NEW YORK — Since Robert F. Kennedy Jr. was sworn in to lead the U.S. Department of Health and Human Services one year ago, he has defended his upending of federal health policy by saying the changes will restore trust in America’s public health agencies.
But as the longtime leader of the anti-vaccine movement scales back immunization guidance and dismisses scientists and advisers, he’s clashed with top medical groups who say he’s not following the science.
The confrontation is deepening confusion among the public that had already surged during the COVID-19 pandemic. Surveys show trust in the agencies Kennedy leads is falling, rather than rising, as the country’s health landscape undergoes dramatic change.
Kennedy says he’s aiming to boost transparency to empower Americans to make their own health choices. Doctors counter that the false and unverified information he’s promoting is causing major, perhaps irreversible, damage — and that if enough people forgo vaccination, it will cause a surge of illness and death.
There was a time when people trusted health agencies regardless of party and the government reported “the best of what science knows at this point,” said Kathleen Hall Jamieson, director of the Annenberg Public Policy Center at the University of Pennsylvania.
“Now, you cannot confidently go to federal websites and know that,” she said.
HHS spokesman Andrew Nixon argued that trust had suffered during the Biden administration. “Kennedy’s mandate is to restore transparency, scientific rigor, and accountability,” he said.
Trust slid during the COVID pandemic
Historically, federal scientific and public health agencies enjoyed strong ratings in public opinion polls. The U.S. Centers for Disease Control and Prevention for decades scored above many other government agencies in Gallup surveys that asked whether they were doing a “good” or “excellent” job.
Two decades ago, more than 60% of Americans gave the CDC high marks, according to Gallup. But that number fell dramatically at the beginning of the COVID-19 pandemic, amid agency mistakes and guidance that some people didn’t like.
In 2020, the percentage of Americans who believed the CDC was doing at least a “good” job fell to 40% and then leveled off for the next few years.
Alix Ellis, a hairstylist and mom in Madison, Georgia, used to fully trust the CDC and other health agencies but lost that confidence during the COVID-19 pandemic. She said some of the guidance didn’t make sense. At her salon, for example, stylists could work directly on someone’s hair, but others in the room had to be several feet away.
“I’m not saying that we were lied to, but that is when I was like, OK, ‘Why are we doing this?’” the 35-year-old said.
Kennedy helped create the trust problem, doctor says
Part of Kennedy’s pitch as health secretary has been restoring Americans’ trust in public health.
“We’re going to tell them what we know, we’re going to tell them what we don’t know, and we’re going to tell them what we’re researching and how we’re doing it,” Kennedy told senators last September, while explaining how he intended to make the CDC’s information reliable. “It’s the only way to restore trust in the agency — by making it trustworthy.”
Before entering politics, Kennedy was one of the loudest voices spreading false information about immunizations. Now, he’s trying to fix a trust problem he helped create, said Dr. Rob Davidson, a Michigan emergency physician.
“You fed those people false information to create the distrust, and now you’re sweeping into power and you’re going to cure the distrust by promoting the same disinformation,” said Davidson, who runs a doctor group called the Committee to Protect Health Care. “It’s upside-down.”
Kennedy has wielded the power of his office to take multiple steps that diverge from medical consensus.
Last May, he announced COVID-19 vaccines were no longer recommended for healthy children and pregnant women, a move doctors called concerning and confusing.
In November, he directed the CDC to abandon its position that vaccines do not cause autism, without supplying new evidence. And earlier this year, the CDC under his leadership reduced the number of vaccines recommended for every child, a decision medical groups said would undermine protections against a half-dozen diseases.
Kennedy also has overhauled his department through canceled grants and mass layoffs. Last summer, Kennedy fired his new CDC chief after less than a month over disagreements about vaccine policy.
Confusion emerges as trust erodes
Some have applauded the moves. But surveys suggest many Americans have had the opposite reaction.
“I have much less trust,” said Mark Rasmussen, a 67-year-old retiree walking into a mall in Danbury, Connecticut, one recent morning.
Shocked by Kennedy’s dismantling of public health norms, professional medical groups have urged Americans not to follow new vaccine recommendations they say were adopted without public input or compelling evidence.
The American Academy of Pediatrics, along with more than 200 public health and advocacy groups, urged Congress to investigate how and why Kennedy changed the vaccine schedule. The American Medical Association, working with the University of Minnesota’s Vaccine Integrity Project, this week announced a new evidence-based process for reviewing the safety of respiratory virus vaccines — something they say is needed since the government stopped doing that kind of systematic review.
Many Democratic-led states also have rebuffed Kennedy’s policies, even creating their own alliances to counter his vaccine guidance.
“We see burgeoning confusion about which sources to trust and about which sources are real. That makes decision-making on an individual level much harder,” said Dr. Megan Ranney, dean of the Yale School of Public Health.
She said she worried the confusion was contributing to the recent rise in diseases like whooping cough and measles, which were once largely eliminated in the U.S.
Surveys indicate growing public wavering over support for the measles-mumps-rubella vaccine. Although a large majority of people support giving it to children, the proportion declined significantly in just over nine months, according to Annenberg research. An August 2025 survey finds that 82% would be “very” or “somewhat” likely to recommend that an eligible child in their household get MMR vaccine, compared with 90% in November 2024.
Surveys show trust is declining again
New findings from the healthcare research nonprofit KFF in January show that 47% of Americans trust the CDC “a great deal” or “a fair amount” to provide reliable vaccine information, down about 10 percentage points since the beginning of Trump’s second term.
Trust among Democrats dropped 9 percentage points since September, to 55%, the survey found. Trust among Republicans and independents hasn’t changed since September, but it has declined somewhat among both groups since the beginning of Trump’s term.
Even among MAHA supporters, the poll shows, fewer than half say they trust agencies like the CDC and FDA “a lot” or “some” to make recommendations about childhood vaccine schedules.
Gallup surveys also show a drop in Americans who believe the CDC is doing a “good job,” from 40% in 2024 to 31% last year.
Those results came alongside a decline of trust across the government — not just agencies under Kennedy’s oversight. Yet concerns about Kennedy’s trustworthiness also have emerged in the past year. Documents recently obtained by The Associated Press and The Guardian, for example, undermine his statements that a 2019 trip to Samoa ahead of a measles outbreak had “nothing to do with vaccines.” The documents have prompted senators to assert that Kennedy lied to them over the visit.
HHS officials say they are promoting independent decision-making by families while working to reduce preventable diseases. They say reducing routine vaccine recommendations was meant to ensure parents vaccinate children against the riskiest diseases.
HHS did not make Kennedy available for an interview, despite repeated requests. But as he has pledged to restore trust, he’s also urged people to come to their own conclusions.
“This idea that you should trust the experts,” Kennedy said recently on The Katie Miller Podcast, “a good mother doesn’t do that.”
SAN JUAN, Puerto Rico — Puerto Rico’s governor on Thursday signed a bill that amends a law to recognize a fetus as a human being, a move doctors and legal experts warn will have deep ramifications for the U.S. Caribbean territory.
The amendment was approved without public hearings and amid concerns from opponents who warned it would unleash confusion and affect how doctors and pregnant or potentially pregnant women are treated.
The new law will lead to “defensive health care,” warned Dr. Carlos Díaz Vélez, president of Puerto Rico’s College of Medical Surgeons.
“This will bring complex clinical decisions into the realm of criminal law,” he said in a phone interview.
He said that women with complicated pregnancies will likely be turned away by private doctors and will end up giving birth in the U.S. mainland or at Puerto Rico’s largest public hospital, noting that the island’s crumbling health system isn’t prepared.
“This will bring disastrous consequences,” he said.
Díaz noted that the amended law also allows a third person to intervene between a doctor and a pregnant woman, so privacy laws will be violated, adding that new protocols and regulations will have to be implemented.
“The system is not prepared for this,” he said.
Gov. Jenniffer González, a Republican and supporter of U.S. President Donald Trump, said in a brief statement that “the legislation aims to maintain consistency between civil and criminal provisions by recognizing the unborn child as a human being.”
The amendment, in Senate Bill 923, was made to an article within Puerto Rico’s Penal Code that defines murder.
The government noted that the amendment complements a law that among other things, classifies as first-degree murder when a pregnant woman is killed intentionally and knowingly, resulting in the death of the conceived child at any stage of gestation. The law was named after Keishla Rodríguez, who was pregnant when she was killed in April 2021. Her lover, former Puerto Rican boxer Félix Verdejo, received two life sentences after he was found guilty in the killing.
Some cheered the amendment signed into law Thursday, while opponents warned that it opens the door to eventually criminalizing abortions in Puerto Rico, which remain legal.
“A zygote was given legal personality,” said Rosa Seguí Cordero, an attorney and spokesperson for the National Campaign for Free, Safe and Accessible Abortion in Puerto Rico. “We women were stripped of our rights.”
