Paoli Hospital was not cited by the Pennsylvania Department of Health for any safety violations between April 2025 and March of this year.
Located in Chester County, the hospital is one of four owned by Main Line Health.
Here’s a look at the publicly available details:
June 18, 2025: Inspectors came to investigate a complaint but found the hospital was in compliance. Complaint details are not made public when inspectors determine it was unfounded.
June 19: The Joint Commission, a nonprofit hospital accreditation agency, renewed the hospital’s accreditation, effective April 2025, for 36 months.
Oct. 20: Inspectors came to investigate a complaint but found the hospital was in compliance.
March 12, 2026: Inspectors came to investigate a complaint but found the hospital was in compliance.
Unionized ChristianaCare doctors — members of the first healthcare union in Delaware — ratified their first contract with the Wilmington-based health system this week.
The contract covers three years and includes provisions to establish “formal structures for physician input on issues affecting clinical practice and patient care,” the union said in a statement.
The contract also establishes a procedure for physicians to file grievances if they feel the contract has been violated, and forms labor management committees to address workplace safety concerns, union officials said.
“This is a major step forward in ensuring physicians have a meaningful voice at ChristianaCare,” Nisha Gandhi, an advanced heart failure cardiologist at the health system, said in a statement.
A ChristianaCare spokesperson said the contract also included provisions against striking and “a mutual commitment to collaboration, stability and long-term partnership.”
ChristianaCare has medical locations in Delaware, Southeastern Pennsylvania, and Maryland.
Attending physicians at ChristianaCare voted to unionize in 2024, citing increased workloads with little support for added administrative tasks. They were the first group of attending doctors to unionize in the Philadelphia area.
Since the 1980s, doctors have shifted from owning their own practices to opting for employment at hospitals and health systems. Just a quarter of physicians were self-employed in 2022, and unionization among physicians is growing.
Last year, hundreds of medical residents across several Philadelphia hospitals also voted to unionize, but unions of attending physicians, who have completed their medical training, are rarer.
Pennsylvania health officialshave now detected measles cases in York and Northumberland Counties as cases in Lancaster County, the center of an ongoing outbreak, continued to rise.
And the state health department is now recommending early measles vaccinations for infants beginning at 6 months in affected areas in an effort to protect them against the spread of the highly contagious disease, which is particularly risky for young children. The same precautions should be taken by families with infants traveling to these areas.
Six Pennsylvania counties have now seen measles cases since an outbreak was first confirmed in Lebanon County in April. In all, the state has reported 81 measles cases across eight counties in 2026, more than five times the cases reported in 2025.
(function() {
var l2 = function() {
new pym.Parent(‘HE_MEASLES.html’,
‘https://media.inquirer.com/storage/inquirer/projects/innovation/arcgis_iframe/HE_MEASLES.html’);
};
if (typeof(pym) === ‘undefined’) {
var h = document.getElementsByTagName(‘head’)[0],
s = document.createElement(‘script’);
s.type = ‘text/javascript’;
s.src = ‘https://pym.nprapps.org/pym.v1.min.js’;
s.onload = l2;
h.appendChild(s);
} else {
l2();
}
})();
State health officials said it was too early to tell how the latest cases in York and Northumberland Counties are connected to others in the region, but that contact tracing investigations are continuing. All cases were among people who had not received at least two doses of the measles, mumps, and rubella (MMR) or whose vaccination status was unclear.
As of Wednesday, six cases had been confirmed in Northumberland County, to the north of Dauphin County, and one case had been detected in York County, along Lancaster’s western border.
Lebanon County has reported 20 cases and Dauphin and Berks Counties have reported two cases each.
Lancaster County has seen 38 cases of measles since late April, with health officials confirming seven cases in the last two weeks. The area was at the center of a prior measles outbreak in January, when state health officials confirmed eight cases in Lancaster County and an additional four between Chester and Montgomery Counties.
