Family Practice & Counseling Services Network won a $3.4 million federal health center grant that will allow the nonprofit to continue providing medical and mental healthcare in Southwest Philadelphia and other low-income Philadelphia neighborhoods, officials confirmed this week.
The clinic had been part of Resources for Human Development, a Philadelphia human services agency that a fast-growing Reading nonprofit called Inperium Inc. acquired in late 2024. As a federally qualified health clinic since 1992, the clinic had received an annual federal grant, higher Medicaid rates, and other benefits.
Federal rules prohibited the clinic from continuing to retain that status and those benefits under a parent company. That meant Family Practice & Counseling Network had two options: close or spin out into a new entity that would reapply to be a federally qualified clinic.
With financial and operational help from the University of Pennsylvania Health System, Family Practice & Counseling formed a new legal entity last July and reapplied for the grant. Last week, the organization’s CEO Emily Nichols learned that the federal agency that oversees federal health centers awarded it the grant.
A new sign with orange letters outside a former Rite Aid in Germantown announces the arrival of a primary care model new to the Philadelphia region.
ArchWell Health recently opened its first three of eight planned primary care centers here for people with Medicare Advantage, promising convenient and personalized care in neighborhoods with a relative lack of doctors.
Two others have opened on North Broad Street, near Stenton and Susquehanna Avenues, also in former Rite Aid stores.
A privately held company based in Nashville, Tenn., ArchWell says it can offer patients greater access to healthcare throughlower patient-provider ratios.
Itplans to limit each of itsphysicians to no more than 500 patients — about a fifth of the patient load for typical primary care doctors. Nurse practitioners working under the doctors will manage a maximum of 250 patients,officials said.
The approach is built around a financial model that differentiates ArchWell from Medicare-focused competitors already in Philadelphia like Oak Street Health and ChenMed’s Dedicated Senior Medical Centers. ArchWell only accepts patients who have private Medicare or are willing to switch to it. Oak Street and ChenMed also accept traditional Medicare.
Privately run Medicare Advantage plans are increasingly popular among people ages 65 and older who qualify for government-funded Medicare coverage. Advantage plans appeal to people bycovering services, such as dental and vision care, left out of traditional Medicare, but have come under scrutiny for exaggerating how sick patients are to rack up more revenue.
ArchWell sees exclusively working with Medicare Advantage plans as helping doctors to focus solely on the best outcomes for patients, rather than on providing more services to bring in more revenue, a criticism of traditional Medicare, said Doron Schneider, its medical director for the Philadelphia market.
Melissa A. Herd, community relations specialist for ArchWell Health in Philadelphia, is shown outside the company’s Germantown location, which is in a former Rite Aid building.
“You have different incentives, you have different care models, you have different case management models, you have different ways to treat one person versus the other,” Schneider said.
Before starting at ArchWell in late 2024, Schneider worked at Tandigm Health, an Independence Health Group company founded in 2014 with the goal of helping primary care doctors manage costs and improve care for their patients. He learned there how hard it is for doctors to work with different types of insurers and the varied incentives that go with them.
How ArchWell conducts business
ArchWell, which opened its first clinic in 2021 in Birmingham, Ala., operates under contracts with Medicare Advantage plans. The plans give ArchWell a portion of the monthly payment they get from Medicare for each patient. That money is supposed to cover all of the person’s medical costs.
Aetna, UnitedHealthcare, and Devoted Health have contracts with ArchWell to cover the Philadelphia market. ArchWell is close to getting contracts with HealthSpring and Humana, Schneider said. Those five companies had more than 90,000 people in their plans in December, according to federal data.
Aetna and UnitedHealthcare said they work with clinics like ArchWell’s around the country to improve health outcomes and leave patients more satisfied with their experience.
“We are pleased that they are now an option for Aetna Medicare Advantage members in the Philadelphia area,” Aetna said in a statement.
ArchWell declined to provide financial details, such as annual revenue from the more than 80 clinics it had in a dozen states before coming to Philadelphia or how much it spends to open each center. ArchWell representatives also did not disclose who its owners are.
The interior of Archwell Health’s Germantown primary care clinic has Philadelphia-centric images painted on the walls.
Company founder Carl Whitmer worked at Clayton, Dubilier & Rice, a global private equity firm, before founding ArchWell.
“We have partners that are focused on our sustainability and growth,” said Christina Cober, ArchWell’s vice president of marketing.
But companies focused on primary care for seniors haven’t always been as successful as anticipated.