Seguí rattled off potential scenarios, including whether a zygote, or fertilized egg, would have the right to health insurance and whether a woman who loses a fetus would become a murder suspect.
Díaz said doctors could even be considered murder suspects and condemned how public hearings were never held and the medical sector never consulted.
“The problem is that no medical recommendations were followed here,” he said. “This is a serious blow … It puts us in a difficult situation.”
Among those condemning the measure was Annette Martínez Orabona, executive director for the American Civil Liberties Union in Puerto Rico.
She noted that no broad discussion of the bill was allowed, which she said is critical because the penal code carries the most severe penalties.
“There is no doubt that the measure did not undergo adequate analysis before its approval and leaves an unacceptable space for ambiguity regarding civil rights,” she said.
“The legislative leadership failed to fulfill its responsibility to the people, and so did the governor.”
WASHINGTON — The Trump administration on Thursday revoked a scientific finding that long has been the central basis for U.S. action to regulate greenhouse gas emissions and fight climate change, the most aggressive move by the Republican president to roll back climate regulations.
The rule finalized by the Environmental Protection Agency rescinds a 2009 government declaration known as the endangerment finding that determined that carbon dioxide and other greenhouse gases threaten public health and welfare. The Obama-era finding is the legal underpinning of nearly all climate regulations under the Clean Air Act for motor vehicles, power plants and other pollution sources that are heating the planet.
The repeal eliminates all greenhouse gas emissions standards for cars and trucks and could unleash a broader undoing of climate regulations on stationary sources such as power plants and oil and gas facilities, experts say. Legal challenges are near certain.
President Donald Trump called the move “the single largest deregulatory action in American history, by far,” while EPA Administrator Lee Zeldin called the endangerment finding “the Holy Grail of federal regulatory overreach.”
Trump called the endangerment finding “one of the greatest scams in history,” claiming falsely that it “had no basis in fact” or law. “On the contrary, over the generations, fossil fuels have saved millions of lives and lifted billions of people out of poverty all over the world,” Trump said at a White House ceremony, although scientists across the globe agree that carbon dioxide and other greenhouse gases are driving catastrophic heat waves and storms, droughts and sea level rise.
Environmental groups described the move as the single biggest attack in U.S. history against federal authority to address climate change. Evidence backing up the endangerment finding has only grown stronger in the 17 years since it was approved, they said.
“This action will only lead to more climate pollution, and that will lead to higher costs and real harms for American families,” said Fred Krupp, president of Environmental Defense Fund, adding that the consequences would be felt on Americans’ health, property values, water supply and more.
The EPA also said it will propose a two-year delay to a Biden-era rule restricting greenhouse gas emissions by cars and light trucks. And the agency will end incentives for automakers who install automatic start-stop ignition systems in their vehicles. The device is intended to reduce emissions, but Zeldin said “everyone hates” it.
Zeldin, a former Republican congressman who was tapped by Trump to lead EPA last year, has criticized his predecessors in Democratic administrations, saying that in the name of tackling climate change, they were “willing to bankrupt the country.”
The endangerment finding “led to trillions of dollars in regulations that strangled entire sectors of the United States economy, including the American auto industry,” Zeldin said. “The Obama and Biden administrations used it to steamroll into existence a left-wing wish list of costly climate policies, electric vehicle mandates and other requirements that assaulted consumer choice and affordability.”
The endangerment finding and the regulations based on it “didn’t just regulate emissions, it regulated and targeted the American dream. And now the endangerment finding is hereby eliminated,” Zeldin said.
Supreme Court has upheld the endangerment finding
The Supreme Court ruled in a 2007 case that planet-warming greenhouse gases, caused by the burning of oil and other fossil fuels, are air pollutants under the Clean Air Act.
Since the high court’s decision, in a case known as Massachusetts v. EPA, courts have uniformly rejected legal challenges to the endangerment finding, including a 2023 decision by the U.S. Court of Appeals for the District of Columbia Circuit.
The endangerment finding is widely considered the legal foundation that underpins a series of regulations intended to protect against threats made increasingly severe by climate change. That includes deadly floods, extreme heat waves, catastrophic wildfires and other natural disasters in the United States and around the world.
Gina McCarthy, a former EPA administrator who served as White House climate adviser in the Biden administration, called the Trump administration’s actions reckless. “This EPA would rather spend its time in court working for the fossil fuel industry than protecting us from pollution and the escalating impacts of climate change,” she said.
Former President Barack Obama said on X that repeal of the endangerment finding will make Americans “less safe, less healthy and less able to fight climate change — all so the fossil fuel industry can make even more money.”
Dr. Lisa Patel, a pediatrician and executive director of the Medical Society Consortium on Climate and Health, said Trump’s action “prioritizes the profits of big oil and gas companies and polluters over clean air and water” and children’s health.
“As a result of this repeal, I’m going to see more sick kids come into the Emergency Department having asthma attacks and more babies born prematurely,” she said in a statement. “My colleagues will see more heart attacks and cancer in their patients.”
David Doniger, a climate expert at the Natural Resources Defense Council, said Trump and Zeldin are trying to use repeal of the finding as a “kill shot’’ that would allow the administration to make nearly all climate regulations invalid. The repeal could erase current limits on greenhouse gas pollution from cars, factories, power plants and other sources and could hinder future administrations from imposing rules to address global warming.
The EPA action follows an executive order from Trump that directed the agency to submit a report on “the legality and continuing applicability” of the endangerment finding. Conservatives and some congressional Republicans have long sought to undo what they consider overly restrictive and economically damaging rules to limit greenhouse gases that cause global warming.
Withdrawing the endangerment finding “is the most important step taken by the Trump administration so far to return to energy and economic sanity,” said Myron Ebell, a conservative activist who has questioned the science behind climate change.
Tailpipe emission limits targeted
Zeldin and Transportation Secretary Sean Duffy have moved to drastically scale back limits on tailpipe emissions from cars and trucks. Rules imposed under Democratic President Joe Biden were intended to encourage U.S. automakers to build and sell more electric vehicles. The transportation sector is the largest source of greenhouse gas emissions in the U.S.
The Trump administration announced a proposal in December to weaken vehicle mileage rules for the auto industry, loosening regulatory pressure on automakers to control pollution from gasoline-powered cars and trucks. The EPA said its two-year delay to a Biden-era rule on greenhouse gas emissions by cars and light trucks will give the agency time to develop a plan that better reflects the reality of slower EV sales, while promoting consumer choice and lowering prices.
Environmental groups said the plan would keep polluting, gas-burning cars and trucks on U.S. roads for years to come, threatening the health of millions of Americans, particularly children and the elderly.
A new sign with orange letters outside a former Rite Aid in Germantown announces the arrival of a primary care model new to the Philadelphia region.
ArchWell Health recently opened its first three of eight planned primary care centers here for people with Medicare Advantage, promising convenient and personalized care in neighborhoods with a relative lack of doctors.
Two others have opened on North Broad Street, near Stenton and Susquehanna Avenues, also in former Rite Aid stores.
A privately held company based in Nashville, Tenn., ArchWell says it can offer patients greater access to healthcare throughlower patient-provider ratios.
Itplans to limit each of itsphysicians to no more than 500 patients — about a fifth of the patient load for typical primary care doctors. Nurse practitioners working under the doctors will manage a maximum of 250 patients,officials said.
The approach is built around a financial model that differentiates ArchWell from Medicare-focused competitors already in Philadelphia like Oak Street Health and ChenMed’s Dedicated Senior Medical Centers. ArchWell only accepts patients who have private Medicare or are willing to switch to it. Oak Street and ChenMed also accept traditional Medicare.
Privately run Medicare Advantage plans are increasingly popular among people ages 65 and older who qualify for government-funded Medicare coverage. Advantage plans appeal to people bycovering services, such as dental and vision care, left out of traditional Medicare, but have come under scrutiny for exaggerating how sick patients are to rack up more revenue.
ArchWell sees exclusively working with Medicare Advantage plans as helping doctors to focus solely on the best outcomes for patients, rather than on providing more services to bring in more revenue, a criticism of traditional Medicare, said Doron Schneider, its medical director for the Philadelphia market.
Melissa A. Herd, community relations specialist for ArchWell Health in Philadelphia, is shown outside the company’s Germantown location, which is in a former Rite Aid building.
“You have different incentives, you have different care models, you have different case management models, you have different ways to treat one person versus the other,” Schneider said.
Before starting at ArchWell in late 2024, Schneider worked at Tandigm Health, an Independence Health Group company founded in 2014 with the goal of helping primary care doctors manage costs and improve care for their patients. He learned there how hard it is for doctors to work with different types of insurers and the varied incentives that go with them.