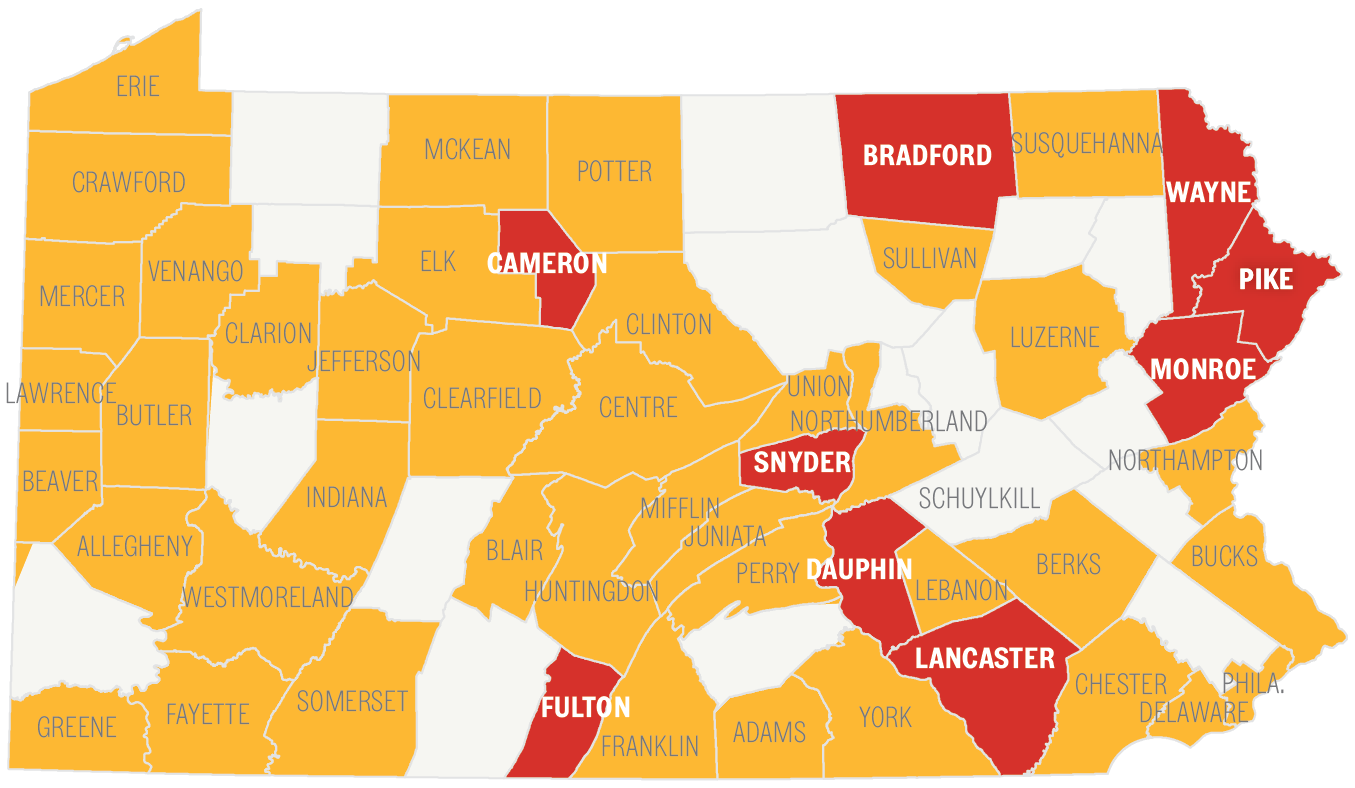
Vaccination rates among kindergarteners have decreased across Pennsylvania in recent years, and some counties affected in the current outbreak have particularly low rates, including Lancaster, where about 88.5% of kindergarten students are vaccinated. Health experts say that 95% of a community must be vaccinated to prevent the spread of the disease.
A map showing vaccination rates in kindergarteners for the 2024-2025 school year. Counties in yellow have vaccination rates between 95% and 90%. Counties in red have vaccination rates below 90%. To halt the spread of measles, at least 95% of a community must be vaccinated against the disease.
Health officials have been conducting contact tracing to detect as many cases as possible. In the current outbreak, they have twice warned Lancaster residents that they could have been exposed to measles.
Shoppers and employees at a local Kohl’s were potentially exposed to the virus over four days after a staffer tested positive in late May, LancasterOnline reported. And a person with measles visited the Lancaster County Courthouse on June 3.
But doctors in Lancaster County say they fear some measles cases are going unreported, either because patients don’t understand the importance of tracking measles cases or because they fear repercussions.
No cases have been confirmed in the Philadelphia region during this outbreak. But Delaware County health officials said last week that they had detected measles in two wastewater samples, indicating that someone with measles had used a bathroom connected to the county’s public water supply. It was unclear if that person lived in the county or was passing through.
Measles can infect nine in 10 unvaccinated people who are exposed to it, and can linger in the air for up to two hours and incubate in patients for three weeks. The disease typically presents with a fever and a rash but can cause brain inflammation and pneumonia in serious cases.
Typically, children receive the first of two MMR vaccines at 1 year old, then a second between 4 and 6 years old.
But children as young as 6 months can receive an additional “dose zero” to protect them from the disease amid an outbreak. In its alert, the state health department said parents should vaccinate infants between 6 and 11 months with the “dose zero” if they live in affected areas or if they’re planning to travel there.
Those children should then receive additional MMR doses at 12 to 15 months and 4 to 6 years.
