A Philadelphia-area infant named Baby KJ made international headlines after doctors at Children’s Hospital of Philadelphia and Penn Medicine successfully treated his rare, life-threatening liver condition with a gene-editing drug earlier this year.
Now back home with his family in Drexel Hill after more than 300 days in the hospital, KJ Muldoon has been named one of 10 people who helped shape medicine in 2025 by Nature, a British scientific journal.
Nature’s 10 is rounded out by career scientists and public health champions, including a neurologist treating brain disorders, an entomologist unearthing new details about mosquito-borne illnesses, and a data researcher who drew attention to troubling patterns in research retractions. The publication honored Baby KJ as a “trailblazing baby.”
KJ was born with a rare disorder that prevented his liver from processing protein. He was at risk of dangerous levels of ammonia, a byproduct of protein, building up in his bloodstream, traveling to his brain, and causing irreparable damage. The condition, called severe carbamoyl phosphate synthetase 1 (CPS1) deficiency, is deadly in more than half of cases.
With few treatment options and limited time, KJ’s doctors proposed a novel treatment using experimental gene-editing technology: They would analyze KJ’s genetic profile to find the genetic mutation that prevented his body from producing a key enzyme that breaks down protein. Then they would infuse a medication laced with bits of genetic code to find the misspelling and fix it, dramatically improving his chances of recovery.
Within six months, researchers at CHOP and Penn had developed a customized drug specifically for KJ using CRISPR, the buzzy shorthand for a scientific tool that works like a find-and-replace command. It is named after a stretch of genetic code utilized — clustered regularly interspaced short palindromic repeats.
KJ received three doses of the medication, and in June, he returned home after 307 days in the hospital. He will need ongoing care, but doctors say the treatment has dramatically improved his liver function.
“This is the future of medicine, a step toward using gene-editing for diseases for which there are few treatments,” Kiran Musunuru, director of the Penn Cardiovascular Institute’s Genetic and Epigenetic Origins of Disease Program and one of the lead doctors on KJ’s case, said during a call with reporters in May.
Baby KJ’s treatment was a first-of-its-kind drug customized to a unique genetic mutation. It will never be used for another patient, but Philadelphia researchers believe the CRISPR framework could be used to customize drugs for other patients.
Musunuru and Rebecca Ahrens-Nicklas, the director of CHOP’s Gene Therapy for Inherited Metabolic Disorders Frontier Program, are developing a new clinical trial to test the CRISPR framework for treating customized gene therapies for urea cycle disorders related to any one of seven genes.
The mechanism will remain the same, but the injection each patient receives will be customized to target their unique genetic mutation.
They are hopeful that their work will make bespoke treatments available to more people with rare diseases, Ahrens-Nicklas told Nature.
“Everyone saw the possibility and thought, ‘Why isn’t this available for my child?’”
Wistar Institute scientist Maureen Murphy wants to solve a decades-long mystery: Why is ovarian cancer often resistant to hormone therapy?
In a recently published study, she shared a new theory as to why treatments designed to block or remove hormones, known as hormone therapy, often fail in ovarian cancer — and a potential approach to make them more effective. Such therapies have cut the risk of death from certain breast cancers by a third and reduced the odds of a recurrence by half.
She pinpointed a problem facing hormone therapy — the vast majority of ovarian cancer cases have mutations in a key protein called p53.
Her study, published last month in the medical journalGenes and Development, suggests that mutations in p53, a protein that normally works to stop tumors from growing, drive resistance to hormone therapy and that their effects could be reversed.
“There are very few drugs that treat it,” Murphy said.
Her p53 mutation discovery led to her identifying a drug currently in clinical trials that’s promisingin a small number of cases. Murphy wants doctors to start testing the combination of the drug and hormone therapy in ovarian cancer.
If the approach makes it into a clinical trial, it would still take years to evaluate the safety and efficacy of the combination. Most treatments tested in clinical trials do not become standard practice.
“For ovarian cancer, the treatment hasn’t changed much in the last 20 years, and so we really do need new treatments,” Murphy said.
How does hormone therapy work?
Hormones are like the body’s mail service.
These chemicals carry messages to cells throughout the body, controlling mood, growth, reproduction, and development.
Tumors can co-opt hormones for their own purposes using proteins called receptors, which act like mailboxes to receive the messages.
