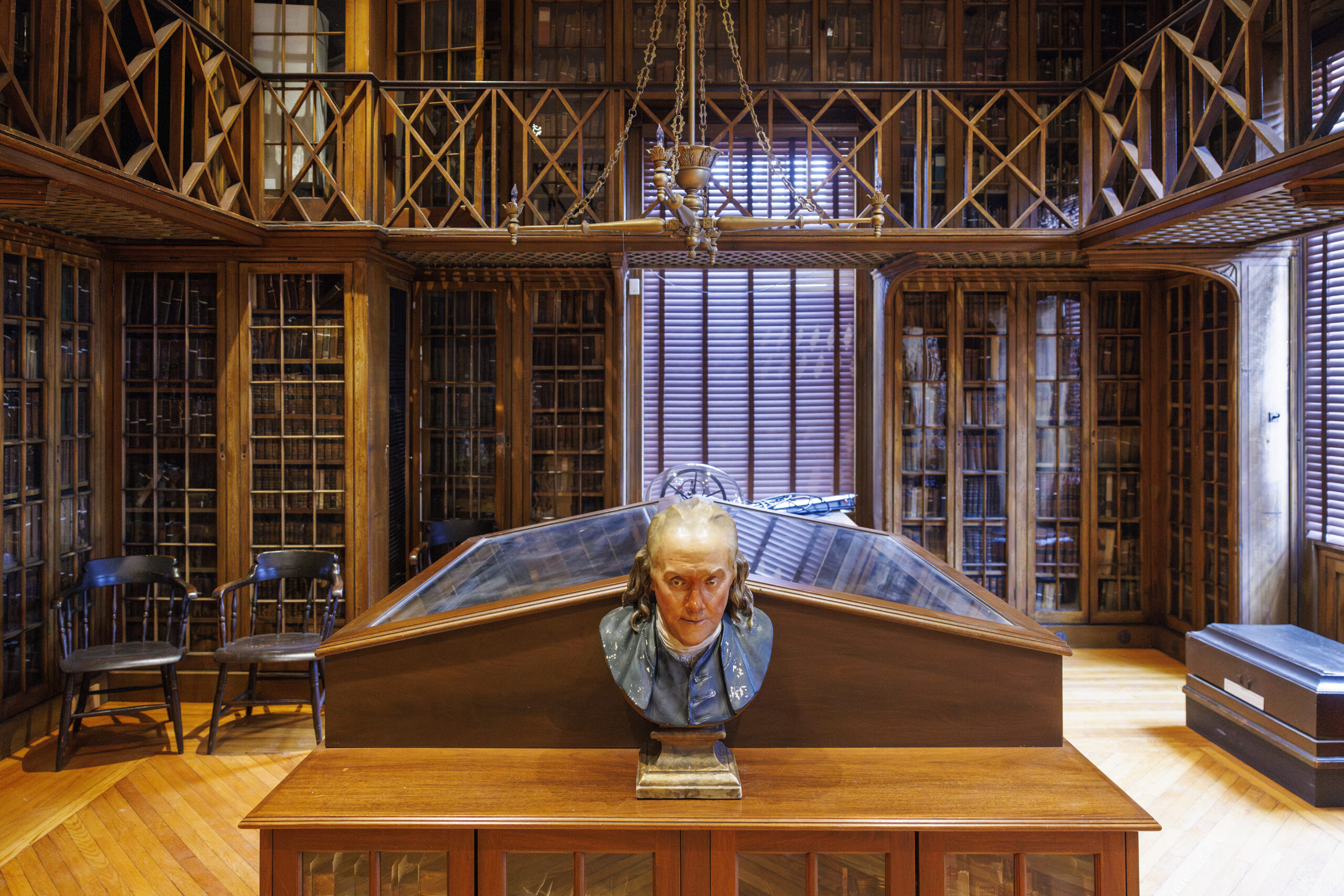
The result was the Pennsylvania Hospital on Spruce Street. The 275-year-old institution became home to the country’s first surgical amphitheater to teach students, the oldest medical library, and a nursing museum, among other historic firsts. It continues to advancemedical research as part of Penn Medicine.
Now the nation’s oldest charteredhospital will become Philadelphia’s newest museum.