How ArchWell conducts business
ArchWell, which opened its first clinic in 2021 in Birmingham, Ala., operates under contracts with Medicare Advantage plans. The plans give ArchWell a portion of the monthly payment they get from Medicare for each patient. That money is supposed to cover all of the person’s medical costs.
Aetna, UnitedHealthcare, and Devoted Health have contracts with ArchWell to cover the Philadelphia market. ArchWell is close to getting contracts with HealthSpring and Humana, Schneider said. Those five companies had more than 90,000 people in their plans in December, according to federal data.
Aetna and UnitedHealthcare said they work with clinics like ArchWell’s around the country to improve health outcomes and leave patients more satisfied with their experience.
“We are pleased that they are now an option for Aetna Medicare Advantage members in the Philadelphia area,” Aetna said in a statement.
ArchWell declined to provide financial details, such as annual revenue from the more than 80 clinics it had in a dozen states before coming to Philadelphia or how much it spends to open each center. ArchWell representatives also did not disclose who its owners are.
The interior of Archwell Health’s Germantown primary care clinic has Philadelphia-centric images painted on the walls.
Company founder Carl Whitmer worked at Clayton, Dubilier & Rice, a global private equity firm, before founding ArchWell.
“We have partners that are focused on our sustainability and growth,” said Christina Cober, ArchWell’s vice president of marketing.
But companies focused on primary care for seniors haven’t always been as successful as anticipated.
Oak Street, founded in Chicago in 2012, grew rapidly and now services 450,000 patients at 230 centers across the country. It declined to say how many patients it has in Philadelphia. Oak Street arrived here in 2018.
CVS Health bought Oak Street in 2023 for $10.6 billion, anticipating that it would expand to more than 300 centers by this year. Last fall, CVS announced it was closing 16 centers and taking a $5.7 billion write-down on its health-services business, largely because of slower anticipated growth at Oak Street.
ArchWell says itslowerpatient-provider ratios allow more frequent interactions with patients. If a patient is diagnosed with high blood pressure, Schneider said, the message to the patient is: “We’ll see you back in a week. We’ll see you back in two weeks.”
The repeat visits happen with no cost to the member and no extra revenue to ArchWell because all care is supposed to be covered by a monthly payment per member.
ArchWell expects to add about 300 patients per year at each center, said Cober. Staffing at the centers starts out with a physician, a nurse-practitioner, two care navigators, two medical assistants, and a center manager.
Among the early patients at ArchWell’s center on Germantown Avenue is Marcella James, 69, who lives across the street from the clinic and watched as the building was transformed from a shuttered Rite Aid.
“I walked over there one day just to see what it was like and what they offer, and I signed up right away,” James said. James likes her doctor at Temple Health, but ArchWell was irresistibly convenient.
“If I can get the same help or better help from ArchWell is to be seen because I just started with them,” she said.
AmeriHealth Caritas, one of the nation’s largest Medicaid insurers, is closing its in-house pharmacy benefits manager, PerformRx, by the end of this year, the Newtown Square company said in an announcement to employees Wednesday.
Health insurers effectively subcontract with pharmacy benefit managers to oversee drug benefits. They have become increasingly powerful cogs in healthcare and face new restrictions under a law signed by President Donald Trump this month.
OptumRx, a unit of UnitedHealth Group Inc. and one of the three largest PBMs, is scheduled to take over for PerformRx on Jan. 1. OptumRx already provides PBM services to the majority owner of AmeriHealth Caritas, Independence Health Group. Independence is best known for its Independence Blue Cross business.
“This decision reflects evolving market and regulatory landscape, not the performance or dedication of our PerformRx leadership or associates,” the AmeriHealth Caritas announcement to staff said.
Caritas said in a statement to The Inquirer that it expected a “limited impact on jobs, with many functions remaining in-house to support the same high-quality experience for members and providers.”
The company did not elaborate on the market and regulatory changes that precipitated the decision to close PerformRx, which Caritas formed in 1999. PerformRx has contracts in 13 states, including Pennsylvania and Delaware, according to the Caritas website.
Every year, I climb to the top of Everest. It’s no big deal. I take it one step at a time, 80,000 steps per year.
By the time Dec. 31 arrives, I calculated, I have ascended at least seven vertical miles, carrying loads roughly equal to the weight of three pickup trucks, mostly composed of laundry, groceries, and small children.
You see, I live on the top floor of a duplex.
Public health messaging has convinced us that the only way to work out is “exercising.” Yet, for most of human history, of course, living was exercise. Humans got most — if not all — of the physical activity needed to stay healthy through natural movement in their daily lives.
After a half-century asking us to exercise more, doctors and physiologists say we have been thinking about it wrong. U.S. and World Health Organization guidelines no longer specify a minimum duration of moderate or vigorous aerobic activity.
Movement-tracking studies show even tiny, regular bursts of effort — as short as 30 seconds — can capture many of the health benefits of the gym. Climbing two to three flights of stairs a few times per day could change your life. Experts call it VILPA, or vigorous intermittent lifestyle physical activity.
“The message now is that all activity counts,” said Martin Gibala, a professor and former chair of the kinesiology department at McMaster University in Canada. And perhaps nothing’s better than stairs.
Here’s how to take your first step toward living to 100.
Staircase athletes
In the world’s “Blue Zones” — Sardinia, Italy; Okinawa, Japan; Nicoya Peninsula, Costa Rica; Ikaria, Greece; Loma Linda, California — a disproportionate number of people live to be 100 and beyond. Scientists aren’t certain why, but they’ve proposed several reasons, including diet, genetics, social connection, purpose, and daily physical activity, especially on hills and stairs.
The villagers of Sardinia, a rugged part of Italy, stand out. A typical octogenarian engages in dailyphysical activity equivalent to climbing many flights of stairs. When researchers looked at what was behind Sardinians’ extraordinary longevity, three factors — terrain slope, distance to workplace, and working as a shepherd (who often climb more than 1,000 feet per day) — were most strongly correlated with longer lives. In some regions, the global pattern of men dying earlier than women was virtually absent.
Since we can’t all move to Sardinia, as beautiful as it is, we can just stop avoiding gravity instead.
From a topological perspective, modern life has leveled what’s healthy about Blue Zones, replacing them with a “frictionless” landscape of elevators, cars, instant delivery, and sedentary jobs. Just about a quarter of U.S. adults meet the modest targets for aerobic activity.
Yet our stairs remain. And if you’re looking to maximize the benefits of short bouts of exercise, “stair climbing is the clear winner,” said Emmanuel Stamatakis, a professor of physical activity and population health at the University of Sydney.
That’s because of what stairs, and hill climbing generally, force your body to do. With each step, you must momentarily balance your entire body weight on one leg. As you ascend — an exquisite feat of neurological coordination — you’re constantly lifting at least 100 pounds into the air, boosting your heart rate and cardiovascular fitness. On the way down, bracing against the pull of gravity, you build bone density and muscle strength, especially in your quadriceps, hamstrings, glutes, calves, adductors, and core muscles.
Over the past decade, studies have shown the potency of going up and down stairs each day to boost your health. It doesn’t take much. Just taking the stairs daily is associated with lower body weight and cutting the risk of stroke and heart disease — the leading (and largely preventable) cause of death globally. While it may not burn many calories (most exercise doesn’t), it does appear to extend your health span. Leg power — a measure of explosive muscle strength — was a stronger predictor of brain aging than any lifestyle factors measured in a 2015 study in the journal Gerontology.
Subsequent studies put a finer point on it: Just nine to 10 brief bouts of vigorous activity per day — averaging 30 to 45 seconds each — lowered the risk of dying by about 40% in nonexercisers, according to a 2022 study in Britain. Benefits increased as people exercised longer, but most of the risk reduction occurred during the first few minutes of daily activity.
Anyone who has ever prepared for a race will be familiar with the question: What are you training for? At some point, I realized what I’m really training for — whether I acknowledge it or not — is the life I want to lead when I’m older.
If the goal is live independently and get out of a chair unassisted, something has to change for many Americans.
The belief that your daily routine isn’t exercise is a good place to start. The truth is that we don’t have “exercise” guidelines, Gibala said. We have physical activity guidelines. That doesn’t distinguish between the gym, dancing, or using your home stairs.
“Exercise doesn’t need to be this special thing you do in this special place after you change into special clothes,” Gibala said. “It can be part of everyday life.”
How little activity can you do?
Four minutes daily. Essentially, a few flights of stairs at a vigorous pace. That’s the effort Stamatakis found delivered significant health benefits in that 2022 study of British nonexercisers.
“We saw benefits from the first minute,” Stamatakis said.
For Americans, the effect is even more dramatic: a 44% drop in deaths, according to a peer-reviewed paper recently accepted for publication.