Breast cancers, for example, often have estrogen receptors so that they can receive more of a hormone called estrogen. Similar to how bodybuilders use steroids to build muscle, tumors use estrogen to grow and divide.
“Breast and ovarian tumors love estrogen. They grow on it,” Murphy said.
Hormone therapy works by either blocking the receptors from receiving the hormones, or reducing the amount of hormones in the body altogether.
One of the first hormone therapy drugs for cancer, tamoxifen, was approved in the U.S. in 1977 to target the estrogen receptor in metastatic breast cancer.
In this study, Murphy looked at fulvestrant and elacestrant, two anti-estrogen drugs approved for breast cancer.
More than 70% of cases of the most common type of ovarian cancer express estrogen receptors, making them theoretically a good target for hormone therapy, if the p53 problem can be fixed.
Solving the mystery
In her first professor job at Temple’s Fox Chase Cancer Center in 1998, Murphy chose to study the tumor suppressor protein p53, with a focus on genetic variants in women of African and Ashkenazi Jewish descent that put them at risk of cancer.
Decades later, Murphy expanded her focus at Wistar to look at hundreds of genetic variants of the protein found in the general population, in an effort to predict people’s risk of cancer.
Murphy started to wonder whether mutant p53 controlled the function of the estrogen receptor, and how it might affect the response of tumor cells to hormone therapy.
That led her team to look atovarian cancer because of its high prevalence of p53 mutations. They used cell lines and a lab model to mimic stage 3 and 4 tumors.
The researchers found that when mutant p53 was bound to the estrogen receptor in these models, it inhibited part of the estrogen receptor’s activity, driving resistance to hormone therapy.
By simply removing the mutant protein, tumors “responded great” to the hormone therapy, Murphy said.
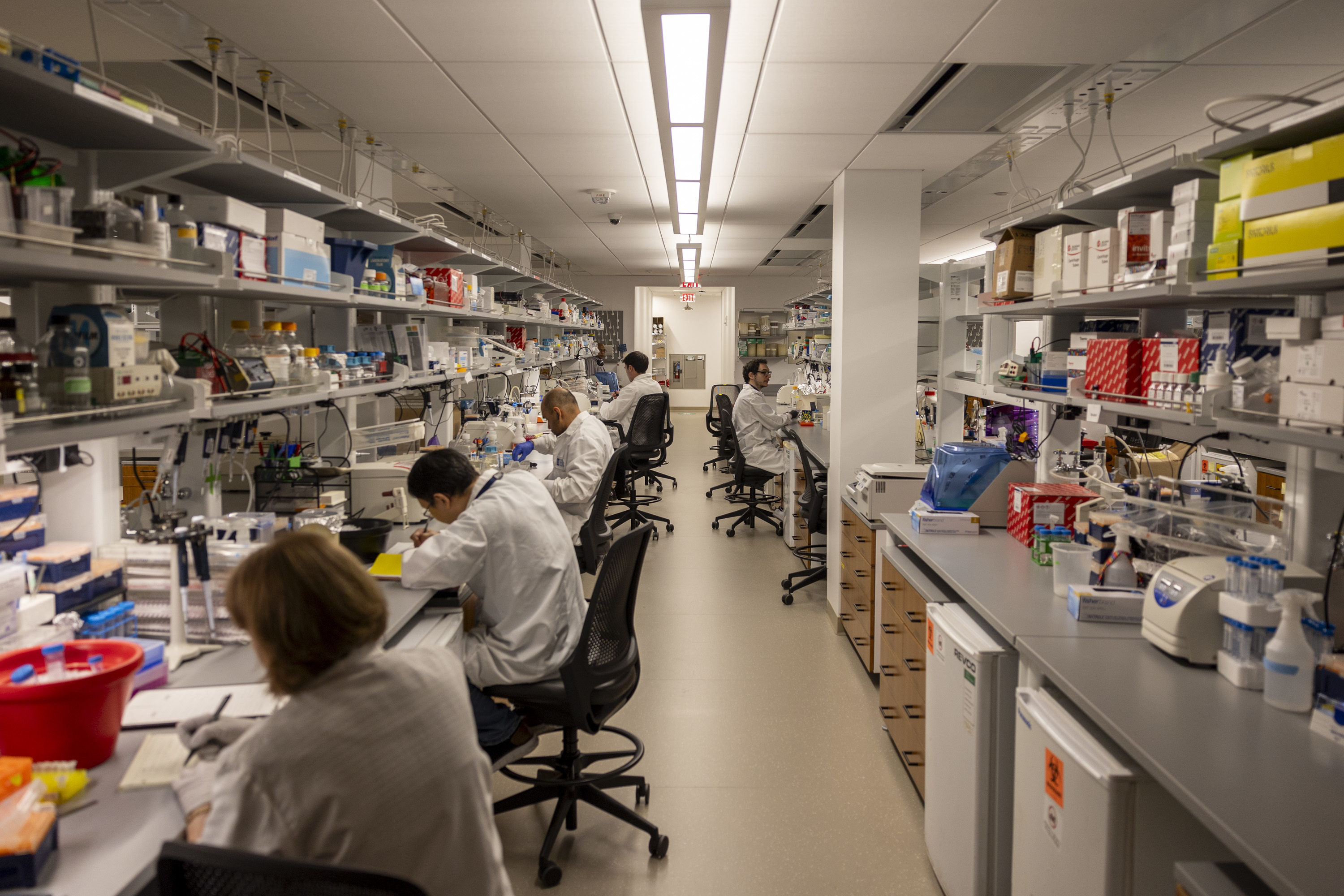
A lab at the Wistar Institute in Philadelphia.
Hope for hormone therapy?
While it’s easy to take away p53 in the lab, it’s not as easy in a patient.
There is, however, a promising drug currently being tested in clinical trials. Called rezatapopt, it can convert mutant p53 into a normal-functioning version of the protein.
It works for one particular mutation, Y220C, found in roughly 4% of ovarian cancers.
Murphy’s team foundadministering rezatapopt alongside hormone therapy led to 75% shrinkage of ovarian tumor models, versus 50% shrinkage when the hormone therapy was given alone.
This finding lined up with rezatapopt’s early data from clinical trials.