Oak Street, founded in Chicago in 2012, grew rapidly and now services 450,000 patients at 230 centers across the country. It declined to say how many patients it has in Philadelphia. Oak Street arrived here in 2018.
CVS Health bought Oak Street in 2023 for $10.6 billion, anticipating that it would expand to more than 300 centers by this year. Last fall, CVS announced it was closing 16 centers and taking a $5.7 billion write-down on its health-services business, largely because of slower anticipated growth at Oak Street.
ArchWell says itslowerpatient-provider ratios allow more frequent interactions with patients. If a patient is diagnosed with high blood pressure, Schneider said, the message to the patient is: “We’ll see you back in a week. We’ll see you back in two weeks.”
The repeat visits happen with no cost to the member and no extra revenue to ArchWell because all care is supposed to be covered by a monthly payment per member.
ArchWell expects to add about 300 patients per year at each center, said Cober. Staffing at the centers starts out with a physician, a nurse-practitioner, two care navigators, two medical assistants, and a center manager.
Among the early patients at ArchWell’s center on Germantown Avenue is Marcella James, 69, who lives across the street from the clinic and watched as the building was transformed from a shuttered Rite Aid.
“I walked over there one day just to see what it was like and what they offer, and I signed up right away,” James said. James likes her doctor at Temple Health, but ArchWell was irresistibly convenient.
“If I can get the same help or better help from ArchWell is to be seen because I just started with them,” she said.
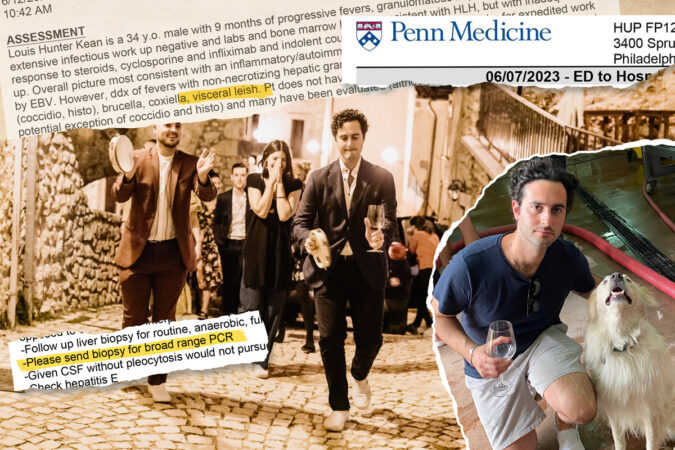
Each night, Louis-Hunter Kean spiked a fever as high as 104.5. He would sweat through bedsheets and shiver uncontrollably. By morning, his fever wouldease but his body stillached; even his jaw hurt.
He had been sick like this for months. Doctors near his South Jersey home couldn’t figure out why a previously healthy 34-year-old was suffering high fevers plus a swollen liver and spleen. In early 2023, they referred Kean to Penn Medicine.
Louis-Hunter Kean visiting a winery in the Tuscany region of Italy in September 2021. He first spiked a mysterious and persistent fever about a year later in August 2022.
“These doctors are very sharp, and there are a lot of teams working on it,” Kean texted a friend after being admitted to the Hospital of the University of Pennsylvania (HUP) in West Philadelphia.
Was it an infection? An autoimmune disease? A blood cancer? Over the next six months, at least 34 HUP doctors — rheumatologists, hematologist-oncologists, gastroenterologists, infectious disease and internal medicine specialists — searched for an answer.
Kean was hospitalized at HUP five times during a six-month period in 2023. His electronic medical chart grew to thousands of pages.
Along the way, doctors missed critical clues, such as failing to obtain Kean’s complete travel history. They recommended a pair of key tests, but didn’t follow up to make sure they got done, medical records provided to The Inquirer by his family show.
Doctors involved in Kean’s care, including at Penn, prescribed treatments that made him sicker, said four infectious disease experts not involved in his care during interviews with a reporter, who shared details about his treatment. Penn doctors continued to do so even as his condition worsened.
Louis-Hunter Kean receives a kiss from bride Ashley Greyson at the October 2021 wedding of his close friend, Joshua Green. Green and Kean graduated from Haddonfield High School in 2007.
“No one was paying attention to what the doctor before them did or said,” Kean’s mother, Lois Kean, said.
“They did not put all the pieces together,” she said. “It was helter-skelter.”
Kean’s family is now suing Penn’s health system for medical malpractice in Common Pleas Court in Philadelphia. The complaint identifies nearly three dozen Penn doctors, accusing them of misdiagnoses and harmful treatments. These physicians are not individually named as defendants.