“We showed for the first time that vigorous intensity, even if it’s done as part of the day-to-day routine, not in a planned and structured manner, works miracles,” Stamatakis said. “The key principle here is start with one, two minutes a day. The focus should be on making sure that it’s something that you can incorporate into your daily routine. Then you can start thinking about increasing the dose.”
Intensity is the most important factor. You won’t break a sweat in a brief burst, but you do need to feel it. A highly conditioned athlete might need to sprint to reach vigorous territory. But many people need only to take the stairs. Use your breathing as a guide, Stamatakis said: If you can sing, it’s light intensity. If you can speak but not sing, you’re entering moderate exertion. If you can’t hold a conversation, it’s vigorous.
The biggest benefits come from moderate to vigorous movement. One minute of incidental vigorous activity prevents premature deaths, heart attacks or strokes as well as about three minutes of moderate activity or 35 to 49 minutes of light activity. Other studies show an even wider gap for reducing the risk of developing Type 2 diabetes:One minute of vigorous activity is roughly as effective as about 1½ hours of light activity.
If you rarely climb stairs, or it’s not safe to climb unassisted, then check with your doctor before starting any activity regimen.
How to do it
Home. Office. Subway. A step platform in your living room. All stairs work at every fitness level.
But they work best with someone else. That’s a lesson from Blue Zones: Social connection is probably essential to our health. You can’t “stair-climb” out of a solitary, stressful, junk-food-filled lifestyle on your own. Try a few sessions with a coach, friend, or social fitness app to stick to your routine.
If you want to know where your fitness level stands (or lies sprawled on the couch), the best gauge of cardiorespiratory fitness is VO2 max, a measure of how much oxygen your body can consume during intense exercise. You can test this in a lab, use a stopwatch or health app, or estimate it with an online calculator.
The most important thing? Start moving, said Gibala, who recommends beginning with at least 30 seconds of continuous climbing or one minute of ascending and descending. “It doesn’t matter what you are starting from, you’re still going to see benefits,” he said.
After that, it’s just one step at a time. I made a calculator through which you can estimate your annual ascents — and decide how many Everests you want to climb.
Are you planning a vacation to Spain, Italy, France, Greece, or another country along the Mediterranean?
If so, you should know about a parasite that puts travelers at risk of a rare disease, called “visceral leishmaniasis,” that can be deadly when untreated. The parasite — leishmania — is transmitted by a bite from an infected sandfly. It can lie dormant in the body for years, then latercause severe illness, including persistent high fever.
A 34-year-old South Jersey resident, Louis-Hunter Kean, died from it in late 2023 after doctors at two South Jersey medical systems and later at Penn Medicine missed the diagnosis. His symptoms developed about a year after he vacationed in Tuscany, where parasitic disease experts now believe he was infected.
“Leishmania in the U.S. is underappreciated,” said Joshua A. Lieberman, assistant director of the molecular microbiology clinical laboratory at University of Washington in Seattle. “We want to get the word out that there’s a lot more of it than we think.”
Parasitic disease experts say most American doctors don’t know enough about leishmania. Here’s what you should know about leishmania:
Visceral leishmaniasis is caused by the most deadly species. At risk are travelers to Southern Europe, Brazil, East Africa, India, and military personnel who were deployed to Afghanistan and Iraq. Its primary symptom is fever, along with an enlarged liver and spleen, weight loss, and a low blood cell count. Each year, an estimated 50,000 to 90,000 new cases are reported globally, according to the World Health Organization (WHO).
The majority of healthy people who get infected never experience symptoms or sickness. However, the parasite can cause severe illness in small children, senior citizens, and people who are malnourished or immunocompromised. It can activate decades after exposure.
Cutaneous leishmaniasis is the most common and less dangerous form of the disease. This species is present in the countries that also have visceral leishmaniasis, as well as in Israel, Mexico, Central and South America — and in a few U.S. states, including Texas, Oklahoma, and Arizona. More than 80 cases have been reported in the U.S. since 2017, though experts believe that’s an undercount, according to a recent study published in the digital journal JMIR Dermatology.
People with active cases first see small, red bumps on the skin that can develop into skin ulcers, which may ooze or scab. These symptoms typically appear within weeks or months after exposure, but ulcers can surface years later. Worldwide, an estimated 600,000 to 1 million cases occur each year, according to the WHO.
“If you’re traipsing through the rain forest in Central America, you’re at huge risk,” said leishmania expert David L. Sacks, an immunologist and senior investigator with the National Institutes of Health (NIH). “We see patients all the time at the NIH hospital who have the cutaneous form from traveling.”
Mucosal leishmaniasis is most commonly found in parts of the Amazon basin, specifically Bolivia, Peru, and Brazil. Symptoms usually start as a skin sore, which can advance to the nose, mouth, or throat and cause severe facial disfigurement. It can be life-threatening.
Can leishmaniasis be treated?
All three typesare treatable with antiparasitic and antifungal medications.
Some forms of cutaneous leishmaniasis will heal on their own.
More than 90% of patients with visceral leishmaniasis will die without treatment. An estimated 20,000 to 50,000 people die from it each year, according to research published in the academic journal Tropical Diseases, Travel Medicine and Vaccines.
How prevalent is leishmaniasis in the U.S.?
An exact number of cases is unknown. The federal government does not require doctors to report the disease to the Centers for Disease Control and Prevention. Texas is the only state that requires medical providers to report cases to the state health department.
How can you protect yourself against leishmaniasis?
There are no vaccines or drugs for prevention, but people can take steps to protect themselves when visiting areas where the parasite is circulating.
Sandflies are most active from dusk until dawn, so consider staying indoors during that time. Wear long-sleeved shirts and long pants, and socks that cover ankles. Apply insect repellent, preferably with DEET, to clothing and exposed skin. Sandflies can slip through window and door screens, so it’s best to stay in accommodations with air-conditioning or sleep under insecticide-treated bed nets.
People who are immunocompromised may want toavoid travel to regions with leishmania.
Also, if you experience symptoms, especially a high fever that won’t go away, provide your doctor with a thorough travel history, going back decades.
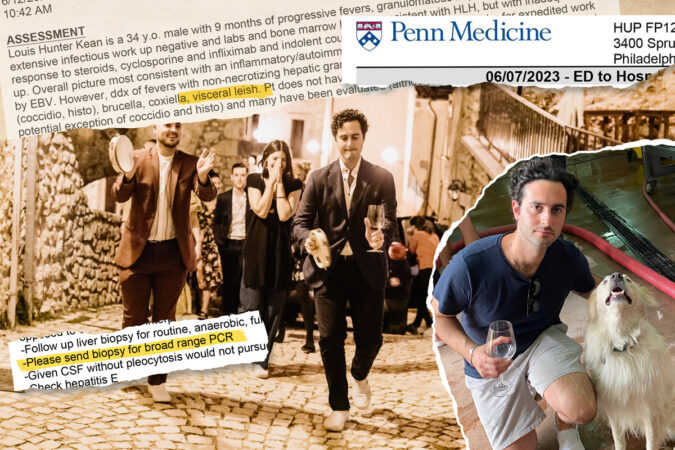
Each night, Louis-Hunter Kean spiked a fever as high as 104.5. He would sweat through bedsheets and shiver uncontrollably. By morning, his fever wouldease but his body stillached; even his jaw hurt.
He had been sick like this for months. Doctors near his South Jersey home couldn’t figure out why a previously healthy 34-year-old was suffering high fevers plus a swollen liver and spleen. In early 2023, they referred Kean to Penn Medicine.
Louis-Hunter Kean visiting a winery in the Tuscany region of Italy in September 2021. He first spiked a mysterious and persistent fever about a year later in August 2022.
“These doctors are very sharp, and there are a lot of teams working on it,” Kean texted a friend after being admitted to the Hospital of the University of Pennsylvania (HUP) in West Philadelphia.
Was it an infection? An autoimmune disease? A blood cancer? Over the next six months, at least 34 HUP doctors — rheumatologists, hematologist-oncologists, gastroenterologists, infectious disease and internal medicine specialists — searched for an answer.
Kean was hospitalized at HUP five times during a six-month period in 2023. His electronic medical chart grew to thousands of pages.
Along the way, doctors missed critical clues, such as failing to obtain Kean’s complete travel history. They recommended a pair of key tests, but didn’t follow up to make sure they got done, medical records provided to The Inquirer by his family show.
Doctors involved in Kean’s care, including at Penn, prescribed treatments that made him sicker, said four infectious disease experts not involved in his care during interviews with a reporter, who shared details about his treatment. Penn doctors continued to do so even as his condition worsened.
Louis-Hunter Kean receives a kiss from bride Ashley Greyson at the October 2021 wedding of his close friend, Joshua Green. Green and Kean graduated from Haddonfield High School in 2007.
“No one was paying attention to what the doctor before them did or said,” Kean’s mother, Lois Kean, said.