“For reasons we didn’t understand, women with ovarian cancer were responding best to this drug,” Murphy said.
Nineteen out of 44 women treated with rezatapopt alone saw their tumors shrink, with one even having a complete response, according to recent interim results from a phase 2 trial.
Murphy hopes this paper will prompt clinical trials to test rezatapopt in combination with anti-estrogen therapy.
However, since rezatapopt only targets one p53 mutation, this approach is limited to a small subset of patients. Murphy hopes that more drugs can be developed thatfix other mutant forms of p53 seen in ovarian cancer.
Murphy’s findings make sense conceptually and present a “promising avenue for future clinical trials,”said Tian-Li Wang, the head of the Molecular Genetics Laboratory of Female Reproductive Cancer at Johns Hopkins University, who was not involved in the Wistar study.
A caveat is that the study looked at a limited number of cell lines, she said.
She thinks the results should be confirmed in cases of ovarian cancer that have other types of p53 mutations to see if it could be applied more broadly.
“[I’m] really interested to see if the approach can benefit patients,” Wang said.
Riddle Hospital was cited by the Pennsylvania Department of Health for failing to properly monitor a patient’s vital signs in the emergency department earlier this year.
The incident was among six times inspectors visited the Media hospital, which is owned by Main Line Health, to investigate potential safety problems.
Here’s a look at the publicly available details:
Jan. 10, 2025: Inspectors came to investigate a complaint but found the hospital was in compliance. Complaint details are not made public when inspectors determine it was unfounded.
June 30: Inspectors cited the hospital for failing to properly monitor a patient’s vital signs while waiting for care in the emergency department. Inspectors found that a patient was evaluated in the emergency department as a triage level 3, meaning their vital signs should be checked every four hours. Records show the patient’s vital signs were documented at 12:40 a.m., and not again until almost seven hours later. Administrators reviewed the hospital’s emergency triage policies and retrained staff.
Aug. 13: Inspectors came to investigate a complaint but found the hospital was in compliance.
Sept. 15: Inspectors came to investigate a complaint but found the hospital was in compliance.
Sept. 18: Inspectors visited for a special monitoring survey and found the hospital was in compliance.
Sept. 18: Inspectors followed up on the June citation regarding vital sign monitoring and found the hospital was in compliance.