This “dose zero” is less effective than doses given at 1 year old, officials cautioned. But it’s 58% effective against measles when given at 6 to 8 months, and 83% effective when administered at 9 to 11 months.
“Early MMR vaccination is safe and provides modest protection when measles is spreading,” officials wrote in the alert.
Children older than 12 months who haven’t been vaccinated should get an MMR dose immediately, and a second 28 days later, health officials said. Unvaccinated adults, or those without evidence of immunity, should also get two MMR doses.
And anyone who has received one dose of the MMR vaccine in the past should get a second at least 28 days after their first, officials said.
Usually, children who received a first dose at around 12 months wait to get their second dose until they’re 4 to 6 years old. But in an outbreak situation, those children should get their second doses early — at least 28 days after their first shot.
Adults born before 1957 are typically considered immune, but healthcare workers in that age group who don’t have lab evidence of immunity or prior infection should consider getting vaccinated, state officials said.
Adults who received an inactivated measles vaccine between 1963 and 1967 are considered unvaccinated during an outbreak, and should also get two doses of the current MMR vaccine.
Pregnant people, people with severely weakened immune systems, and people who have a history of experiencing severe allergic reactions, like anaphylaxis, to a vaccine ingredient or to a previous dose of MMR cannot receive the vaccine.
Merakey USA, based in Lafayette Hill, is acquiring Boundless, an Ohio nonprofit that provides services for people with intellectual and developmental disabilities and behavioral health needs, in a deal that leaders of both organizations described this week as a model for their industry.
“It’s the marriage of two financially stable organizations” that are preparing for turbulence in the human services sector, said Merakey CEO Joseph S. Martz. More typically human services deals happen because one nonprofit needs a financial rescue, as happened with Philadelphia’s Resources for Human Development in 2024.
Merakey and Boundless planned to announce the news Thursday.
Martz and the CEO of Boundless, Patrick Maynard, both said the size of the combined organization — more than $1 billion in revenue — would enable it to invest in the systems, technology, training, and workforce development needed to be financially sustainable.
The deal, expected to close in July, will create an organization that supports 50,000 individuals and families annually in 12 states and employs 11,000 people.
Joseph S. Martz is CEO of Merakey USA, which is acquiring Boundless, a human services provider based in Columbus, Ohio.
The executives cited pressures from an expected change in how their organizations get paid. A shift is underway to payment for results rather than for straight volumes of services. Looming cuts to Medicaid over the next decade are also forcing human services providers to rethink how they operate.
“We’re entering a time when resources are going to be a lot tighter, and I think organizations need to be thinking differently about how they approach that. We’re seeing some other pretty large consolidations,” said Chuck Ingoglia, CEO of the National Council for Mental Wellbeing, a Washington nonprofit advocacy group.
Origins of the Merakey-Boundless deal
Stacy DiStefano, CEO of Consulting for Human Services, a Philadelphia-based adviser firm, introduced Martz and Maynard to each other in July 2024.
That led to a series of conversations about issues the two organizations were spending money to solve and the realization: “Why don’t we just come together and use the combined resources of our organizations to solve that problem,” Martz said.
Merakey and Boundless had already been growing through acquisitions, though Boundless has grown more dramatically. In the last seven years, the nonprofit made five acquisitions that helped increase its annual revenue to an expected $200 million this year from $20 million, Maynard said.
“My goal was to create sustainability in a broken system where most of us are living off of Medicaid, which comes nowhere close to providing the resources that cover the costs,” Maynard said.
Patrick Maynard is CEO of Boundless, a Ohio human services provider that is merging into Merakey USA, of Lafayette Hill.
The added scale enabled Boundless to add healthcare and dentistry for its clients, but the Medicaid shortfall for those dental services is $75,000 a month, Maynard said. That kept Maynard looking for even bigger partners, like Merakey.
Maynard cited Merakey’s expenditure of $18 million for Workday software, a system for human resources and financial management as an example of something Boundless could never afford. At $200 million in annual revenue, Boundless struggled to spend $2 million on a system for electronic health records, he said.
A new structure
Merakey, which started as the Northwest Center in the Mount Airy section of Philadelphia in 1969, remains firmly rooted in Pennsylvania. The state is expected to account for more than half its $850 million in revenue for the fiscal year that ends this month, Martz said.
States where Merakey operates include Indiana, Kentucky, Ohio, Michigan, and Wisconsin. A new division called Boundless Midwest, led by Maynard, will assume responsibility for Merakey’s operations in that region when the deal is done.
Both boards have approved the transaction, which remains under review by the Ohio Attorney General.
Martz said he expect Boundless to continue growing though acquisitions and the development of new programs with the support of Merakey.
“We are going to be a big organization, but it’s really about being a better organization, about the quality of care that we provide,” Martz said. “If you’re not culturally aligned, bigger for bigger sake, just doesn’t make any sense to me.”