In court filings, Penn says its doctors did not act recklessly or with disregard for Kean’s well-being, and his case is not indicative of any systemic failures within its flagship hospital. A Penn spokesperson declined further comment on behalf of both the hospital and the individual doctors involved in Kean’s care, citing the pending lawsuit.
The puzzle of Kean’s diagnosis finally came together in November 2023 after a Penn doctor, early in his career, sought help from the National Institutes of Health (NIH).
An NIH doctor recommended a test that identified the cause: a parasite prevalent in countries bordering the Mediterranean Sea. Kean likely got infected while vacationing in Italy, four parasitic disease experts told The Inquirer.
The infection, which is treatable when caught early, is so rare in the U.S. that most doctors here have never seen a case, the experts said.
By the time Penn doctors figured it out, Kean’s organs were failing.
Louis-Hunter Kean and his then-girlfriend Zara Gaudioso at a friend’s wedding in Tuscany in September 2021. Kean and Gaudioso got engaged in early 2023. Gaudioso was smitten by Kean’s good looks and sense of humor.While vacationing in Italy in September 2021, Louis-Hunter Kean and his friends hiked in the foothills of the Apennine Mountains and visited Gran Sasso and Monti della Laga National Park.
A missed clue
When a patient has an ongoing and unexplained fever, an infectious disease doctor will routinely start by takinga thorough travel history to screen for possible illnesses picked up abroad.
A medical student took Kean’s travel history during his initial workup at HUP in June 2023. An infectious disease specialist reviewed the student’s notes and added a Cooper University Hospital doctor’s earlier notes into Kean’s electronic medical chart at Penn.
Those records show Kean had traveled to Turks and Caicos with his fiancée in May 2022. The next month, he took a work trip out West, including to California, where he visited farms, but didn’t interact with livestock.
This was not unusual for Kean, who worked with fruits and vegetables imported from around the world at his family’s produce distribution center on Essington Avenue in Southwest Philadelphia.
Kean’s fiancée, Zara Gaudioso, said she repeatedly told doctors about another trip: In September 2021, about a year before his fevers began, they traveled to Italy for a friend’s wedding in Tuscany.
The couple hiked remote foothills, danced all night in a courtyard, dined by candlelight surrounded by a sunflower farm, and slept in rustic villas with the windows flung open.
“We told everybody,” Gaudioso said. “A lot of Americans go to Italy — it’s not like a third-world country, so I could see how it could just go in one ear and out the other.”
But notes in Kean’s medical record from the Penn infectious disease specialist don’t mention Italy. Neither do the ones the specialist copied over from Kean’s infectious disease doctor at Cooper.
Kean “does not have known risk factors” for exposure to pathogens, the Penn specialist concluded, except possibly from farm animals or bird and bat droppings.
Still, the specialist listed various diseases that cause unexplained fever: Tick-borne diseases. Fungal infections. Tuberculosis. Bacteria from drinking unpasteurized milk.
The possible culprits included a parasitic disease, called visceral leishmaniasis, transmitted by a bite from an infected sandfly. It can lie dormant for a lifetime — or, in rare cases, activate long after exposure, so it’s important for doctors to take extensive past travel histories, parasitic experts say.
The parasite is widely circulating in Southern European countries, including Spain, Greece, Portugal, and Italy.
“Mostly, people living there are the ones who get it. But it’s just a lottery sandwich, and there’s no reason that travelers can’t get it,” said Michael Libman, a top parasitic disease expert and former director of a tropical medicine center at McGill University in Canada.
But few cases become severe. Hospitals in Italy reported only 2,509 cases of active infection between 2011 and 2016, affecting fewer than one in 100,000 people. Infections requiring hospital care in Italy began to decline after 2012, according a 2023 European study by the Public Library of Science (PLOS) journal Neglected Tropical Diseases.
Caught early, visceral leishmaniasis is treatable. Without treatment, more than 90% of patients will die.
In addition to fever, other telltale symptoms are swelling of the liver and spleen and low blood cell counts. Kean had all of those.
A missed test
The infectious disease specialist requested a test to examine tissue biopsied from Kean’s liver, which was damaged and enlarged. Lab results showed that immune cells there had formed unusual clusters — another sign that his body might be fighting off an infection.
In her notes, the specialist identified “visceral leish” as a possible diagnosis, which repeated — via copy and paste — seven times in his medical record. Her request to “please send biopsy for broad-range PCR” repeated five times.
That is a diagnostic (polymerase chain reaction) test that looks for the genetic fingerprint of a range of pathogens.