Philadelphia didn’t take home any Nobel Prizes this year, but work illuminating how babies respond togarlic-flavored breast milk at Monell Chemical Senses Center did get recognized by its satirical counterpart, the Ig Nobel Prize.
Julie Mennella, a longtime scientist at the center in West Philadelphia, and Gary Beauchamp, Monell’s former director, won the prize earlier this fall for their 1991 study published in the academic journalPediatrics that disproved popular folklore around breastfeeding.
Their study examined whether eating garlic would flavor a mother’s breast milk and, if so, how a nursing baby would react to it.
At the time, breastfeedingwomen were often told to eat bland foods, for fear their babies would reject strong flavors. However, the study’s results showed the opposite: Babies savored the garlic-flavored breast milk.
“That simple, elegant study really showed how one of the first ways we learn about foods is through what our mothers eat,” Mennella said.
These early life experiences shape food preferences and influence cultural food practices around the world, she emphasized. Babies whose mothers come from cultures in which garlic is a defining flavor would have experienced garlic long before their first meal.
Mennella spoke with The Inquirer about the implications of her Ig Nobel Prize-winning work and her decades of research on flavor sciences and early nutritional programming.
The following conversation has been lightly edited for length and clarity.
What did you discover in your Ig Nobel Prize-winning study?
We found in this study that not only did the milk get flavored with garlic, but contrary to a lot of the folklore, the babies actually liked it. They nursed longer when the milk was garlic-flavored than when it was bland and devoid of garlic.
We went on to show that when women eat garlic, the flavor of amniotic fluid also gets altered.
Through these first exposures, babies are learning about what mom is eating, what mom has access to, and what mom likes before their own first taste of solid food.
What is the takeaway for breastfeeding mothers?
Eat the healthy foods that you enjoy because your baby’s going to learn about the food. Food is much more than a source of calories. In many cases, it defines who we are as a people.
What other flavors have you studied?
A wide variety of flavors, from vanilla to even alcohol if a woman drinks it, get transmitted and flavors the milk. If women smoke, the tobacco flavor does, too. So it’s not only what you eat, but what you breathe.
Why is it important for babies to learn about food this way?
There’s a great story about the European rabbit (an animal that nurses), where they tagged the mother’s diet with juniper berry. What they were able to show is that in a group where the mothers ate juniper berry during either pregnancy or lactation, once those young rabbit pups left the nest, they were more likely to forage on juniper berry.
So, she’s telling them, ‘These are the foods that are out there. I’m eating them. They’re safe.’ It’s really a very elegant, sustainable behavior, how moms transmit this information about the foods in the environment. She’s teaching her young and giving them an advantage early on.
How long do these flavors last in the milk?
Depending on the size of the chemical, some will get in fast. Garlic gets in a couple hours after the mom eats it, and then if she stops eating, it’s out of the milk like four or five hours later. The sensory experience of that baby is changing throughout the course of the day, day to day, depending on what she eats.
What research have you been up to since?
I’ve gone into so many different directions of looking at not only early flavor learning, but also nutritional programming. I also looked at the taste of medicine in children, looking at individual differences because taste is the primary reason for noncompliance. Children have a harder time because they can’t encapsulate the bad taste in a pill or tablet, so liquid medicines are particularly difficult.
One study where we looked at variation in the taste of pediatric Motrin (among adult participants) was really interesting. Some people experience a tingle when they taste it. Others don’t. It makes you think that how one child tastes Motrin isn’t like how another does. If you don’t experience the tingle, or this burning sensation, all you taste is a sweet liquid, and those are the children that may be at risk of over-ingestion.
What is your favorite project that you have worked on since the garlic study?
I serendipitously found that another flavor that gets transmitted is alcohol, and that became a whole new area of research.
We found that when women just have the equivalent of one or two glasses of wine or beer, not only did the alcohol get transmitted, but it flavored the milk. That became a lead article in theNew England Journal of Medicine.
At that time, there was talk about a folklore that women should drink when they’re breastfeeding, so they would make more milk. And contrary to that folklore, they actually made less milk.
How did it feel to win an Ig Nobel?
It was so nice to celebrate science. That’s really what that award does: It uses humor to teach about science.
Pennsylvania’s Department of Health investigated several complaints at the Children’s Hospital of Philadelphia between October 2024 and September of this year but did not cite the hospital for any safety violations.