The hospital’s Pine Building, which started construction in 1755, will be converted to the Pennsylvania Hospital Museum, Penn announced on Monday. The museum in the majestic Georgian architecture building at Eighth and Pine Streets, designed by architect Samuel Rhoads, is scheduled to open to the public on May8.
“It’s a very Philadelphia story to hear the history of the hospital because it really is about caring for other people,” said Stacey Peeples, lead archivist at Pennsylvania Hospital.
Stacey Peeples, lead archivist at Pennsylvania Hospital, described artifacts in the hospital’s new museum.
The medical library, surgical amphitheater, and apothecary have all been restored for the museum. Eight galleries will feature videos, hands-on activities, and archival objects describing the history of the hospital and the care it delivered.
The opening of the museum in the hospital’s 275th year coincides with America’s Semiquincentennial celebrations. (The University of Pennsylvania Health System, which merged with the hospital in October 1997, will run the museum.)
One of Peeples’ favorite items on display is a collection of medical cases compiled by the hospital’s doctors in the early 19th century.
Housed in the historic library, the book is flipped to a page showing a man with a seven-pound tumor in his cheek and neck area. Visitors can also find the actual preserved tumor from 1805 on display in the back of the room.
A historic medical book compiling interesting cases at Pennsylvania Hospital shows an image of Pete Colberry, a patient who fell from ship rigging and was stabilized on a bed to hold him in place, circa 1804.
A look at early medicine
Pennsylvania Hospital’s apothecary — where medicines were mixed and sold — was last used for that purpose in the early 1900s.
Most recently, it served as a conference room.
It’ll now be restored to its original layout, based on historic images from the 19th century. That includes bringing back alcoves filled with shelves of bottles, the scale used to weigh ingredients, as well as a giant counter where the apothecary could mix medications, Peeples said.
An archival image of Mildred Carlisle working in the Pennsylvania Hospital apothecary, circa 1920s.
In the historic library, the only room ready for news media to view this week, the artifacts remained scattered around.
A tonsil guillotine, designed to remove tonsils using a blade, sat next to early surgical tools and stethoscopes. Some objects, such as the scalpel, have not changed significantly in form through the years.
“But how we treat those objects certainly is very, very different. We want to make sure everything’s sanitized now,” Peeplessaid.
Surgical instruments belonging to Dr. James Wilson from the 1800s.
Other artifacts included old tools of medical education.Like three anatomical casts of women who died during childbirth in the mid-1700s that were used for anatomical study in lieu of cadavers.
The museum’s exhibits will showcase the hospital’s history of delivering care related to behavioral health and women’s health, as well as its role treating patients during times of conflicts, beginning with the Seven Years’ War, and through pandemics.
“People would always talk about us being able to do something on a larger scale like this, and I honestly wasn’t sure that was ever going to happen,” said Peeples, who has been at the hospital for 25 years.
Tickets will go on sale at the end of the month and cost $12 per person, with discounts for those 12 and under, 65 and over, and the military.
The plan is for the museum to be a permanent fixture, open Wednesdays to Sundays. The rest of the hospital will keep operating as normal.
Interior of the Historic Library of Pennsylvania Hospital, located at Eighth and Pine Streets.
The hospital, older than the nation, houses 517 licensed inpatient beds, and saw 19,759 adult admissions, 54,023 emergency department visits, and 5,163 births in fiscal year 2025, per Penn Medicine’s statement.
“Pennsylvania Hospital is a jewel in the crown that is Penn Medicine, where our staff draw energy from our rich history to shape the future of medicine,” Alicia Gresham, CEO of Pennsylvania Hospital, said in a statement.
Jefferson Health oncologist Jennifer Johnson had exhausted all the standard treatment options for her 49-year-old patient with esophageal cancer, who was likely to die within months.
Surgery, chemotherapy, radiation, and immunotherapy had kept the Northeast Philadelphia woman alive for six years after her diagnosis, but no longer were enough to stop her cancer from spreading.
Johnson knew her patient needed something novel. She recalled a presentation several years prior at a conference for head and neck cancers, where a doctor discussedan experimental treatment called T-cell receptor (TCR) therapy.