“They did not put all the pieces together,” she said. “It was helter-skelter.”
Kean’s family is now suing Penn’s health system for medical malpractice in Common Pleas Court in Philadelphia. The complaint identifies nearly three dozen Penn doctors, accusing them of misdiagnoses and harmful treatments. These physicians are not individually named as defendants.
In court filings, Penn says its doctors did not act recklessly or with disregard for Kean’s well-being, and his case is not indicative of any systemic failures within its flagship hospital. A Penn spokesperson declined further comment on behalf of both the hospital and the individual doctors involved in Kean’s care, citing the pending lawsuit.
The puzzle of Kean’s diagnosis finally came together in November 2023 after a Penn doctor, early in his career, sought help from the National Institutes of Health (NIH).
An NIH doctor recommended a test that identified the cause: a parasite prevalent in countries bordering the Mediterranean Sea. Kean likely got infected while vacationing in Italy, four parasitic disease experts told The Inquirer.
The infection, which is treatable when caught early, is so rare in the U.S. that most doctors here have never seen a case, the experts said.
By the time Penn doctors figured it out, Kean’s organs were failing.
Louis-Hunter Kean and his then-girlfriend Zara Gaudioso at a friend’s wedding in Tuscany in September 2021. Kean and Gaudioso got engaged in early 2023. Gaudioso was smitten by Kean’s good looks and sense of humor.While vacationing in Italy in September 2021, Louis-Hunter Kean and his friends hiked in the foothills of the Apennine Mountains and visited Gran Sasso and Monti della Laga National Park.
A missed clue
When a patient has an ongoing and unexplained fever, an infectious disease doctor will routinely start by takinga thorough travel history to screen for possible illnesses picked up abroad.
A medical student took Kean’s travel history during his initial workup at HUP in June 2023. An infectious disease specialist reviewed the student’s notes and added a Cooper University Hospital doctor’s earlier notes into Kean’s electronic medical chart at Penn.
Those records show Kean had traveled to Turks and Caicos with his fiancée in May 2022. The next month, he took a work trip out West, including to California, where he visited farms, but didn’t interact with livestock.
This was not unusual for Kean, who worked with fruits and vegetables imported from around the world at his family’s produce distribution center on Essington Avenue in Southwest Philadelphia.
Kean’s fiancée, Zara Gaudioso, said she repeatedly told doctors about another trip: In September 2021, about a year before his fevers began, they traveled to Italy for a friend’s wedding in Tuscany.
The couple hiked remote foothills, danced all night in a courtyard, dined by candlelight surrounded by a sunflower farm, and slept in rustic villas with the windows flung open.
“We told everybody,” Gaudioso said. “A lot of Americans go to Italy — it’s not like a third-world country, so I could see how it could just go in one ear and out the other.”
But notes in Kean’s medical record from the Penn infectious disease specialist don’t mention Italy. Neither do the ones the specialist copied over from Kean’s infectious disease doctor at Cooper.
Kean “does not have known risk factors” for exposure to pathogens, the Penn specialist concluded, except possibly from farm animals or bird and bat droppings.
Still, the specialist listed various diseases that cause unexplained fever: Tick-borne diseases. Fungal infections. Tuberculosis. Bacteria from drinking unpasteurized milk.
The possible culprits included a parasitic disease, called visceral leishmaniasis, transmitted by a bite from an infected sandfly. It can lie dormant for a lifetime — or, in rare cases, activate long after exposure, so it’s important for doctors to take extensive past travel histories, parasitic experts say.
The parasite is widely circulating in Southern European countries, including Spain, Greece, Portugal, and Italy.
“Mostly, people living there are the ones who get it. But it’s just a lottery sandwich, and there’s no reason that travelers can’t get it,” said Michael Libman, a top parasitic disease expert and former director of a tropical medicine center at McGill University in Canada.
But few cases become severe. Hospitals in Italy reported only 2,509 cases of active infection between 2011 and 2016, affecting fewer than one in 100,000 people. Infections requiring hospital care in Italy began to decline after 2012, according a 2023 European study by the Public Library of Science (PLOS) journal Neglected Tropical Diseases.
Caught early, visceral leishmaniasis is treatable. Without treatment, more than 90% of patients will die.
In addition to fever, other telltale symptoms are swelling of the liver and spleen and low blood cell counts. Kean had all of those.
A missed test
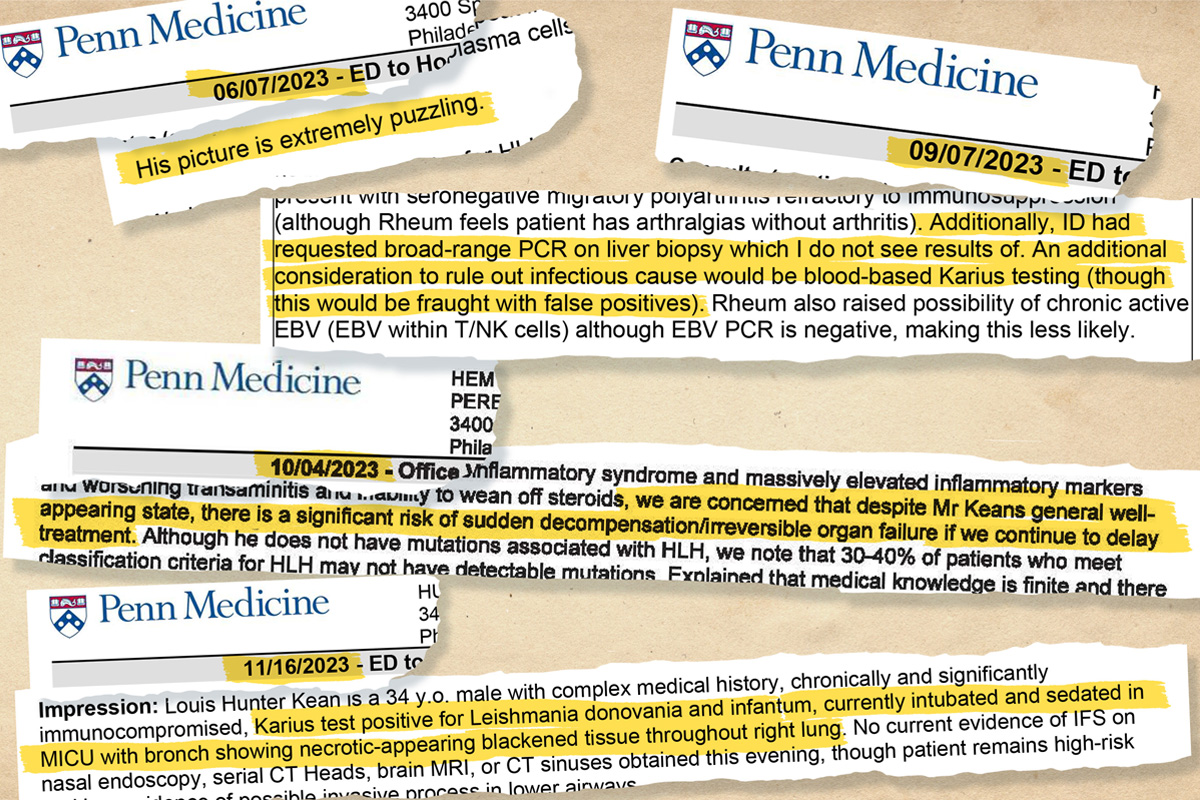
The infectious disease specialist requested a test to examine tissue biopsied from Kean’s liver, which was damaged and enlarged. Lab results showed that immune cells there had formed unusual clusters — another sign that his body might be fighting off an infection.
In her notes, the specialist identified “visceral leish” as a possible diagnosis, which repeated — via copy and paste — seven times in his medical record. Her request to “please send biopsy for broad-range PCR” repeated five times.
That is a diagnostic (polymerase chain reaction) test that looks for the genetic fingerprint of a range of pathogens.
The test comes in different versions: One looks broadly for bacteria. The other is for fungi. The broad fungal test candetect leishmania, even though it’s not a fungus. However, it’s not always sensitive enough to identify the parasite and can produce a false negative, experts said.
The specialist’s chart note doesn’t specify which type she wanted done.
It’s not clear if anyone asked. The test wasn’t done.
Louis-Hunter Kean (right, with wine glass and tambourine) leads a wedding procession through the small stone village of Santo Stefano di Sessanio in Italy’s Abruzzo region in September 2021.
She did not order a low-cost rapid blood test that screens specifically for leishmaniasis by detecting antibodies made by the immune system after fighting it. She also didn’t order a leishmania-PCR, which is highly targeted to detect the exact species of the parasite.
Nor did the medical record show that the specialist followed up on the results of the broader test she requested, even though she saw Kean on nine of the 13 days of his first hospitalization at HUP in June 2023.