Here’s a look at the publicly available details:
Oct. 30, 2024: Inspectors came to investigate a complaint but found the hospital was in compliance. Complaint details are not made public when inspectors determine it was unfounded.
Jan. 27, 2025: Inspectors came to investigate a complaint but found the hospital was in compliance.
Feb. 18: Inspectors came to investigate a complaint but found the hospital was in compliance.
March 11: Inspectors came to investigate a complaint but found the hospital was in compliance.
May 15: Inspectors came to investigate a complaint but found the hospital was in compliance.
Temple University Health System reported a $15 million operating loss in the three months that ended Sept. 30.
The result for the first quarter of fiscal 2026 was an improvement from the North Philadelphia nonprofit’s $17 million loss last year.
“We’re pretty happy where we are,” CEO Mike Young said Wednesday. Revenue was above budget and labor costs were on budget in the first quarter for the first time in several years.
Here are some details:
Revenue: Total revenue was $800 million, up 13% from $712.5 million a year ago. Outpatient revenue increased by nearly $62 million, much of it from the health system’s specialty and retail pharmacy business.
Temple participates in a federal program for safety-net hospitals that allows it to buy certain drugs at a discount and then get full reimbursement from insurance companies.
Expenses: Temple noted in its report to municipal bond investors Tuesday that salaries, including higher pay rates for nurses, and higher drug spending for outpatient infusions and other pharmacy business were the biggest expense increases.
Notable: On the labor front, several job categories remain hard to fill, Young said. Those are CT techs, nurse anesthetists, and lab techs. “Other than those three [specialties], it’s not where it was three years ago, where you couldn’t find anybody,” he said.
A lawsuit filed Tuesday in Philadelphia accused Jefferson Health of violating federal labor rules when it laid off 1% of its 65,000 employees in October and this month without providing a 60-day notice.
The purported class-action lawsuit says the proposed lead plaintiff, Ciara Brice, lost her job as a medical assistant on Nov. 12 with no notice and has not received the severance pay she was promised.
Brice was not available for comment, said her lawyer, Jeremy E. Abay, with Philadelphia law firm Pond Lehocky Giordano Inc.
The Worker Adjustment and Retraining Notification Act has a complicated rubric for determining when a mass layoff requires advance notification, which is filed with state labor departments. One of the triggers is an employer cutting at least 500 jobs, according to Abay.
Even though the layoffs happened throughout Jefferson’s entire footprint from South Jersey to near Scranton, Abay said notice is required because Jefferson operates as a single entity.
“We believe the facts will show that there was no violation of the federal WARN Act,” Jefferson said in a statement.
The nonprofit filed a notice of 108 layoffs at Jefferson Cherry Hill Hospital, Jefferson Stratford Hospital, and Jefferson Washington Township Hospital because New Jersey has its own rules, Abay said.
The nonprofit, which grew through acquisitions from three hospitals in Philadelphia in 2015 to more than 30 now, provided no details when it announced the layoffs in mid-October.
That layoff was part of a series of large job cuts starting in the summer of 2023, but may have been the first time patient-facing workers like Brice were hit.
The lawsuit seeks back pay, benefits, and damages for each laid-off employee who did not receive a 60-day notice.
Editor’s note: The headline on this article has been updated to clarify that a lawsuit claims violations.
A Philadelphia jury reached $35 million verdict last week against Main Line Health and the University of Pennsylvania Health System for a cancer misdiagnosis that led a then-45-year old Philadelphia resident to undergo a total hysterectomy in 2021.
Main Line discovered later that the biopsy slides used to make the diagnosis in February 2021 were contaminated. The cancer diagnosis was due an error that involveda second person’s DNA, not that of the plaintiff, Iris Spencer, who did not have cancer.
Main Line settled with Spencer in 2022 for an undisclosed amount, so it won’t have to pay its share of the verdict.
The jury found Penn and its physician, Janos Tanyi, a gynecological oncologist, liable for $12.25 million, or 35%, of the total awarded in damages for her unnecessary hysterectomy. The lawsuit said Spencer suffers from “surgically-induced menopause.”
The lawsuit against Penn and Tanyi said the physician did not do enough to resolve a conflict between biopsy results at Main Line and those at Penn, where Spencer sought a second opinion.