The test comes in different versions: One looks broadly for bacteria. The other is for fungi. The broad fungal test candetect leishmania, even though it’s not a fungus. However, it’s not always sensitive enough to identify the parasite and can produce a false negative, experts said.
The specialist’s chart note doesn’t specify which type she wanted done.
It’s not clear if anyone asked. The test wasn’t done.
Louis-Hunter Kean (right, with wine glass and tambourine) leads a wedding procession through the small stone village of Santo Stefano di Sessanio in Italy’s Abruzzo region in September 2021.
She did not order a low-cost rapid blood test that screens specifically for leishmaniasis by detecting antibodies made by the immune system after fighting it. She also didn’t order a leishmania-PCR, which is highly targeted to detect the exact species of the parasite.
Nor did the medical record show that the specialist followed up on the results of the broader test she requested, even though she saw Kean on nine of the 13 days of his first hospitalization at HUP in June 2023.
Penn has a policy that a lead doctor on the patient’s case is responsible for making sure that recommended tests get done. The specialist was called in as a consultant on Kean’s case. During that June hospitalization alone, his medical chart grew to 997 pages.
Patient safety experts have warned for years that electronic medical record systems — designed for billing and not for care — can become so unwieldy that doctors miss important details, especially with multiple specialists involved, or repeat initial errors.
A seemingly innocuous step in charting — copying and pasting previous entries and layering on new ones— can add to the danger, patient safety experts say.
That’s how the specialist’s mention of “visceral leish” and her test recommendation got repeated in Kean’s chart.
Marcus Schabacker, president of ECRI, a nonprofit patient-safety organization based in Plymouth Meeting, said “copy and paste” in electronic medical records puts patients at risk of harm.
“The reality is if you are reading something over and over again, which seems to be the same, you’re just not reading it anymore. You say, ‘Oh, yeah, I read that, let’s go on,’” said Schabacker, speaking generally about electronic medical record systems and not specifically about Kean’s case.