Penn has a policy that a lead doctor on the patient’s case is responsible for making sure that recommended tests get done. The specialist was called in as a consultant on Kean’s case. During that June hospitalization alone, his medical chart grew to 997 pages.
Patient safety experts have warned for years that electronic medical record systems — designed for billing and not for care — can become so unwieldy that doctors miss important details, especially with multiple specialists involved, or repeat initial errors.
A seemingly innocuous step in charting — copying and pasting previous entries and layering on new ones— can add to the danger, patient safety experts say.
That’s how the specialist’s mention of “visceral leish” and her test recommendation got repeated in Kean’s chart.
Marcus Schabacker, president of ECRI, a nonprofit patient-safety organization based in Plymouth Meeting, said “copy and paste” in electronic medical records puts patients at risk of harm.
“The reality is if you are reading something over and over again, which seems to be the same, you’re just not reading it anymore. You say, ‘Oh, yeah, I read that, let’s go on,’” said Schabacker, speaking generally about electronic medical record systems and not specifically about Kean’s case.
Louis-Hunter Kean plays guitar in his younger years. He loved music and shared eclectic playlists with his friends.
When treatments harm
Penn doctors believed Kean had a rare,life-threatening disorder, known as hemophagocytic lymphohistiocytosis (HLH), in which the immune system attacks the body. Instead of fighting infections, defective immune cells start to destroy healthy blood cells.
In most adults, the constellation of symptoms diagnosed as HLH gets triggered when an underlying disease sends the body’s immune system into overdrive. Triggers include a blood cancer like lymphoma, an autoimmune disease like lupus, or an infection.
Penn doctors across three specialties — hematology-oncology, rheumatology, and infectious disease — were searching for the cause within their specialties.
“His picture is extremely puzzling,” one doctor wrote in Kean’s chart. “We are awaiting liver biopsy results. I remain concerned about a possible infectious cause.”
As HUP doctors awaited test results, they treated Kean’s HLH symptoms with high doses of steroids and immunosuppressants to calm his immune system and reduce inflammation.
The treatments, however, made Kean highly vulnerable to further infection.And defenseless against another possible trigger of HLH: visceral leishmaniasis.
At the time, a Penn rheumatologist involved in Kean’s care before his first hospitalization warned about steroids “causing harm” to Kean if it turned out he had an infection. He wrote, “please ensure all studies requested by” infectious disease are done, medical records show.
Steroid treatments would allow the parasites to proliferate unchecked, experts said.
“It’s unfortunately exactly the wrong treatment for parasitic disease,” said Libman, the leishmania disease expert at McGill University.
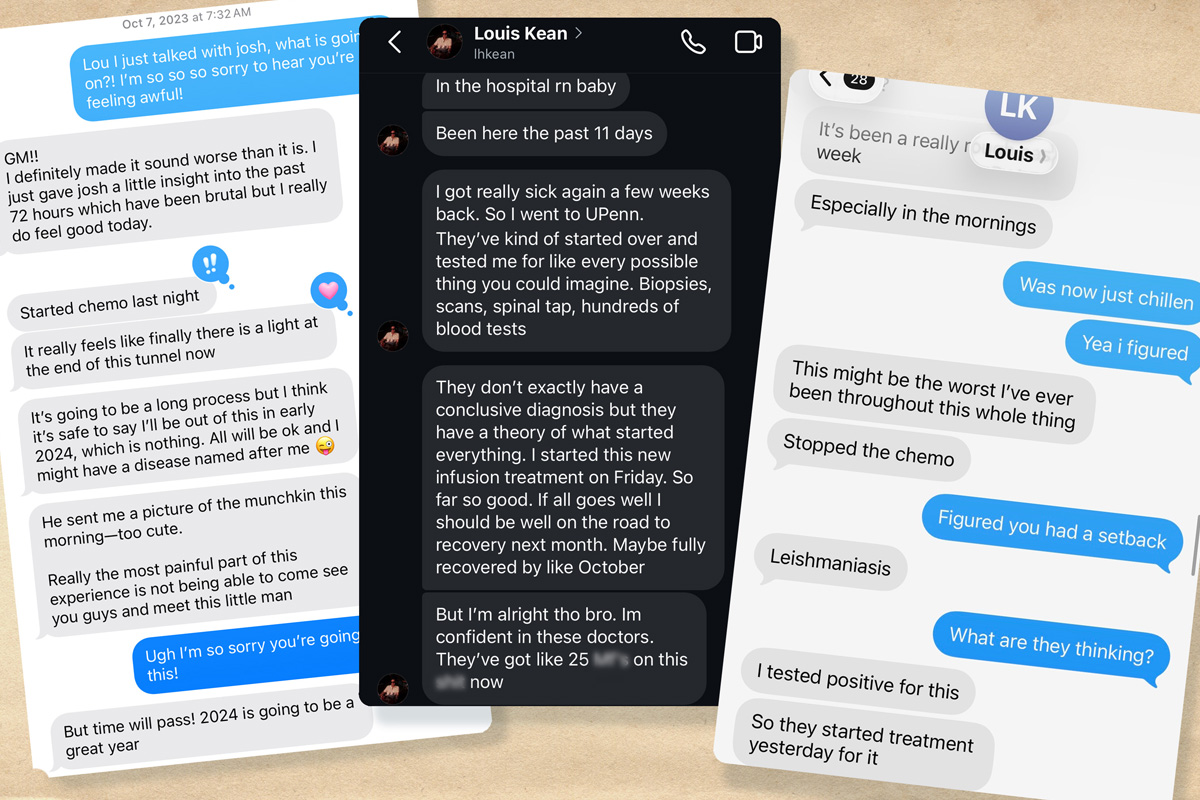
As Kean grew sicker, he was readmitted to HUP for a third time in September 2023. He texted a friend: “I’m on more medications than I’ve ever been on and my condition is worse than it’s ever been.”
A sampling of Louis-Hunter Kean’s electronic medical records, which ballooned to thousands of pages over five HUP hospitalizations within six months in 2023.
Handoffs between doctors
No single doctor seemed to be in charge of Kean’s care, his family said. And the number of specialists involved worried them.
“Everyone just kept being like, ‘We don’t know. Go see this specialist. Go see that specialist,’” Kean’s sister, Priscilla Zinsky, said.
By fall 2023, rheumatologists hadn’t found a trigger of Kean’s symptoms within their specialty. They turned to doctors specializing in blood cancer.
During the handoff, three doctors noted that they didn’t see the results of the test requested by the infectious disease specialist back in June. They still thought it was possible that Kean had an infection, records show.
“An additional consideration to rule out infectious cause would be blood-based Karius testing (though this would be fraught with false positives),” wrote that doctor, who was still training as a hematologist-oncologist.
A supervising physician reviewed the Sept. 8, 2023, note and signed off on it. The medical records don’t show any follow-up with infectious disease doctors, and the test wasn’t done at the time.
In the coming days, blood cancer specialists struggled to find a link between Kean’s symptoms and an underlying disease.
They thought he might have a rare form of leukemia, but tests weren’t definitive, Kean texted friends.
Untreated HLH symptoms can lead to rapid organ failure, so doctors often start patients on treatment while trying to figure out the underlying cause, said Gaurav Goyal, a leading national expert on HLH, noting that it can take days to get test results.
“You have to walk and chew the gum. You have to calm the inflammation so the patient doesn’t die immediately, and at the same time, try to figure out what’s causing it by sending tests and biopsies,” said Goyal, a hematologist-oncologist at the University of Alabama at Birmingham.
Medical records show that Penn doctors feared Kean was at “significant risk” of “irreversible organ failure.”
They suggested a more aggressive treatment: a type of chemotherapy used to treat HLH that would destroy Kean’s malfunctioning immune cells.
In his medical record, a doctor noted that beginning treatment without a clear diagnosis was “not ideal,” but doctors thought it was his best option.
Four parasitic disease experts told The Inquirer that chemotherapy, along with steroids and immunosuppressants, can be fatal to patients with visceral leishmaniasis.
“If that goes on long enough, then they kill the patient because the parasite goes out of control,” Libman said, explaining that ramping up the HLH treatments weakens the immune system. “The parasite has a holiday.”
A sample of text messages from Louis-Hunter Kean to friends during separate HUP hospitalizations over a six-month period in 2023.
Chemo as last resort
Kean banked his sperm, because chemo infusions can cause infertility. He told friends he trusted his Penn team and hoped to make a full recovery.
“Started chemo last night. It really feels like finally there is a light at the end of the tunnel,” he texted a friend on Oct. 7, 2023.
“I’m gonna get to marry my best friend, and I think I’m going to be able to have children,” Kean wrote in another text to a different friend.
Kean spent nearly all of October at HUP getting chemo infusions. He rated his pain as a nine out of 10. His joints throbbed. He couldn’t get out of bed. He started blacking out.