A Penn biopsy did not find cancer. Other tests were also negative, but Spencer did not know about those results.
“The verdict affirms the central importance of the patient and the doctor’s obligation to inform the patient of all of the test results, of all of her options, and that she shouldn’t be dismissed because she’s a patient and not a doctor,” Spencer’s lawyer, Glenn A. Ellis, said Monday.
The $35 million verdict is Philadelphia’s largest this year for medical malpractice, according to data from the Philadelphia Court of Common Pleas.
Medical malpractice costs have been rising throughout healthcare. A factor in Pennsylvania is a 2023 rule change that allowed more flexibility in where cases can be filed.
Spencer’s troubles started in February 2021 at Main Line’s Lankenau Medical Center where her biopsy found that she had cancer in the lining of her uterus despite the lack of symptoms.
For a second opinion, Spencer saw Tanyi at Penn a few days later. A repeat biopsy came back negative, according to Spencer’s complaint that was filed in early 2023. Tanyi also performed other tests, all of which came back negative, but he did not share that information with Spencer, the complaint says.
After Tanyi performed the complete hysterectomy on March 8, 2021, Penn’s pathology laboratory found no cancer in the tissues that had been removed from Spencer’s body.
That’s when Spencer, who has since moved to Georgia, went back to Lankenau seeking an explanation. Seven months later, Main Line informed her that she never had cancer.
Main Line and Spencer subsequently “reached an amicable full and final settlement to resolve and discharge all potential claims for care involving the health system,” Main Line said in a statement. Main Line did not participate in the trial.
Penn said in a statement: “We are disappointed by the jury’s verdict in this case that was unmoored to the evidence presented at trial on negligence and damages. Our physician reasonably relied on the pathology performed at a hospital outside our system that revealed a very aggressive cancer.”
Penn said it plans to appeal the verdict, which could increase by more than $2 million if the court approves a motion for delay damages that Ellis filed Saturday.
Temple University Health System‘s medical malpractice expenses have surged in the two years that ended June 30 as part of a campaign to reduce financial risk by settling old cases.
The hope is that “aggressively” settling cases will pay off over the next few years by reducing medical malpractice expenses, Michael DiFranco, the health system’s chief accounting officer, told investors during a conference call last week on the health system’s fiscal 2025 financial results.
Temple’s annual medical malpractice expenses increased nearly fourfold, to $117.8 million in fiscal 2025 from $31.6 million two years ago. Over the same period, it cut its reserves for future expenses by $88 million, or 22%. Temple’s reserves peaked at $402.9 million in 2023.
Rising medical malpractice costs are reverberating throughout healthcare. Tower Health recently boosted its reserves after its auditor decided they should be higher to deal with anticipated claims. Lifecycle Wellness, a birth center in Bryn Mawr, blamed its decision to stop delivering babies in February in part on rising medical malpractice costs.
The average number of medical malpractice lawsuits filed in Philadelphia every month has risen from 34 and 35 in the two years before the pandemic to 51 last year and 52 so far this year, according to the Philadelphia Court of Common Pleas.In additional to lawsuits against hospitals, the tally includes litigation against physicians, nursing homes, and other healthcare providers.
Contributing to the increase was a rule change at the beginning of 2023 that allowed more cases to be filed in Philadelphia rather than the county where an injury occurred. Malpractice lawyers say they like to file in Philadelphia because the system for trying cases is efficient. Health systems often note that Philadelphia juries sometimes award large verdicts.
A ‘wake-up call’ at Temple
Temple Health started rethinking its medical malpractice strategy after John Ryan started as general counsel in January 2022. A month before he started, The Inquirer published an article about three suicides at Temple Episcopal Hospital in 2020. At least two of the families sued Temple.
“That was a wake-up call,” Ryan said in a recent interview on his approach to handling malpractice cases.
Then in May 2023, a Philadelphia jury hit Temple with a $25.9 million verdict in a case involving a delayed diagnosis of a leg injury leading to an amputation.
After that loss, Temple changed the kinds ofoutside lawyers it hiresto defend it in malpractice cases, Ryan said, swapping medical malpractice specialists for commercial litigators from firms like Blank Rome, Cozen O’Connor, and Duane Morris. Such lawyers cost more, but it’s paying off, he said.