Main Line Health and UnitedHealthcare have an “agreement in principle” on new contract and will extend the current contract until the new deal is completed, Main Line Health said Wednesday.
Main Line’s contract with United was set to expire Tuesday, potentially disrupting care for 32,000 people who rely on Main Line doctors and have health insurance through United. The negotiations covered employer-sponsored plans and Medicare Advantage plans.
“For nearly a year, Main Line Health worked diligently and in good faith to reach a responsible agreement — one that reflects the true cost and complexity of the high-quality care we deliver to this community every day. We are pleased to have reached this milestone, and our patients will experience no disruption to their care,“ Main Line said in an email.
Main Line said the preliminary agreementrelieves some of the administrative burden for doctors and patients. They include prior authorization delays, claim denials, and excessive audit activity, Main Line said.
United, the nation’s largest health insurer, did not immediately provide a comment.
The company based in Eden Prairie, Minn., this year failed to reach a new agreement with Jefferson Health’s Lehigh Valley Health Network for Medicare Advantage and employer plans. That outcome added to the worry for some patients that the same thing would happen in Philadelphia’s western suburbs, where Main Line is the leading provider of healthcare services.
Project HOME is adding 20 beds to a Hunting Park shelter to house hospital patients who have nowhere to go once they’re discharged.
The new center, Hawthorne House Respite, expands the respite beds available at the housing nonprofit’s Sacred Heart Recovery Residence on Old York Road.
Renovations to the building, a former nursing home for cancer patients run by Dominican nuns, added 20 beds in dormitory-style housing — 10 for men, 10 for women — and cost $3.4 million. Funds came in part from $2.3 million raised at the behest of Jon Bon Jovi, a longtime Project HOME collaborator, at the organization’s 35th anniversary gala in 2024.
“We can’t stress enough how much housing is healthcare, and that respite beds at every level is so important as part of the ecosystem,” said Donna Bullock, Project HOME’s CEO, after a ribbon-cutting ceremony for the new beds Wednesday.
“People need different levels of care for healing, different levels of housing for stability.”
Sacred Heart, which also offers longer-term housing for people in recovery, already had 10 respite beds for residents.
Now, providers can refer more patients directly from the hospital to Sacred Heart. The program is part of the Project HOME Collaborative, a partnership to address homelessness and substance use recovery with Jefferson Health, Penn Medicine, Temple Health, and Prevention Point.
Project HOME officials say respite beds are in high demand and short supply across Philadelphia. Another respite program run by the Public Health Management Corporation in northwest Philadelphia offers 40 beds for patients with higher-level medical needs.
“It’s not enough,” Bullock said.
Gaps in the healthcare, shelter, and addiction treatment systems often make it difficult for homeless patients to heal after a hospital stay.
Inpatient addiction rehabs and shelters often do not have the capacity to care for patients with ongoing medical needs, while hospitals cannot sustain long-term care for patients who have recovered enough to be discharged.
“We know that recovery doesn’t stop when we discharge you and send you out into the community. Too often, individuals who are homeless face impossible challenges after they are discharged,” said Steve Carson, Temple Health’s senior vice president of population health.
Patients placed in respite beds say such programs are crucial to their recovery and continued stability. Amber Moon arrived at Sacred Heart two years ago after she developed endocarditis from injection drug use, resulting in two heart surgeries.
After months in the hospital, she was well enough to leave — but still needed support to heal. At Sacred Heart, staff arranged rides to doctors’ appointments and helped her navigate new medication regimens. Moon relished the opportunity to continue her recovery outside of a hospital room, surrounded by other residents who’d survived similar experiences.
“I was happy that I was around other people — not just the girls that I was staying with, but staff that understood what I was going through,” she said. “They treat you with humanity, like a regular person.”
Now a certified recovery specialist who helps other people with addiction navigate treatment, Moon is set to move into her own apartment soon.
“I‘m very grateful to have met all the people I’ve met, and been through what I’ve been through, because now I’m able to help others who think that there’s no chance,” she said. “There always is.”
Bill Curry, 65, raises cattle on the same land in rural Oklahoma once owned by his father and generations before him. Each quarter, for several years, he has made the 2½-hour drive to Oklahoma City for an epidural in his spine to treat his back pain.
But this year, because of a new Medicare program, Curry has traveled a little more often.
In February, during one trip, he was told unexpectedly that he needed preapproval for the procedure. Then he went again a month or so later to get the injection, for a total of 10 hours on the road. His clinic wanted him to come in a third time, which they had never asked of him before. That appointment was “just to fill out a piece of paper to tell them how you feel again,” Curry said, so he hasn’t gone.