Doctors added a full dose of steroids on top of the IV chemo infusion. By the end of the month, Kean told a friend he feared he was dying.
A year had passed since Kean first spiked a fever. He no longer could see himself returning to his former life — one filled with daily exercise, helping run his family’s produce store, nights out with friends at concerts and bars, and vacations overseas.
Lethargic and weak, he could barely feed himself. His sister tried to spoon-feed him yogurt in his hospital bed.
He started texting reflections on his life to friends and family, saying his illness had given him a “polished lens” through which he could see clearly. He wrote that their love felt “like a physical thing, like it’s a weighted blanket.”
“I’ve lived an extremely privileged life. I don’t think it’s possible for me to feel bad for myself,” he said in a text. “And I don’t want anyone else to either.”
Louis-Hunter Kean enjoying dinner out with his sister, Jessica Kean, in Manhattan in 2014. Friends and family described him as a “foodie” and health food advocate prior to the onset of his illness in August 2022.
Puzzle solved
One doctor involved in Kean’s care had seen him at Penn’s rheumatology clinic in early June 2023, just before his first HUP hospitalization. The doctor, a rheumatology fellow,urged him to go to HUP’s emergency department, so he could be admitted for a medical workup.
The fellowremained closely involved in Kean’s care, medical records show. Also in his 30s, this doctor shared Kean’s interests in music, fashion, and the city’s restaurant scene, according to Kean’s family.
“They had a rapport,” Kean’s father, Ted Kean, said. “Louis thought a lot of him, and he seemed to think a lot of my son.”
By early November 2023, the rheumatology fellow was extremely concerned, medical records show.
The chemo infusions weren’t helping. Kean still was running a fever of 103. The fellow wrote in his chart that he was worried Kean needed a bone-marrow transplant to replace his failing immune system.
And doctors still didn’t know the root of his symptoms.
The fellowcontacted the NIH, medical notes show.
An NIH doctor recommended a test to check for rare pathogens, including parasites that cause visceral leishmaniasis,according to family members present when the testing was discussed.
The NIH-recommended Karius test was the same one suggested two months earlier by the Penn hematologist-oncologist in training, but with no follow-up.
File of sign on front of Hospital of the University of Pennsylvania (HUP) taken on Tuesday, March 19, 2024.
On Nov. 16, the fellow got the results. He went to Kean’s bedside.
After five HUP hospitalizations over six months, a single test had revealed the cause of his illness: visceral leishmaniasis.
Kean cried with relief and hugged the fellow, joined by his mother and sister.
“‘You saved my life,’” Kean’s sister, Jessica Kean, recalled her brother telling the doctor. “‘Finally, we know what this is, and we can treat it.’”
Kean’s medical chart was updated to note that he traveled to “Italy in the past,” also noting he had visited Nicaragua and Mexico. A HUP infectious disease doctor consulted with the Centers for Disease Control and Prevention on antiparasitic medications.
Meanwhile, Kean’s nose wouldn’t stop bleeding. He felt light-headed and dizzy, with high fever. Even on morphine for his pain, his joints ached.
“I’ve been struggling, buddy,” he texted a friend on Nov. 20. “This might be the worst I’ve ever been.”
By Nov. 22, he stopped responding to text messages. He began hallucinating and babbling incoherently, family members recalled. “Things went downhill very, very quickly, like shockingly quickly,” his sister, Priscilla Zinsky, said.
When she returned on Thanksgiving morning, he was convulsing, thrashing his head and arms. “It was horrifying to see,” Zinsky said.
Her brother had suffered brain bleeds that caused a stroke. His organs were failing. He had a fungal infection with black mold growing throughout his right lung, medical records show.
Kean was put on life support, with a doctor noting the still-preliminary diagnosis: “Very medically ill with leishmaniasis.”
“Prognosis is poor,” read the note in his Nov. 29, 2023, medical records.
A few hours later, Kean’s family took him off life support. He died that day.
“All of his organs were destroyed,” said Kean’s mother, Lois Kean. “Even if he had lived, he had zero quality of life.”
Portraits of Lois and Ted Kean’s four children decorate a wall at their home in Haddonfield. Their son, Louis-Hunter, died after contracting visceral leishmaniasis, a parasitic infection he likely picked up in Italy. When caught early, it’s treatable with medication. It’s deadly without treatment.
It’s not clear why the parasites began to attack Kean a year after his return from Italy. Healthy people rarely develop severe disease from exposure to the deadly form of the parasite circulating outside the U.S., experts said.
Most people infected by a sandfly “are probably harboring small amounts of the parasite” in their organs, according to Naomi E. Aronson, a leishmania expert and director of infectious diseases at the Uniformed Services University of the Health Sciences in Bethesda, Md.
“Most of the time, you don’t have any problem from it,” Aronson said.
Children under age 5, seniors, and people who are malnourished or immunodeficient are most susceptible to visceral leishmaniasis. Aronson said she worries about people who might harbor the parasite without problems for years, and then become immunocompromised.
Libman, the parasitic expert from McGill, said he’s seen six to 10 patients die from visceral leishmaniasis because doctors unfamiliar with the disease mistakenly increased immunosuppressants to treat HLH during his 40 years specializing in parasite disease.
“That’s a classic error,” he said.
Kean’s case “should be a real clarion call” for infectious disease specialists and other doctors in the U.S., said Joshua A. Lieberman, an infectious disease pathologist and clinical microbiologist who pioneered the leishmania-PCR test at the Washington state lab.
“If you’re worried about an unexplained [fever], you have to take a travel history that goes back pretty far and think about Southern Europe, Iraq, Afghanistan, India, and maybe even Brazil,” Lieberman said.
In the wake of Kean’s death, his family was told that Penn doctors held a meeting to analyze his case so they could learn from it.
An infectious disease doctor called Zinsky, Kean’s sister, to let her know about the postmortem review and shared that doctors discussed that Kean had likely picked up the parasite in Tuscany.
“Why didn’t you guys have this meeting,” she asked, ”while he was alive?”
Editor’s note: This story has been updated to clarify that ECRI President Marcus Schabacker was not speaking specifically on Kean’s case.
Robert E. Booth Jr., 80, of Gladwyne, renowned pioneering knee surgeon, former head of the Department of Physical Medicine and Rehabilitation at Pennsylvania Hospital, celebrated antiquarian, professor, researcher, writer, lecturer, athlete, mentor, and volunteer, died Thursday, Jan. 15, of complications from cancer at his home.
Born in Philadelphia and reared in Haddonfield, Dr. Booth was a top honors student at Haddonfield Memorial High School, Princeton University, and what is now the Perelman School of Medicine at the University of Pennsylvania. He was good at seeing things differently and went on to design new artificial knee joint implants and improved surgical instruments, serve as chief of orthopedics at Pennsylvania Hospital, and mentor celebrated surgical staffs at Jefferson Health, Aria Health, and Penn Medicine.
He joined with two other prominent doctors to cofound the 3B orthopedic private practice in the late 1990s and, over 50 years until recently, performed more than 50,000 knee replacements, more than anyone, according to several sources. Last March 26, he did five knee replacements on his 80th birthday.
In a tribute, fellow physician Alex Vaccaro, president of Rothman Orthopaedic Institute, said: “He restored mobility to thousands, pairing unmatched technical mastery with a compassion that patients never forgot.”
In a 1989 story about his career, Dr. Booth told The Inquirer: “It’s so much fun and so gratifying and so rewarding to see what it means to these people. You don’t see that in the operating room. You see that in the follow-ups. That’s the fun of being a surgeon.”
Dr. Booth was also praised for his organization and collaboration in the operating room. “His OR was a clinic in team work and efficiency,” a former colleague said on LinkedIn.
He told Medical Economics magazine in 2015: “I love fixing things. I like the mechanics and the positivity of something assembled and fixed.”
This article about Dr. Booth’s practice was published in The Inquirer in 2015.
His procedural innovations reduced infection rates and increased success rates. They were scrutinized in case studies by Harvard University and others, and replicated by colleagues around the world. Some of the instruments he redesigned, such as the Booth retractor, bear his name.
He was president of the Illinois-based Knee Society in the early 2000s and earned its 2026 lifetime achievement award. In an Instagram post, colleagues there called him “one of the most influential leaders in the history of knee arthroplasty.”
He was a professor of orthopedics at Penn’s school of medicine, Thomas Jefferson University Hospital, and the old Allegheny University of Health Sciences. He loved language and studied poetry on a scholarship in England after Princeton and before medical school at Penn. He told his family that his greatest professional satisfaction was using both his “manual and linguistic skills.”