“The settlements we’re getting from the plaintiff lawyers, because they can see that we’re serious, are much better,” Ryan said. The two Episcopal cases were settled this year for undisclosed amounts, according to court records. A birth-injury lawsuit against Temple University Hospital in federal court settled for $8 million this month.
In 2024, a jury awarded $45 million to a teen who was shot in the neck and suffered brain damage from aspirating food soon after his release from Temple. Temple appealed and the judge who oversaw the original trial ordered a new one. That case then settled at the end of October for an undisclosed amount.
The new approach has helped Temple reduce the number of outstanding cases at any one time to 65 or so now compared to 110 three years ago, according to Ryan.
Temple is using the money it is saving on malpractice costs to invest in better and safer care, Ryan said. “That’s not a byproduct of all we’re trying to do as the lawyers. It’s the goal,” he said.
Inquirer staff reporter Abraham Gutman contributed to this article.
When Pamela Collins was pregnant, she would talk and sing to her sonthrough her belly, telling him he was loved.
He was the “miracle” that the 32-year-old mother had been waiting for, after four miscarriages and an ectopic pregnancy.
She never expected that her son, John, would arrive early at 29 weeks in September and have tospend his first months in the intensive care nursery at the Hospital of the University of Pennsylvania.
Her family hasrelocated from Mount Pocono to stay at the nearby Ronald McDonald House, a charity, so they canvisit John every day. Even still, she wishes she could be with him all the time, to sing to him and tell him that he is strong and loved — just as she did when he was in her womb.
A new medical device being tested at HUP could help her do just that.
Collins’ son is one of five babies so far to try out the Sonura Beanie, a device that aims to connect NICU babies with their parents and block out harmful noises in the hospital environment.
Invented by five undergraduates at the University of Pennsylvania, the beanie is designed to mimic the womb, by filtering out high-frequency sounds like alarms — which frequently plague the NICU — while allowing human voices at low frequencies to be heard.
The device can also deliver audio messages recorded by parents for their babies.
“It’s as if they were laying on your chest [or] as if they were in the womb,” said Sophie Ishiwari, one of the founders.
Their idea won Penn’s 2023 President’s Innovation Prize, which provided a $100,000 cash award and living stipends for the team to pursue their commercial project after graduation. Three of the original members went onto medical school, leaving two — Gabby Daltoso and Ishiwari — to continue working on the product full-time.
In the two years since graduating, they’ve tested the device in the lab and pitched it to hospitals around the country, earning accolades along the way. Now, they’re putting the beanie on infants in the hospital for the first time.
Over the next several months, Ishiwari and Daltoso will be testing the beanie on 30 infants in HUP’s intensive care nursery. They’ll be looking to see whether the beanie can reduce stress, based on changes in heart rate, respiratory rate, and oxygen saturation.
They will also evaluate how easy it is for nurses to use, and how parents feel about the experience.
Collins joined the study hoping the beanie could help her son feel calmer by hearing her voice, as well as that of his father and teenage sister.
“I know my baby can listen more than he can see, and I’m excited to know he’s listening to our voices instead of this beeping,” she said, gesturing to the noisy NICU machines.
Pamela Collins suffered four miscarriages and an ectopic pregnancy before giving birth to John.
The origin
The first thing Daltoso and Ishiwari noticed when shadowing in the NICU was how loud it was. Between beeping from machines to hospital alarms going off, it felt overwhelming even for adults.
“They can’t turn the alarms off because it’s their job to keep patients alive,” Daltoso said.
In the womb, a fetus would primarily be exposed to low frequency sounds under 500 Hertz. Alarms in the NICU can hit 2,000 Hertz and higher, Daltoso said. Imagine having to hear a fire alarm go off continuously throughout the day.
A 2014 study found that babies in a NICU in Massachusetts were exposed to frequencies over 500 Hertz 57% of the time.
Some medical equipment also emit high frequencies of sounds. Babies on a ventilator, for example, are exposed to sounds in the 8,000 Hertz range of frequencies, Daltoso said.
“They’re in a room of 20, so if one baby’s on it, they’re all exposed,” she added.
In the short term, this noise can stress babies out to the point of not being able to sleep or eat, Daltoso said. Babies may experience trouble gaining weight as a result and show unstable signs such as heart rates that arefaster than normal.