This type of cancer immunotherapy works by engineering the immune system to fight cancer, and falls into the same family of treatments as CAR-T, or chimeric antigen receptor (CAR) T cell therapy, an approach pioneered at the University of Pennsylvania that has revolutionized treatment for blood cancers.
She thought TCR therapy’s clever approach could work against solid tumors, where CAR-T had not been effective.
“I just remember sitting in the room and watching him present, thinking, I’m gonna use that one day,” the oncologist and cancer researcher recalled.
As it would happen, the approach was being tested in a phase II clinical trial at Rutgers Cancer Institute against tumors just like her patient’s: metastatic cancers driven by a virus called human papillomavirus 16. One of the most common strains, HPV16 causes roughly half of cervical cancer cases worldwide, as well as cancers of the head and neck area, anus, and genitals.
Cases that reach the metastatic stage like Johnson’s patient often run out of treatment options. Whether T-cell receptor therapy would work was unknown, but the alternatives were expected to fail.
“Anything that you might offer them would definitely not be expected to make their cancer go away completely and do it for a long time,” said Christian Hinrichs, the oncologist and scientist heading the trial whose presentation Johnson saw.
But interim results from the first half of the trial showed improvement in six out of 10 patients, whose tumors at least partially shrank. And two of them had no evidence of cancer after treatment.
Johnson’s patient, Maria Pascale, was one of thetwo whose promising early results were presented at a medical conference and highlighted in a research abstract in the Journal for ImmunoTherapy of Cancer in November.
She arrived at the health system in New Jersey in the summer of 2024 in such poor health thather lungs were starting to collapse.
The therapy has enabled her to celebrate two birthdays, start martial arts classes, reunite with old friends visiting from Argentina, and see her 23-year-old son get engaged.
“Imagine the wedding, then later the grandkids, I’m always thinking about [that],” she said.
What is a T-cell receptor therapy?
In the immune system, T cells act as frontline defenders against viruses, bacteria, and other threats.
Sometimes, these cells aren’t great at their jobs.
In the face of cancer, T cells can become exhausted over time, and fail to recognize invaders or mount attacks.
The idea behind immunotherapy is to transform these regular immune cells into cancer-fighting super-soldiers.
The Rutgers approach, an engineered TCR therapy, involves collecting T cells from a patient’s blood and genetically engineering them to better target a cancer cell for attack.
Afterward, the scientists grow more of the enhanced T cells in the lab and infuse them back into the patient.
The “prototype” for this style of therapy is CAR-T, a treatment that has saved tens of thousands of lives since the first FDA approval in 2017. Scientists have not yet been able to replicate the therapy’s success in blood cancers in solid cancers, although some early stage trials have shown potential.
TCR therapy is thought to be more promising against the latter cancer type — which is what’s being treated in the Rutgers trial — due to differences in the way the engineered T cells identify cancer cells.
CAR-T therapy uses what’s called a chimeric antigen receptor, a protein that recognizes a cell as cancer based on what’s on the outside of the cell.
It’s like knowing you’re at your friend’s house because of a specific doormat or set of house numbers on the exterior.
TCR therapy uses what’s called a T-cell receptor, which can recognize cancer cells based on what’s inside the cell.
It’s like knowing you’re at your friend’s house because you can see your friend inside.
Sometimes cancer cells have more unique identifiable elements on the outside, but other times they don’t. Imagine if multiple houses had the same doormat.
“That target would be on other cells that aren’t cancer cells and cause lots of toxicity,” said Carl June, the pioneering cancer scientist at Penn who developed the first FDA-approved CAR-T therapy and was not involved in the Rutgers trial.
That’s been the problem that’s held back CAR-T’s use in solid tumors.
The target in the Rutgers trial is a protein called HPV16 E7, found inside the cell. In tumors driven by the virus HPV16, it plays a key role in turning a cell into cancer.
“That’s like going after its Achilles’ heel,” June said.
Swarming the cancer
Pascale first arrived at Thomas Jefferson University Hospital in Center City in 2018 after suffering injuries in a car accident.
Doctors found a mass in the 43-year-old’s neck that turned out to be cancer.
Surgeons removed the mass,and she was fine until 2021 when doctors, including Johnson, found the cancer at the top of her esophagus.
They treated her with a combination of chemotherapy and radiation, which worked until March of 2022, when the cancer started appearing in Pascale’s lungs.