In January, Oklahoma became one of six states to begin a pilot program testing the use of pre-approvals in traditional Medicare, the federal health insurance program for people 65 and older or with disabilities. Medicare had previously eschewed the practice — also known as prior authorization — which requires patients or someone on their medical team to seek insurance approval before proceeding with certain procedures, tests, and prescriptions.
Epidurals like Curry’s are among 13 medical services subject to the new program because the Trump administration says they’re prone to fraud or misuse. Powered by artificial intelligence, the program — called the Wasteful and Inappropriate Service Reduction Model, or WISeR — is intended to save the federal government money and protect patients from potentially unsafe or unneeded care.
Yet early reviews from Oklahoma and the other pilot states — Arizona, New Jersey, Ohio, Texas, and Washington — suggest WISeR’s rollout has not been smooth. Patients, doctors, and other healthcare professionals who spoke with KFF Health News say the effort has created confusion, errors, long wait times, and stress. Some described the rollout as “horrendous” and say people enrolled in Medicare in the pilot states are now getting ensnared in the same red tape as those with private insurance.
One key concern is that it all happened too hastily. WISeR was announced in June 2025 and launched in mid-January.
That was “quicker than normal” for the federal government, said Todd Baker, who recently stepped down as CEO of the Ohio State Medical Association. Doctors “just sort of had to figure it out,” added Jeb Shepard, director of policy at the Washington State Medical Association.
Government contractors have also acknowledged the rapid pace. “We’ve had an aggressive rollout from the time of being notified to going live,” said Jeremy Friese, CEO of Humata Health, the vendor for Oklahoma. Tech executives servicing other states have said they were still adding features to their products in the spring.
Abe Sutton, director of the Center for Medicare and Medicaid Innovation, which is administering the program, didn’t comment on the rollout schedule. But he said in a statement that the goal of these reforms is to ensure that prior authorization is efficient, fast, and streamlined.
“The model aims to reduce inappropriate care without delaying appropriate care,” he said.
Mehmet Oz, the leader of the Centers for Medicare & Medicaid Services, told NewsNation in December that they were “rolling out some prior authorization on abused practices.”
“The purpose of these is not to deny care,” Oz continued. “It’s to make sure you get the care you need and deserve, not the care some unscrupulous doctor wants to use on you.”
Medicare has struggled in recent years with suspected fraud associated with particular services. The Department of Health and Human Services’ inspector general warned in September that the program’s spending on skin substitutes, for example, had surged nearly 700% over two years, raising “major concerns about fraud, waste, and abuse.” Skin substitutes are among the 13 therapies currently subject to review under WISeR.
The program also imposes prior authorization requirements for kyphoplasty, a surgery for spinal fractures, which a report by the Medicare Payment Advisory Commission flagged as overused.
Sutton acknowledged, however, that “the percentage of providers committing waste, fraud, and abuse is small.”
Consumers and clinicians largely detest prior authorization. Even as federal health officials test the process for Medicare, the Trump administration is trying to scale it back for those with private insurance. According to a KFF poll conducted in January, 69% of insured adults consider prior authorization a burden for care.
Through WISeR, doctors and their staff log in to online portals to submit medical records that justify the procedures. Using artificial intelligence, the systems quickly approve applications that meet the program’s criteria, Friese, Humata’s chief executive, told KFF Health News. He said there is an “immediate yes” in 88% of cases for which clinical data supports an approval.
CMS has touted the process as one in which decisions are returned within 72 hours. After that, clinicians receive a “universal tracking number,” which allows them to schedule the procedure and get paid. In practice, however, participants say the process is anything but easy.
The University of Washington’s medical system alone had nearly 100 patients waiting earlier this year for epidural injections due to WISeR-related delays, according to an April report from the office of U.S. Sen. Maria Cantwell (D-Wash.) that drew on hospital association data. “Now, patients are subject to delays or denials which did not exist prior to the WISeR Model,” the report said.
FILE – Sen. Maria Cantwell, D-Wash., speaks on Capitol Hill in February. (AP Photo/Tom Brenner, File)
Curry, the Oklahoma cattle farmer, said he might go to Kansas for future treatments to avoid the approval process. Dorota Gribbin, a New Jersey-based physical medicine and rehabilitation physician, said that by the time authorization came for one of her patients who needed a back pain procedure, the patient had gone to the hospital for more expensive care.
Jennifer Valle, a precertification and insurance supervisor at Clinical Radiology of Oklahoma, said when it comes to kyphoplasties, there has been a lot of “nitpicking” from reviewers. Other times, information her practice provides to CMS gets overlooked, she said, and reviewers ask for imaging that’s already in the file.
Claims with no problems are supposed to be paid within 15 days, said James Webb, a musculoskeletal radiologist in Tulsa, Okla., who has also been frustrated by the prior approval and reimbursement process for kyphoplasties. “Six- to eight-week delays is what we’ve been seeing,” he said.