Louis-Hunter Kean plays guitar in his younger years. He loved music and shared eclectic playlists with his friends.
When treatments harm
Penn doctors believed Kean had a rare,life-threatening disorder, known as hemophagocytic lymphohistiocytosis (HLH), in which the immune system attacks the body. Instead of fighting infections, defective immune cells start to destroy healthy blood cells.
In most adults, the constellation of symptoms diagnosed as HLH gets triggered when an underlying disease sends the body’s immune system into overdrive. Triggers include a blood cancer like lymphoma, an autoimmune disease like lupus, or an infection.
Penn doctors across three specialties — hematology-oncology, rheumatology, and infectious disease — were searching for the cause within their specialties.
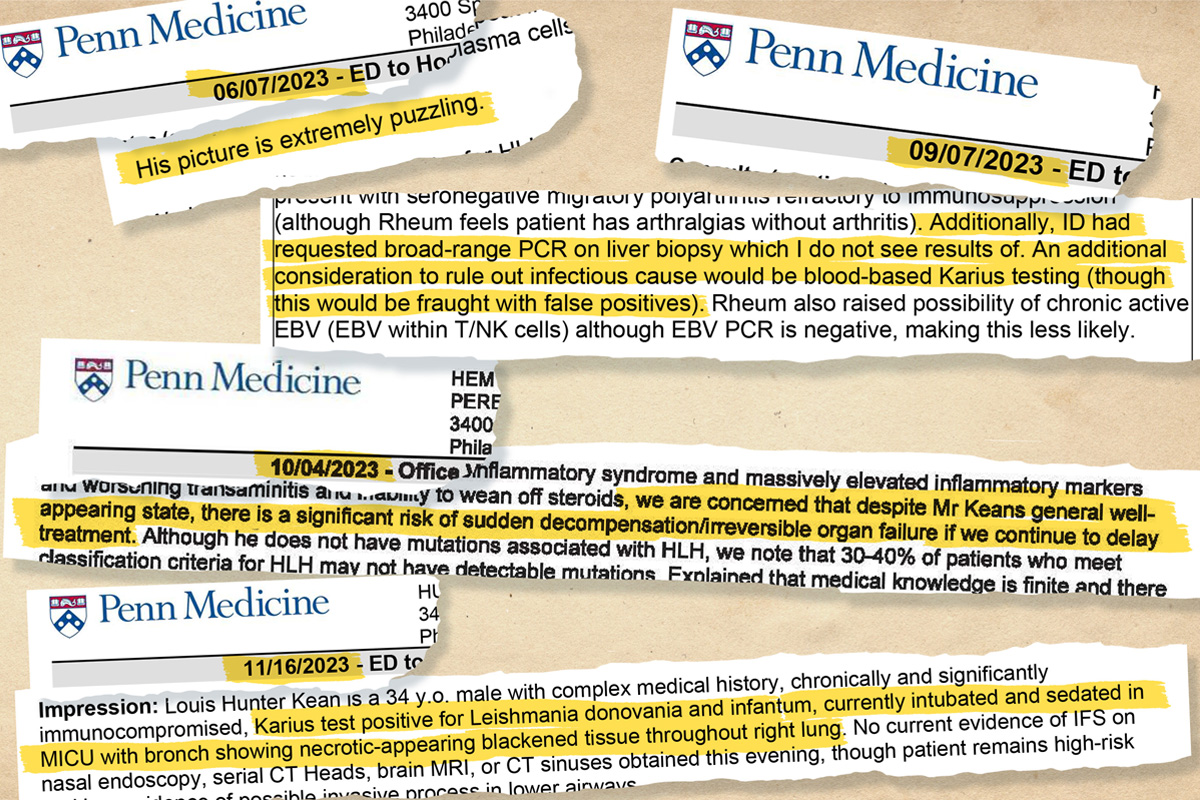
“His picture is extremely puzzling,” one doctor wrote in Kean’s chart. “We are awaiting liver biopsy results. I remain concerned about a possible infectious cause.”
As HUP doctors awaited test results, they treated Kean’s HLH symptoms with high doses of steroids and immunosuppressants to calm his immune system and reduce inflammation.
The treatments, however, made Kean highly vulnerable to further infection.And defenseless against another possible trigger of HLH: visceral leishmaniasis.
At the time, a Penn rheumatologist involved in Kean’s care before his first hospitalization warned about steroids “causing harm” to Kean if it turned out he had an infection. He wrote, “please ensure all studies requested by” infectious disease are done, medical records show.
Steroid treatments would allow the parasites to proliferate unchecked, experts said.
“It’s unfortunately exactly the wrong treatment for parasitic disease,” said Libman, the leishmania disease expert at McGill University.
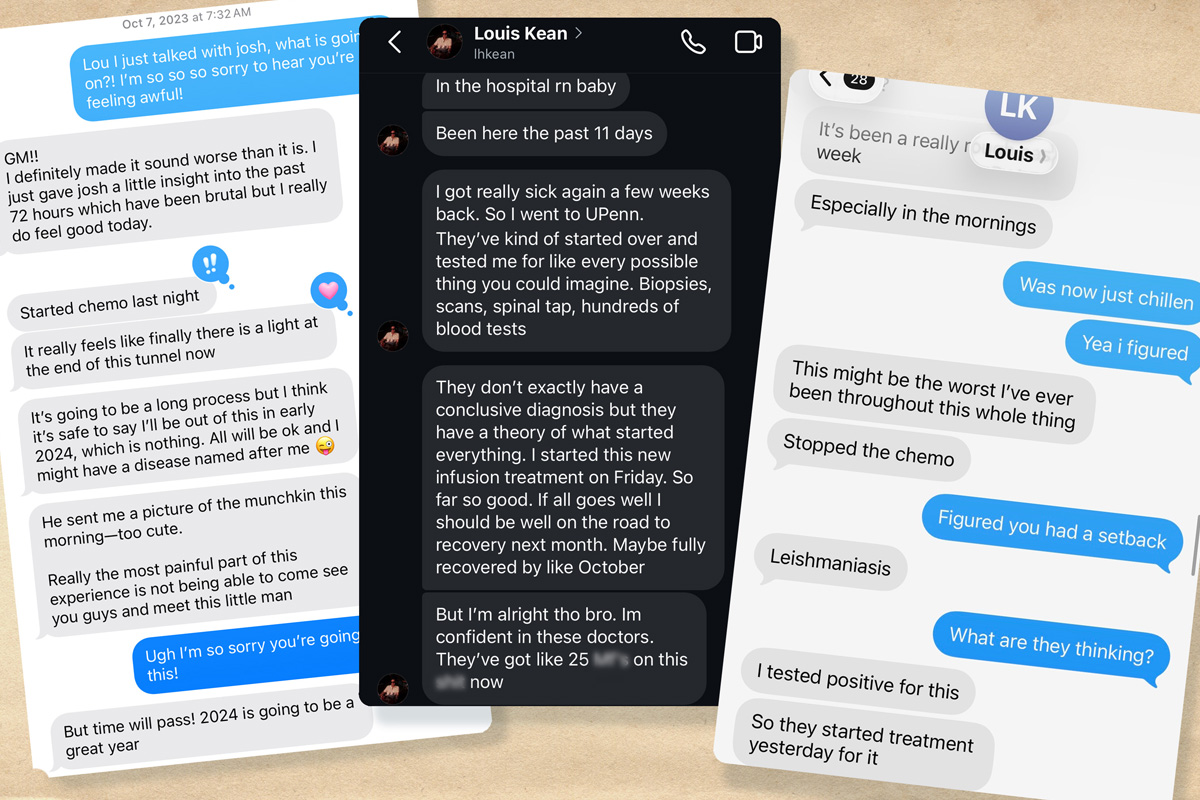
As Kean grew sicker, he was readmitted to HUP for a third time in September 2023. He texted a friend: “I’m on more medications than I’ve ever been on and my condition is worse than it’s ever been.”