He was onetime president of the International Spine Study Group and volunteered with the nonprofit Operation Walk Denver to provide free surgical care for severe arthritis patients in Panama, Guatemala, Honduras, Nicaragua, and elsewhere. Colleagues at Operation Walk Denver noted his “remarkable spirit, profound expertise, and unwavering commitment” in a Facebook tribute.
This story about Dr. Booth’s charitable work abroad appeared in The Inquirer in 2020.
At home, Dr. Booth and his wife, Kathy, amassed an extensive collection of Shaker and Pennsylvania German folk art. They curated five notable exhibitions at the Philadelphia Antiques Show and were recognized as exceptional collectors in 2011 by the Philadelphia Society for the Preservation of Landmarks.
He lectured widely about art and antiques, and wrote articles for Magazine Antiques and other publications. He was president of the American Folk Art Society and active at the Philadelphia Museum of Art, the Metropolitan Museum of Art in New York, and the Canterbury Shaker Village in New Hampshire.
“He was larger than life for sure,” said his daughter, Courtney.
Robert Emrey Booth Jr. was born March 26, 1945, in Philadelphia. He was the salutatorian of his senior class and ran track and field at Haddonfield High School.
Dr. Booth enjoyed time with his family.
He earned a bachelor’s degree in English at Princeton in 1967, won a letter on the swimming and diving team, and played on the school’s Ivy League championship lacrosse team as a senior. He wrote his senior thesis about poet William Butler Yeats and returned to Philadelphia from England at the suggestion of his father, a prominent radiologist, to become a doctor. He graduated from Penn’s medical school in 1972.
“I always liked the intellectual side of medicine,” he told Medical Economics. “And once I got to see the clinical side, I was pretty well hooked.”
He met Kathy Plummer at a wedding, and they married in 1972 and had a daughter, Courtney, and sons Robert and Thomas. They lived in Society Hill, Haddonfield, and Gladwyne.
Dr. Booth liked to ski and play golf. He was an avid reader and enjoyed time with his family on Lake Kezar in Lovell, Maine.
“He was quite the person, quite the partner, and quite the husband,” his wife said, “and I’m so proud of what we built together.”
Dr. Booth and his wife, Kathy, married in 1972.
In addition to his wife and children, Dr. Booth is survived by six grandchildren and other relatives.
A private celebration of his life is to be held later.
Donations in his name may be made to Operation Walk Denver, 950 E. Harvard Ave., Suite 230, Denver, Colo. 80210.
He was a surgical oncologist at a hospital in a Southern city, a 78-year-old whose colleagues had begun noticing troubling behavior in the operating room.
During procedures, he seemed “hesitant, not sure of how to go on to the next step without being prompted” by assistants, said Mark Katlic, director of the Aging Surgeon Program at Sinai Hospital in Baltimore.
The chief of surgery, concerned about the doctor’s cognition, “would not sign off on his credentials to practice surgery unless he went through an evaluation,” Katlic said.
Since 2015, when Sinai inaugurated a screening program for surgeons 75 and older, about 30 from around the country have undergone its comprehensive two-day physical and cognitive assessment. This surgeon “did not come of his own accord,” Katlic recalled.
But he came. The tests revealed mild cognitive impairment, often but not necessarily a precursor to dementia. The neuropsychologist’s report advised that the surgeon’s difficulties were “likely to impact his ability to practice medicine as he is doing presently, e.g. conducting complex surgical procedures.”
That didn’t mean the surgeon had to retire; a variety of accommodations would allow him to continue in other roles. “He retained a lifetime of knowledge that had not been impacted by cognitive changes,” Katlic said. The hospital “took him out of the OR, but he continued to see patients in the clinic.”
Such incidents are likely to become more common as America’s physician workforce ages rapidly. In 2005, more than 11% of doctors who were seeing patients were 65 or older, the American Medical Association said. Last year, the proportion reached 22.4%, with nearly 203,000 older practitioners.
Given physician shortages, especially in rural areas and key specialties like primary care, nobody wants to drive out veteran doctors with skills and experience.
Yet researchers have documented “a gradual decline in physicians’ cognitive abilities starting in their mid-60s,” said Thomas Gallagher, an internist and bioethicist at the University of Washington who has studied late-career trajectories.
At older ages, reaction times slow; knowledge can become outdated. Cognitive scores vary greatly, however. “Some practitioners continue to do as well as they did in their 40s and 50s, and others really start to struggle,” Gallagher said.
A few health organizations have responded by establishing late-career practitioner programs mandating that older doctors be screened for cognitive and physical deficits.
UVA Health at the University of Virginia began its program in 2011 and has screened about 200 older practitioners. Only in four cases did the results significantly change a doctor’s practice or privileges.
Stanford Health Care launched its late-career program the following year. Penn Medicine at the University of Pennsylvania also put in place a testing program.
Nobody has tracked how many exist; Gallagher guesstimated as many as 200. But given that the United States has more than 6,000 hospitals, those with late-career programs constitute “a vast minority,” he said.
The number may actually have shrunk. A federal lawsuit, along with the profession’s lingering reluctance, appears to have put the effort to regularly assess older doctors’ abilities in limbo.
Late-career programs typically require those 70 and older to be evaluated before their privileges and credentials are renewed, with confirmatory testing for those whose initial results indicate problems. Thereafter, older doctors undergo regular rescreening, usually every year or two.
It’s fair to say such efforts proved unpopular among their intended targets. Doctors frequently insist that “‘I’ll know when it’s time to stand down,’” said Rocco Orlando, senior strategic adviser to Hartford HealthCare, which operates eight Connecticut hospitals and began its late-career practitioner program in 2018. “It turns out not to be true.”
When Hartford HealthCare published data from the first two years of its late-career program, it reported that of the 160 practitioners 70 and older who were screened, 14.4% showed some degree of cognitive impairment.
That mirrored results from Yale New Haven Hospital, which instituted mandatory cognitive screening for medical staff members starting at age 70. Among the first 141 Yale clinicians who underwent testing, 12.7% “demonstrated cognitive deficits that were likely to impair their ability to practice medicine independently,” a study reported.
Proponents of late-career screening argued that such programs could prevent harm to patients while steering impaired doctors to less demanding assignments or, in some cases, toward retirement.
“I thought as we got the word out nationally, this would be something we could encourage across the country,” Orlando said, noting that Hartford’s program cost only $50,000 to $60,000 a year.
Instead, he has seen “zero progress” in recent years. “Probably we’ve gone backward,” he said.
A key reason: In 2020, the federal Equal Employment Opportunity Commission sued Yale New Haven over its testing efforts, charging age and disability discrimination. The legal action continues (the EEOC declined to comment on its status), as does the hospital’s late-career program.
But the suit led several other organizations to pause or shut down their programs, including those at Hartford HealthCare and at Driscoll Children’s Hospital in Corpus Christi, Texas, while few new ones have emerged.
“It made lots of organizations uncomfortable about sticking their necks out,” Gallagher said.
Instituting later-career programs has always been an uphill effort. “Doctors don’t like to be regulated,” Katlic acknowledged. Late-career programs have “in some cases been very controversial, and they’ve been blocked by influential physicians,” he said.
As health systems wait to see what happens in federal court, most national medical organizations have recommended only voluntary screening and peer reporting.
“Neither works very well at all,” Gallagher said. “Physicians are hesitant to share their concerns about their colleagues,” which can involve “challenging power dynamics.”
As for voluntary evaluation, since cognitive decline can affect doctors’ (or anyone’s) self-awareness, “they’re the last to know that they’re not themselves,” he added.
In a recent commentary in The New England Journal of Medicine, Gallagher and his co-authors recommended procedural policies to promote fairness in late-career screening, based on an analysis of such programs and interviews with their leaders.
“How can we design these programs in a way that’s fair and that therefore physicians are more apt to participate in?” he said. The authors emphasized the need for confidentiality and safeguards, such as an appeals process.
“There are all sorts of accommodations” for doctors whose assessments indicate the need for different roles, Gallagher noted. They could adopt less onerous schedules or handle routine procedures while leaving complex six-hour surgeries to their colleagues. They might transition to teaching, mentoring, and consulting.
Yet a substantial number of older doctors head for the exits and retire rather than face a mandated evaluation, he said.
The future, therefore, might involve programs that regularly screen every practitioner. That would be inefficient (few doctors in their 40s will flunk a cognitive test) and, with current tests, time-consuming and consequently expensive. But it would avoid charges of age discrimination.
Faster reliable cognitive tests, reportedly in the research pipeline, may be one way to proceed. In the meantime, Orlando said, changing the culture of healthcare organizations requires encouraging peer reporting and commending “the people who have the courage to speak up.”
“If you see something, say something,” he continued, referring to healthcare professionals who witness doctors (of any age) faltering. “We are overly protective of our own. We need to step back and say, ‘No, we’re about protecting our patients.’”
The New Old Age is produced through a partnership with The New York Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.