“It’s been horrendous,” said Jerry Sobel, a Phoenix-area pain management doctor. “Right from the beginning, there seemed to be no organization.” Sobel said that as of May, he hadn’t gotten paid by Medicare for nine epidurals.
“We continuously monitor operations and work closely with stakeholders to address questions and improve the provider experience,” said Sundar Subramanian, the CEO of Zyter, which has the contract for Arizona.
During an April webinar, another Zyter executive acknowledged a large backlog in payments stretching to January. Those backlogs “are currently being resolved,” Medicare’s Sutton said, without providing further detail.
When asked about other issues — including what doctors suspect are AI-driven errors — Medicare’s Sutton said the agency appreciates “feedback on provider experience.” It will be used “to help providers better understand WISeR processes,” he said.
Although CMS vendors say humans make the final decisions on approvals, doctors and their staffs believe artificial intelligence is playing a large role in the process and that denials are sometimes the result of AI hallucinations that garble or make up information.
One Arizona doctor, who wasn’t authorized by his practice to speak, recalled a denial saying his patient wasn’t eligible for procedures in the thoracic region, or midback. The patient needed an injection to the neck. Webb, the Oklahoma radiologist, documented four times that a patient lacked numbness, and yet his WISeR application was still denied, citing numbness, which, in the reviewer’s interpretation, would rule out the spinal surgery procedure.
Friese, Humata’s CEO, said he hasn’t heard about any AI hallucinations.
The process is also raising government costs. With more rejections, more appeals are being filed with Medicare’s administrative contractors. The government pays the contractors to handle the appeals, and Medicare’s Sutton acknowledged that the agency has “accounted for potential changes in the volume of Medicare appeals because of the WISeR program and its associated costs.”
Eighty-four percent of commercial insurers already use AI tools, according to a survey released in 2025 by the National Association of Insurance Commissioners, though they have consistently said AI isn’t used to deny prior authorization requests.
Its use in Medicare risks introducing friction and frustration into the program — and piling costs onto its beneficiaries. Prior authorization saves money for insurers partly by making patients pay a price in wait times and inconvenience, said Miranda Yaver, a University of Pittsburgh health policy researcher studying the technique.
“People will end up getting ensnared in a lot of red tape, having to be on hold, and getting rerouted,” she said. She often wonders whether prior authorization simply shifts costs to patients and doctors, rather than saving them.
Some doctors involved in Medicare’s prior authorization experiment believe it will inevitably expand beyond a few services officials in Washington consider fraud-prone.
“Everybody knows that if this pilot project works, it will be prior auth for basically all procedures,” said Mary Clarke, a family practice physician in Stillwater, Okla. “If they can show that they can save money, then that’s going to be extrapolated and rolled out to other procedures and multiple other things in other states.”
When asked whether CMS is considering expansion of its prior authorization pilot, Sutton said in his statement that there are “currently no changes” considered for the list of services subject to the WISeR program, “but CMS continues to assess whether any changes are warranted.”
KFF Health News Southern correspondent Lauren Sausser contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
A group of Rutgers researchers led by neuroscientist Ioana Carcea want to learn more about how women’s brains are affected by pregnancy, motherhood, menopause, and other hormonal changes that they say have been under studied.
The Women’s Brain Health Initiative at the Rutgers Brain Health Institute in Piscataway will focus on research and public education about women’s brain function, neurodevelopment, mental health, and disease vulnerability.
The Inquirer spoke with Carcea, associate professor in the Department of Pharmacology, Physiology and Neuroscience at Rutgers New Jersey Medical School, to learn more about the initiative, which launched in June.
The interview has been lightly edited for clarity and length.
Ioana Carcea is an associate professor in the Department of Pharmacology, Physiology and Neuroscience at Rutgers New Jersey Medical School.
What is the focus of your research and the Women’s Brain Health Initiative?
In my laboratory we study different aspects related to how the brain works, how it communicates with the body. One focus area for us is understanding maternal behavior and what regulates maternal behavior. The institute is much broader than what I do. In the Rutgers Women’s Brain Health Initiative, we want to focus on the transitions in life that are specific to women — puberty and monthly menstruation, pregnancy, postpartum, menopause. These are very dramatic hormonal changes that women experience and they impact general health, particularly brain health.
How are the hormonal changes women experience different from men?
Men obviously experience puberty, but it’s a different set of hormones. Post-puberty, testosterone does have a full cycle mode of release, but it’s not the monthly cycle that women experience in hormone levels, and the fluctuations are not as profound as in women. Then with aging, men don’t really experience a “pause.” There is going to be a decrease in testosterone levels with aging, but it’s not a complete pause like we see in women.