“All bets were off,” Johnson said.
Doctors gave Pascale chemotherapy and immunotherapy over the next couple of years, but in the spring of 2024, she developed an allergy to one of her chemotherapy drugs.
Around the same time, the cancer spread to the skin on Pascale’s back.
That’s when Johnson transferred her care to Hinrichs’ team at Rutgers.
Pascale started preparations for the treatment in July 2024, spending a couple weeks in the hospital.
The Rutgers team took T cells from her blood, gave her chemotherapy to knock her immune system down, and then transfused the engineered cells back into her body.
Within 48 hours, Pascale started feeling horrible.
“It was painful. It was my whole body, like I had pneumonia,” she said.
She had trouble breathing as the cells fought the cancer in her lungs. Hinrichs described it as “the T cells swarming the cancer,” leading to an inflammatory reaction.
The same thing occurred on her back. When Pascale’s sister came over, she saw one of the tumors in her skin was suddenly the size of a lemon.
Another one appeared red and felt like someone was burning a cigarette on her back.
The pain continued for three days, and then she felt well enough to go home. Pascale and her sister could see and feel the nodules on her back get smaller, until eventually they were gone.
Roughly five months later, Pascale’s scans showed no evidence of cancer. As of last month, a year and a half after she received the treatment, that was still true.
“What’s three days of pain compared with the opportunity that I have to live a lot of beautiful things with my family and friends?” Pascale said.
Maria Pascale walks with her sister Maria Durante and her doctor Christian Hinrichs at Rutgers.
The future of the treatment
Hinrichs said his team is working to figure out why two of the patients, including Pascale and a patient with anal cancer, responded better to the treatment.
He cautioned that it’s too early to draw sweeping conclusions since the sample size is small. (Researchers will seek to recruit another 10 patients for the ongoing trial.)
The patients who had complete responses will need follow-up scans every few months to make sure their cancers have not returned.
It will still take years to finish evaluating safety and efficacy. Treatments tested in clinical trials often do not advance to become standard practice.
June, the Penn scientist, called the trial’s early results promising and noted that there weren’t any major safety problems reported.
Adverse effects seen in the trial were mainly those caused by the chemotherapy.
However, the drawback of using TCR therapy is that patients need a certain genetic background for it to work, June said. This is similar to how not every organ donor would be a good match for a recipient.
The genetic profile chosen for the Rutgers therapy is the most common in America. However, it is less common in Black and Asian people compared to white people.
Scientists hope it could one day be possible to manufacture the therapy witha warehouse approach, where TCR therapies that work across genetic backgrounds could be mixed and matched.
“It’s a practical issue that the drug companies face,” June said.
CAR-T, in comparison, canbe used more broadly across different genetic backgrounds.
What matters most, since the treatment is expensive to make, is that the responses hold up over time, June said.
(The TCR therapy’s cost has not yet been set, Hinrichs said, since it is currently manufactured individually for each patient.)
“If they’re long lasting, then it’s really going to be a huge advance because nothing else works in the patients he’s treated,” June said.
At Jefferson, Johnson is cautiously optimistic about the treatment that has kept her patient alive.
If the therapy makes it through the rest of the trial process and proves effective, she hopes it could become “another thing in our armamentarium against this type of cancer.” (A type that doctors would hope to see less of since the introduction of the HPV vaccine in 2006.)
“I can’t tell you how wonderful it is to have a patient responding and living well when you saw things going the wrong way,” Johnson said.
Editor’s note: This story has been updated to clarify where the research has been presented and a reference to the prevalence of the genetic profile used in TCR therapy.
A person infected with measles traveled through Philadelphia International Airport last week, city health officials are warning.
The infected person spent time in Terminal E of the airport between 1:35 and 4:30 p.m. Thursday.
Measles is highly contagious and spreads via airborne particles when an infected person coughs, sneezes, or talks. The virus can linger in the air for up to two hours after the infected person moves.
Palak Raval-Nelson, Philadelphia’s health commissioner, said he believed there was no threat to the general public, but encouraged those who are not protected against measles to take action.
Children under a year old, pregnant people without immunity, and those with a weakened immune system who were exposed and who develop symptoms through March 5 should call their doctor immediately. They’re also asked to call their local health department and Philadelphia’s Health Department if they live outside the city.