A sampling of Louis-Hunter Kean’s electronic medical records, which ballooned to thousands of pages over five HUP hospitalizations within six months in 2023.
Handoffs between doctors
No single doctor seemed to be in charge of Kean’s care, his family said. And the number of specialists involved worried them.
“Everyone just kept being like, ‘We don’t know. Go see this specialist. Go see that specialist,’” Kean’s sister, Priscilla Zinsky, said.
By fall 2023, rheumatologists hadn’t found a trigger of Kean’s symptoms within their specialty. They turned to doctors specializing in blood cancer.
During the handoff, three doctors noted that they didn’t see the results of the test requested by the infectious disease specialist back in June. They still thought it was possible that Kean had an infection, records show.
“An additional consideration to rule out infectious cause would be blood-based Karius testing (though this would be fraught with false positives),” wrote that doctor, who was still training as a hematologist-oncologist.
A supervising physician reviewed the Sept. 8, 2023, note and signed off on it. The medical records don’t show any follow-up with infectious disease doctors, and the test wasn’t done at the time.
In the coming days, blood cancer specialists struggled to find a link between Kean’s symptoms and an underlying disease.
They thought he might have a rare form of leukemia, but tests weren’t definitive, Kean texted friends.
Untreated HLH symptoms can lead to rapid organ failure, so doctors often start patients on treatment while trying to figure out the underlying cause, said Gaurav Goyal, a leading national expert on HLH, noting that it can take days to get test results.
“You have to walk and chew the gum. You have to calm the inflammation so the patient doesn’t die immediately, and at the same time, try to figure out what’s causing it by sending tests and biopsies,” said Goyal, a hematologist-oncologist at the University of Alabama at Birmingham.
Medical records show that Penn doctors feared Kean was at “significant risk” of “irreversible organ failure.”
They suggested a more aggressive treatment: a type of chemotherapy used to treat HLH that would destroy Kean’s malfunctioning immune cells.
In his medical record, a doctor noted that beginning treatment without a clear diagnosis was “not ideal,” but doctors thought it was his best option.
Four parasitic disease experts told The Inquirer that chemotherapy, along with steroids and immunosuppressants, can be fatal to patients with visceral leishmaniasis.
“If that goes on long enough, then they kill the patient because the parasite goes out of control,” Libman said, explaining that ramping up the HLH treatments weakens the immune system. “The parasite has a holiday.”
A sample of text messages from Louis-Hunter Kean to friends during separate HUP hospitalizations over a six-month period in 2023.
Chemo as last resort
Kean banked his sperm, because chemo infusions can cause infertility. He told friends he trusted his Penn team and hoped to make a full recovery.
“Started chemo last night. It really feels like finally there is a light at the end of the tunnel,” he texted a friend on Oct. 7, 2023.
“I’m gonna get to marry my best friend, and I think I’m going to be able to have children,” Kean wrote in another text to a different friend.
Kean spent nearly all of October at HUP getting chemo infusions. He rated his pain as a nine out of 10. His joints throbbed. He couldn’t get out of bed. He started blacking out.
Doctors added a full dose of steroids on top of the IV chemo infusion. By the end of the month, Kean told a friend he feared he was dying.
A year had passed since Kean first spiked a fever. He no longer could see himself returning to his former life — one filled with daily exercise, helping run his family’s produce store, nights out with friends at concerts and bars, and vacations overseas.
Lethargic and weak, he could barely feed himself. His sister tried to spoon-feed him yogurt in his hospital bed.
He started texting reflections on his life to friends and family, saying his illness had given him a “polished lens” through which he could see clearly. He wrote that their love felt “like a physical thing, like it’s a weighted blanket.”