Babies in the NICU could also suffer long-term impacts from what is known as “language deprivation,” Ishiwari said.
Normally, an infant would be exposed to language early in life, which is important for the infant’s neurodevelopment. But a baby in the NICU has less exposure to their parents’ speech.
Studies have shown that preterm babies are generally at higher risk of language delays and deficits.
Daltoso and Ishiwari, alongside those three other seniors majoringin bioengineering at Penn, were inspired to create the beanie for their senior capstone project in 2023.
Through a sound-engineering class and interviews with hundreds of clinicians and parents, they devised the technology inside the beanie to cancel out high-frequency noises, particularly above the 2,000 Hertz range, while allowing lower frequencies through.
A mobile app connects to the hat to enable parents to send songs, stories, audio messages, and recordings of their heartbeat to the baby remotely through a speaker in the hat.
The babies wear the beanies during feeding so that it mimics a real-life interaction, where the baby would normally be lying against their mother’s chest.
Ishiwari said she has teared up listening to some of the messages parents were leaving for their babies. They’ve so far included bedtime stories, songs, and shorter messages like “I love you” and “good night.”
“A lot of them don’t know where to put that love and joy and excitement,” Daltoso said. “This is a place that they can.”
Gabby Daltoso and Sophie Ishiwari are testing the beanie at the Hospital of the University of Pennsylvania.
Sending love from afar
When Collins and her husband, Franqlin, prepared to record messages for John, they turned off the lights in the room and prayed.
Then they started recording.
Collins, who is originally from Brazil, sang a Brazilian song to tellhim that he is perfect the way he is. Her husband made up a story about John, and her 15-year-old daughter narrated another with the messagethat he is enough.
A nurse told Collins that John was laughing when he wore the beanie.
“I can tell he loved that,” Collins recalled the nurse telling her.
Babies in the study wear the beanies for three 45-minute sessions a day, butCollins wishes her son could wear his the whole day.
“I feel babies can be more calm now and [won’t] be crying all the time,” she said.
The beanie designed by Gabby Daltoso and Sophie Ishiwari cancels out high-frequency sounds while allowing low-frequency sounds through.
Michelle Ferrant, a clinical nurse specialist in HUP’s intensive care nursery, was excited that its NICU was chosen as a pilot site.
Herteam has done projects to try to reduce noise levels in the NICU, including putting signs up to remind people to use hushed voices, and closing doors and trash can lids as softly as possible.
“There are a lot of things that might not seem very loud to us, but [if] you’re a small baby and it’s so close to [you], it sounds much louder,” Ferrant said.
However, until the beanie study came along, they didn’t have a way of filtering which noises babies heard.
The Sonura Beanie team is next looking to launch a multi-center trial that will evaluate whether wearing the beanie could help promote weight gain.
Exposure to their mother’s voice and reduced noise levels can help preterm infants with weight gain and feeding, studies have shown.
“We will be looking to prove that our hat is able to soothe the babies to the point where they are taking in more food, gaining more calories, growing faster, and hopefully going home faster,” Daltoso said.
They also plan to launch in other hospitals, including Stanford Medicine Children’s Health, affiliated with Stanford Medicine and Stanford University in California, so that clinicians can test out the product and see how it fits into their workflow. These pilots would function like “a trial for a pre-purchase,” Daltoso said.
They are currently working on submitting their medical device for clearance by the Food and Drug Administrationso they can begin selling it.
Because the product is deemed low-risk in terms of safety, they are eligible for fast-track approval, which they expect to get within the next year, Daltoso said.
The team is still working on setting a price and declined to disclose details.
They would eventually hope to get the product covered by insurance as a sensory-integrative technique. For that, they would need their larger clinical study to show that the beanie has functional outcomes.
‘Holding the miracle’
John weighed only one pound and 14 ounces at birth.
John doesn’t have a specific release date from the NICU. The timeline will depend on when he is able to breathe on his own and put on weight.
At birth, he weighed only 1 pound, 14 ounces. Today, he weighs more than 4 pounds and no longer requires a feeding tube.
Collins was 20 weeks pregnant when she found out that John had a heart defect that doctors said may one day require surgery. A few weeks after that, doctors found an issue with the placenta that ultimately led to his preterm birth.
Now, when she holds her son in her arms, she feels like “I am holding the miracle,” she said.