What are some of the challenges in this type of research?
It is a difficult topic to study. Menopause varies among women, as far as when it starts, how long the perimenopause period lasts — it can be two years, it can be 10. The symptoms vary, genetic risks can amplify the risk of disease. Another challenge is we don’t really have great animal models for menopause. Menopause is very rare in nature. Other than women, only orcas and some other whales have true menopause, where they can lead healthy lives after the reproductive window closes. Primates can come close to menopause – it’s not quite the same, but they do experience reproductive aging.
Has research funding been a challenge?
We need more funding in this area. The funding climate has been changing and both NIH and private foundations are now investing more in women’s brain health research, but that hasn’t happened for a long time, and I think that’s one of the reasons we have these gaps in knowledge when it comes to women’s brains.
A COVID vaccine study that the CDC’s chief halted this spring over methodological concerns was published Tuesday in JAMA Network Open, a leading peer-reviewed medical journal.
The analysis used the same methodology that CDC’s interim director had criticized when the paper was not allowed to be published in the weekly scientific report of the Centers for Disease Control and Prevention.
The study, which had been slated for publication in March in the CDC’s Morbidity and Mortality Weekly Report, found that the COVID-19 vaccine reduced the risk of emergency department visits and hospitalizations among healthy adults by about half last winter. The findings were consistent with what researchers have found in past years, that the vaccine can help reduce the risk of severe illness in adults even after accounting for immunity from prior vaccination or infection.
“Science was never the issue,” said Michelle Barron, one of the study’s authors and senior medical director of infection prevention and control for UCHealth, a nonprofit health system in Colorado. “Certainly it was within [the CDC’s] purview to keep it out, for whatever reason, but it was clearly not for scientific reasons that the study was withheld from publication in the MMWR.”
Jay Bhattacharya questioned the study’s methodology. (AP Photo/Julia Demaree Nikhinson)
Jay Bhattacharya, CDC’s interim director, delayed publication of the study before it was subsequently not published in the MMWR at all, The Washington Post previously reported. Bhattacharya had concerns about the methods used to calculate vaccine effectiveness, a Health and Human Services spokesman said at the time.
Barron said she believed the study was not published because the findings did not support Health Secretary Robert F. Kennedy Jr.’s agenda that wants to limit the use of COVID vaccine specifically.
Kennedy, the founder of a prominent anti-vaccine group, has been an outspoken critic of COVID shots, once referring to them as the “deadliest vaccine ever made.”
A spokeswoman for the Health and Human Services Department did not directly address the author’s allegation Tuesday that the paper was withheld because it conflicted with the administration’s vaccine agenda. Spokeswoman Emily Hilliard said the CDC evaluates studies using rigorous scientific methods and reviews methodological concerns before publication.
“The CDC does not make scientific determinations based on predetermined conclusions,” Hilliard wrote in an email. “We evaluate the weight of evidence using rigorous methods, communicate uncertainty and limitations, and subject our work to scientific scrutiny before publication.”
A commentary accompanying Tuesday’s JAMA Network Open report said the methodology in question, known as test negative design, has limitations, like any study. But those shortcomings are well understood, actively studied, and outweighed by the method’s practicality for routine vaccine-effectiveness monitoring, wrote Natalie Dean, associate professor of biostatistics and epidemiology at Emory University’s Rollins School of Public Health.
“This is not a controversial study design — this is [the] same design that has been churning out vaccine results for a long time,” Dean wrote in an email. “And from a highly experienced group — CDC plus a network of top vaccine researchers across the country. They are a well-oiled machine.”
She added: “There was no scientific reason to reject this paper. It had undergone internal review, and it clearly meets the standards of peer-reviewed science. It makes my colleagues on edge to see political interference in the scientific process.”
Dean said the methodology is being “unfairly maligned” and worried that efforts to discard it could weaken the nation’s vaccine surveillance system. “Then we’ll be flying blind with respect to influenza, COVID, and RSV vaccine monitoring,” she said.
Between September and December last year, healthy adults who received the COVID-19 vaccine reduced their likelihood of emergency department and urgent care visits by 50% and cut the likelihood of COVID-associated hospitalizations by 55%, compared with those not receiving a 2025-26 vaccine dose, the report found.
Researchers analyzed data from a CDC-funded surveillance network to compare data on adults who sought medical care for COVID-like symptoms and compared outcomes between those who received the updated 2025-26 vaccine and those who had not.
No parent should lose sleep over a condition that doesn’t exist.
Yet every summer, viral headlines resurface the myth of “dry drowning,” the misleading belief that a child can suddenly die days after a normal swim from water hidden in their lungs.