Symptoms of the disease are fever, runny nose, cough, and watery, red eyes — as well as a rash.
Those who have immunity do not need to do anything. Those with immunity include people born before 1957, those who have already had measles, and those who have received two doses of the measles, mumps, and rubella vaccine.
Measles, in some cases, can lead to pneumonia, brain infection, and death, health officials say.
Rebekah Stewart, a nurse at the U.S. Public Health Service, got a call last April that brought her to tears. She had been selected for deployment to the Trump administration’s new immigration detention operation at Guantánamo Bay, Cuba.
This posting combined Donald Trump’s longtime passion to use the offshore base to move “some bad dudes” out of the United States with a promise made shortly after his inauguration last year to hold thousands of noncitizens there. The naval base is known for the torture and inhumanetreatment of men suspected of terrorism in the wake of 9/11.
“Deployments are typically not something you can say no to,” Stewart said. She pleaded with the coordinating office, which found another nurse to go in her place.
Other public health officers who worked at Guantánamo in the past year described conditions there for the detainees, some of whom learned they were in Cuba from the nurses and doctors sent to care for them. They treated immigrants detained in a dark prison called Camp 6, where no sunlight filters in, said the officers, whom KFF Health News agreed not to name because they fear retaliation for speaking publicly. It previously held people with suspected ties to al-Qaeda. The officers said they were not briefed ahead of time on the details of their potential duties at the base.
Although the Public Health Service is not a branch of the U.S. armed forces, its uniformed officers — roughly 5,000 doctors, nurses, and other health workers — act like stethoscope-wearing soldiers in emergencies. The government deploys them during hurricanes, wildfires, mass shootings, and measles outbreaks. In the interim, they fill gaps at an alphabet soup of government agencies.
The Trump administration’s mass arrests to curb immigration have created a new type of health emergency as the number of people detained reaches record highs. About 71,000 immigrants are currently imprisoned, according to Immigration and Customs Enforcement data, which show that most have no criminal record.
Homeland Security Secretary Kristi Noem has said: “President Donald Trump has been very clear: Guantánamo Bay will hold the worst of the worst.” However, several news organizationshave reported that many of the men shipped to the base had no criminal convictions. As many as 90% of them were described as “low-risk” in a May progress report from ICE.
In fits and starts, the Trump administration has sent about 780 noncitizens to Guantánamo Bay, according to the New York Times. Numbers fluctuate as new detainees arrive and others are returned to the U.S. or deported.
While some Public Health Service officers have provided medical care to detained immigrants in the past, this is the first time in American history that Guantánamo has been used to house immigrants who had been living in the U.S. Officers said ICE postings are getting more common. After dodging Guantánamo, Stewart was instructed to report to an ICE detention center in Texas.
“Public health officers are being asked to facilitate a man-made humanitarian crisis,” she said.
Seeing no option to refuse deployments that she found objectionable, Stewart resigned after a decade of service. She would give up the prospect of a pension offered after 20 years.
“It was one of the hardest decisions I ever had to make,” she said. “It was my dream job.”
One of her PHS colleagues, nurse Dena Bushman, grappled with a similar moral dilemma when she got a notice to report to Guantánamo a few weeks after the shooting at the Centers for Disease Control and Prevention in August. Bushman, who was posted with the CDC, got a medical waiver delaying her deployment on account of stress and grief. She considered resigning, then did.
“This may sound extreme,” Bushman said. “But when I was making this decision, I couldn’t help but think about how the people who fed those imprisoned in concentration camps were still part of the Nazi regime.”
Others have resigned, but many officers remain. While they are alarmed by Trump’s tactics, detained people need care, multiple PHS officers told KFF Health News.
“I respect people and treat them like humans,” said a PHS nurse who worked in detention facilities last year. “I try to be a light in the darkness, the one person that makes someone smile in this horrible mess.”
The PHS officers conceded that their power to protect people was limited in a detention system fraught with overcrowding, disorganization, and the psychological trauma of uncertainty, family separations, and sleep deprivation.
“Ensuring the safety, security, and well-being of individuals in our custody is a top priority at ICE,” said Tricia McLaughlin, chief spokesperson for the Department of Homeland Security, in an emailed statement to KFF Health News.