“I’ve lived an extremely privileged life. I don’t think it’s possible for me to feel bad for myself,” he said in a text. “And I don’t want anyone else to either.”
Louis-Hunter Kean enjoying dinner out with his sister, Jessica Kean, in Manhattan in 2014. Friends and family described him as a “foodie” and health food advocate prior to the onset of his illness in August 2022.
Puzzle solved
One doctor involved in Kean’s care had seen him at Penn’s rheumatology clinic in early June 2023, just before his first HUP hospitalization. The doctor, a rheumatology fellow,urged him to go to HUP’s emergency department, so he could be admitted for a medical workup.
The fellowremained closely involved in Kean’s care, medical records show. Also in his 30s, this doctor shared Kean’s interests in music, fashion, and the city’s restaurant scene, according to Kean’s family.
“They had a rapport,” Kean’s father, Ted Kean, said. “Louis thought a lot of him, and he seemed to think a lot of my son.”
By early November 2023, the rheumatology fellow was extremely concerned, medical records show.
The chemo infusions weren’t helping. Kean still was running a fever of 103. The fellow wrote in his chart that he was worried Kean needed a bone-marrow transplant to replace his failing immune system.
And doctors still didn’t know the root of his symptoms.
The fellowcontacted the NIH, medical notes show.
An NIH doctor recommended a test to check for rare pathogens, including parasites that cause visceral leishmaniasis,according to family members present when the testing was discussed.
The NIH-recommended Karius test was the same one suggested two months earlier by the Penn hematologist-oncologist in training, but with no follow-up.
File of sign on front of Hospital of the University of Pennsylvania (HUP) taken on Tuesday, March 19, 2024.
On Nov. 16, the fellow got the results. He went to Kean’s bedside.
After five HUP hospitalizations over six months, a single test had revealed the cause of his illness: visceral leishmaniasis.
Kean cried with relief and hugged the fellow, joined by his mother and sister.
“‘You saved my life,’” Kean’s sister, Jessica Kean, recalled her brother telling the doctor. “‘Finally, we know what this is, and we can treat it.’”
Kean’s medical chart was updated to note that he traveled to “Italy in the past,” also noting he had visited Nicaragua and Mexico. A HUP infectious disease doctor consulted with the Centers for Disease Control and Prevention on antiparasitic medications.
Meanwhile, Kean’s nose wouldn’t stop bleeding. He felt light-headed and dizzy, with high fever. Even on morphine for his pain, his joints ached.
“I’ve been struggling, buddy,” he texted a friend on Nov. 20. “This might be the worst I’ve ever been.”
By Nov. 22, he stopped responding to text messages. He began hallucinating and babbling incoherently, family members recalled. “Things went downhill very, very quickly, like shockingly quickly,” his sister, Priscilla Zinsky, said.
When she returned on Thanksgiving morning, he was convulsing, thrashing his head and arms. “It was horrifying to see,” Zinsky said.
Her brother had suffered brain bleeds that caused a stroke. His organs were failing. He had a fungal infection with black mold growing throughout his right lung, medical records show.
Kean was put on life support, with a doctor noting the still-preliminary diagnosis: “Very medically ill with leishmaniasis.”
“Prognosis is poor,” read the note in his Nov. 29, 2023, medical records.
A few hours later, Kean’s family took him off life support. He died that day.
“All of his organs were destroyed,” said Kean’s mother, Lois Kean. “Even if he had lived, he had zero quality of life.”
Portraits of Lois and Ted Kean’s four children decorate a wall at their home in Haddonfield. Their son, Louis-Hunter, died after contracting visceral leishmaniasis, a parasitic infection he likely picked up in Italy. When caught early, it’s treatable with medication. It’s deadly without treatment.
It’s not clear why the parasites began to attack Kean a year after his return from Italy. Healthy people rarely develop severe disease from exposure to the deadly form of the parasite circulating outside the U.S., experts said.
Most people infected by a sandfly “are probably harboring small amounts of the parasite” in their organs, according to Naomi E. Aronson, a leishmania expert and director of infectious diseases at the Uniformed Services University of the Health Sciences in Bethesda, Md.
“Most of the time, you don’t have any problem from it,” Aronson said.
Children under age 5, seniors, and people who are malnourished or immunodeficient are most susceptible to visceral leishmaniasis. Aronson said she worries about people who might harbor the parasite without problems for years, and then become immunocompromised.
Libman, the parasitic expert from McGill, said he’s seen six to 10 patients die from visceral leishmaniasis because doctors unfamiliar with the disease mistakenly increased immunosuppressants to treat HLH during his 40 years specializing in parasite disease.