As a pediatric emergency room doctor, I know these rumors are not harmless. Terms like “dry drowning” create anxiety about letting children enjoy the water. They also generate false expectations about the need for long-term vigilance after swimming. Instead, we must help families recognize the real signs of respiratory distress after a water incident.
Water play and swimming are fun ways for kids to stay cool and active in the summer, but water safety should always come first. Drowning is the No. 1 leading cause of death in children 1 to 4 years of age in the U.S., and a major risk for older children as well. Inaccurate information can distract from proper prevention, recognition, and treatment, so we must understand the facts to stay safe around water.
What is drowning?
Drowning occurs when water gets in the way of normal breathing. This can happen quickly (in under 30 seconds) and silently; most kids do not scream and splash like in the movies. Drowning is not always fatal; symptoms can present or persist after a child gets out of the water but they occur shortly after the event, not days later.
Symptoms of drowning include coughing, trouble breathing, chest pain, vomiting, pale or blue-appearing skin, or being unusually sleepy, irritable, or less interested in playing. These symptoms occur as a result of the body’s natural response to drowning; the body tries to clear water from the windpipe and lungs through protective reflexes like coughing before critical organs like the heart and brain suffer from a lack of oxygen. Children who develop concerning symptoms should be promptly evaluated by a medical professional.
Drowning can occur in either salt water or fresh water, or any kind of liquid. And it doesn’t just happen in oceans and pools; young children have drowned in bathtubs, buckets, and even toilets. All it takes is a few inches of water.
Why is ‘dry drowning’ a myth?
“Dry drowning” — the idea that a child can look well after a water incident and then deteriorate days later without warning due to water in their lungs — doesn’t exist. Drowning by definition requires breathing issues caused by water. Since oxygen is necessary for life, the body does not wait days before telling you that something is awry.
So how long should parents monitor their child? Multiple analyses of drowning events have shown that symptoms occur immediately or shortly after water exposure — usually within eight hours. If water reaches the lungs, it can trigger inflammation that may take several hours to become apparent. A child who is acting like their normal self is unlikely to develop symptoms from drowning beyond this initial period.
If we recognize drowning and intervene quickly, we can help a child before breathing issues can lead to organ failure and death. The effects of non-fatal drowning range from no injury at all to severe complications, including brain damage or permanent disability. Swift action, however, can help limit the long-term consequences.
If a child gets sick days after playing in the water, they haven’t drowned, but they still need to be seen by a healthcare professional to be evaluated for other serious conditions.
How to prevent drowning
I once cared for a young child who wandered out of her house without her parents noticing, only to be found unconscious in her neighbor’s unfenced pool. Kids are naturally curious and want to explore the world; it is up to us to keep them safe. Using multiple layers of protection can greatly reduce the risk of drowning:
Swim lessons: Swimming is a life skill; the American Academy of Pediatrics recommends that all children start swim lessons after their first birthday. Similar to putting on your own oxygen mask before helping others in an airplane emergency, supervising adults should know how to swim so they can help others. Check out classes in Philadelphia and the surrounding area for you and your children.
Properly fitted life jackets: Small children and weak swimmers should wear U.S. Coast Guard-approved life jackets whenever they are near water, including pools and waterparks. Everyone should wear a life jacket when boating or participating in water-based activities in open water, such as lakes, rivers, and oceans. Inflatable aids like “floaties” are not safe substitutes as they can deflate and do not prevent drowning. Refer to the U.S. Coast Guard brochure for guidance on choosing a properly fitted life jacket.
Four-sided pool fencing with a self-latching gate: Fencing that surrounds pools decreases the risk of drowning by a whopping 83% compared to three-sided fencing or no fencing. Barriers should be a minimum of four feet high, and avoid horizontal bars, chain links, or nearby patio furniture that children could easily climb.
Close supervision:Even with a lifeguard present, adults should closely supervise infants, toddlers, and noncompetent swimmers at all times when near water, staying within arm’s reach and avoiding distractions like phones, socializing, or alcohol. This applies to bathtubs, buckets, and toilets as well. Caregivers should always clearly hand off supervision responsibilities.
Emergency preparedness: Parents, caregivers, and pool owners should be CPR trained in case of an emergency. Older children and adolescents can learn too. For the patient I cared for, CPR saved her life. A year later, she is thriving with no residual deficits.
With the right precautions, we can help kids enjoy the water safely all summer long. Talk to your pediatrician or visit CHOP Pediatric Health Chat whenever you have questions about kids’ health.
Priya Shah is a fellow physician in Pediatric Emergency Medicine at Children’s Hospital of Philadelphia. She earned her medical degree from Harvard Medical School and is board-certified in General Pediatrics. Her work focuses on child injury prevention.
The views expressed in this article are those of the authors and not necessarily those of CHOP. This information is not intended to provide medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional regarding any health or medical concerns.