Adm. Brian Christine, assistant secretary for health at the Department of Health and Human Services (HHS), which oversees the Public Health Service, said in an email: “Our duty is clear: say ‘Yes Sir!’, salute smartly, and execute the mission: show up, provide humane care, and protect health.” Christine is a recent appointee who, until recently, was a urologist specializing in testosterone and male fertility issues.
“In pursuit of subjective morality or public displays of virtue,” he added, “we risk abandoning the very individuals we pledged to serve.”
Into the unknown
In the months before Stewart resigned, she reflected on her previous deployments, during Trump’s first term, to immigration processing centers run by Customs and Border Protection. Fifty women were held in a single concrete cell in Texas, she recalled.
“The most impactful thing I could do was to convince the guards to allow the women, who had been in there for a week, to shower,” she said. “I witnessed suffering without having much ability to address it.”
Stewart spoke with Bushman and other PHS officers who were embedded at the CDC last year. They assisted with the agency’s response to ongoing measles outbreaks, with sexually transmitted infection research, and more. Their roles became crucial last year as the Trump administration laid off droves of CDC staffers.
Stewart, Bushman, and a few other PHS officers at the CDC said they met with middle managers to ask for details about the deployments: If they went to Guantánamo and ICE facilities, how much power would they have to provide what they considered medically necessary care? If they saw anything unethical, how could they report it? Would it be investigated? Would they be protected from reprisal?
Stewart and Bushman said they were given a PHS office phone number they could call if they had a complaint while on assignment. Otherwise, they said, their questions went unanswered. They resigned and so never went to Guantánamo.
PHS officers who were deployed to the base told KFF Health News they weren’t given details about their potential duties — or the standard operating procedure for medical care — before they arrived.
Stephen Xenakis, a retired Army general and a psychiatrist who has advised on medical care at Guantánamo for two decades, said that was troubling. Before health workers deploy, he said, they should understand what they’ll be expected to do.
The consequences of insufficient preparation can be severe. In 2014, the Navy threatened tocourt-martial one of its nurses at Guantánamo who refused to force-feed prisoners on hunger strike, who were protesting inhumane treatment and indefinite detention. The protocol was brutal: A person was shackled to a five-point restraint chair as nurses shoved a tube for liquid food into their stomach through their nostrils.
“He wasn’t given clear guidance in advance on how these procedures would be conducted at Guantánamo,” Xenakis said of the nurse. “Until he saw it, he didn’t understand how painful it was for detainees.”
The American Nurses Association and Physicians for Human Rights sided with the nurse, saying his objection was guided by professional ethics. After a year, the military dropped the charges.
A uniformed doctor or nurse’s power tends to depend on their rank, their supervisor, and chains of command, Xenakis said. He helped put an end to some inhumane practices at Guantánamo more than a decade ago, when he and other retired generals and admirals publicly objected to certain interrogation techniques, such as one called “walling,” in which interrogators slammed the heads of detainees suspected of terrorism against a wall, causing slight concussions. Xenakis argued that science didn’t support “walling” as an effective means of interrogation, and that it was unethical, amounting to torture.
Medics practice evacuating a detained immigrant in a simulated exercise at Guantánamo in April 2025.
Torture hasn’t been reported from Guantánamo’s immigration operation, but ICE shift reports obtained through a Freedom of Information Act request by the government watchdog group American Oversight note concerns about detainees resorting to hunger strikes and self-harm.
“Welfare checks with potential hunger strike IA’s,” short for illegal aliens, says an April 30 note from a contractor working with ICE. “In case of a hunger strike or other emergencies,” the report adds, the PHS and ICE are “coordinating policies and procedures.”
“De-escalation of potential pod wide hunger strike/potential riot,” says an entry from July 8. “Speak with alien on suicide watch regarding well being.”
Inmates and investigations have reported delayed medical care at immigration detention facilities and dangerous conditions, including overcrowding and a lack of sanitation. Thirty-two people died in ICE custody in 2025, making it the deadliest year in two decades.
“They are arresting and detaining more people than their facilities can support,” one PHS officer told KFF Health News. The most prevalent problem the officer saw among imprisoned immigrants was psychological. They worried about never seeing their families again or being sent back to a country where they feared they’d be killed. “People are scared out of their minds,” the officer said.
U.S. service members stand by during an April 2025 simulated medical evacuation of immigrants detained at Guantánamo.
No sunlight
The PHS officers who were at Guantánamo told KFF Health News that the men they saw were detained in either low-security barracks, with a handful of people per room, or in Camp 6, a dark, high-security facility without natural light. The ICE shift reports describe the two stations by their position on the island, Leeward for the barracks and Windward for Camp 6. About 50 Cuban men sent to Guantánamo in December and January have languished at Camp 6.
A Navy hospital on the base mainly serves the military and other residents who aren’t locked up — and in any case, its capabilities are limited, the officers said. To reduce the chance of expensive medical evacuations back to the U.S. to see specialists quickly, they said, the immigrants were screened before being shipped to Guantánamo. People over age 60 or who needed daily drugs to manage diabetes and high blood pressure, for example, were generally excluded. Still, the officers said, some detainees have had to be evacuated back to Florida.
PHS nurses and doctors said they screened immigrants again when they arrived and provided ongoing care, fielding complaints including about gastrointestinal distress and depression. One ICE monthly progress report says, “The USPHS psychologist started an exercise group” for detainees.
Doctors’ requests for lab work were often turned down because of logistical hurdles, partly due to the number of agencies working together on the base, the officers said. Even a routine test, a complete blood count, took weeks to process, vs. hours in the U.S.
DHS and the Department of Defense, which have coordinated on the Guantánamo immigration operation, did not respond to requests for comment about their work there.
One PHS officer who helped medically screen new detainees said they were often surprised to learn they were at Guantánamo.
“I’d tell them, ‘I’m sorry you are here,’” the officer said. “No one freaked out. It was like the ten-millionth time they had been transferred.” Some of the men had been detained in various facilities for five or six months and said they wanted to return to their home countries, according to the officer. Health workers had neither an answer nor a fix.
Unlike ICE detention facilities in the U.S., Guantánamo hasn’t been overcrowded. “I have never been so not busy at work,” one officer said. A military base on a tropical island, Guantánamo offers activities such as snorkeling, paddleboard yoga, and kickboxing to those who aren’t imprisoned. Even so, the officer said they would rather be home than on this assignment on the taxpayer’s dime.
Transporting staff and supplies to the island and maintaining them on-base is enormously expensive. The government paid an estimated $16,500 per day, per detainee at Guantánamo, to hold those accused of terrorism, according to a 2025 Washington Post analysis of Department of Defense data. (The average cost to detain immigrants in ICE facilities in the U.S. is $157 a day.)
Even so, the funding has skyrocketed: Congress granted ICE a record $78 billion for fiscal year 2026, a staggering increase from $9.9 billion in 2024 and $6.5 billion nearly a decade ago.
Last year, the Trump administration also diverted more than $2 billion from the national defense budget to immigration operations, according to a report from congressional Democrats. About $60 million of it went to Guantánamo.
“Detaining noncitizens at Guantánamo is far more costly and logistically burdensome than holding them in ICE detention facilities within the United States,” wrote Deborah Fleischaker, a former assistant director at ICE, in a declaration submitted as part of a lawsuit brought by the American Civil Liberties Union early last year. In December, a federal judge rejected the Trump administration’s request to dismiss a separate ACLU case questioning the legality of detaining immigrants outside the U.S.
Anne Schuchat, who served with the PHS for 30 years before retiring in 2018, said PHS deployments to detention centers may cost the nation in terms of security, too. “A key concern has always been to have enough of these officers available for public health emergencies,” she said.
Andrew Nixon, an HHS spokesperson, said the immigration deployments don’t affect the public health service’s potential response to other emergencies.
In the past, PHS officers have stood up medical shelters during hurricanes in Louisiana and Texas, rolled out COVID testing in the earliest months of the pandemic, and provided crisis support after the deadly shooting at Sandy Hook Elementary School and the Boston Marathon bombing.
“It’s important for the public to be aware of how many government resources are being used so that the current administration can carry out this one agenda,” said Stewart, one of the nurses who resigned. “This one thing that’s probably turning us into the types of countries we have fought wars against.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.