“That’s a classic error,” he said.
Kean’s case “should be a real clarion call” for infectious disease specialists and other doctors in the U.S., said Joshua A. Lieberman, an infectious disease pathologist and clinical microbiologist who pioneered the leishmania-PCR test at the Washington state lab.
“If you’re worried about an unexplained [fever], you have to take a travel history that goes back pretty far and think about Southern Europe, Iraq, Afghanistan, India, and maybe even Brazil,” Lieberman said.
In the wake of Kean’s death, his family was told that Penn doctors held a meeting to analyze his case so they could learn from it.
An infectious disease doctor called Zinsky, Kean’s sister, to let her know about the postmortem review and shared that doctors discussed that Kean had likely picked up the parasite in Tuscany.
“Why didn’t you guys have this meeting,” she asked, ”while he was alive?”
Editor’s note: This story has been updated to clarify that ECRI President Marcus Schabacker was not speaking specifically on Kean’s case.
At Roxborough Memorial Hospital in Philadelphia, surgeon Piotr Krecioch has his hands full launching a program offering surgical interventions to treat obesity.
One in three Philadelphians are living with obesity, putting them at higher risk of chronic conditions like diabetes and heart disease, but these days fewer are seeking the bariatric surgical procedures long considered a leading medical treatment for the condition.
“I’m trying to start a bariatric program at probably the worst possible time you can ever imagine because everybody’s losing patients, and I don’t even have a patient to begin with,” Krecioch said.
Tower Health’s Reading Hospital recently closed its bariatric surgery program, and other local health systems have seen declines in weight-loss operations approach 50%.
Independence Blue Cross, the Philadelphia region’s largest insurer, said the number of bariatric surgeries it paid for dropped by half in the five years ended June 30.
Those shifts in the bariatric surgery landscape have followed the meteoric national rise in the use of GLP-1s and related drugs for weight loss.
So far, the drugs havebenefited patients by allowing them to avoid an invasive surgery.With bariatric surgery, people lose weight because the procedures restrict the amount of food a person can eat. Drugs in a class known asGLP-1s make people feel full longer.
For hospitals, the upheaval in treatment options cuts into a profitable business line and adds to the financial pressure health systems have been experiencing since the pandemic.
Despite the ever-increasing popularity of GLP-1s for weight loss like Novo Nordisk’s Ozempic and Wegovy and Eli Lilly’s Mounjaro and Zepbound, it’s too soon to write off bariatric surgery as an option, some doctors say.
Insurers are imposing limits on coverage because of the long-term cost of the drugs compared to surgery, and doctors are watching for side effects that may emerge as more people take the drugs for longer periods of time.
It’s not the first time a new technology has reduced surgical volumes.
Whenever a less-invasive treatment has come along, “surgical volumes always have taken a beating,” said Prashanth R. Ramachandra, a bariatric and general surgeon at Trinity Health Mid-Atlantic’s Mercy Fitzgerald Hospital. Declines in peptic ulcer and open heart surgeries are past examples of the phenomenon, he said.
Such industrywide moves away from profitable procedures can create financial challenges for individual clinics or independent hospitals, said Daniel Steingart, who leads the nonprofit healthcare practice at Moody’s, a major credit ratings agency.
“But I also see it as an opportunity, because there’s other patients out there, there’s other services that can be provided. This is a matter of the management team being nimble,” he said.
Sharp decline in bariatric surgeries
National data show a 38% decline in bariatric surgeries from the beginning of 2024 through September, according to data firm Strata Decision Technology. Comparable local data were not available.
A substantial portion of the drop is from patients who previously had bariatric surgery but regained weight, physicians say. In the past, they would have had a type of surgery called a revision. Now, those patients are more likely to start taking GLP-1s, local doctors said.
Prashanth R. Ramachandra is a general and bariatric surgeon at Trinity Health Mid-Atlantic’s Mercy Fitzgerald Hospital in Darby.
Only two Philadelphia-area health systems provided details on changes in bariatric surgery volumes in recent years as GLP-1s for weight loss took off.
At the University of Pennsylvania Health System’s three Philadelphia hospitals, the annual number of bariatric surgeries has fallen by more than half, from a peak of 850 three or four years ago to around 400 in the year that ended June 30, said Noel Williams, a physician who leads Penn’s bariatric surgery program.
At Mercy Fitzgerald in Darby, the number fell from an annual peak in the 220-230 range to about 125 last year, Ramachandra said.
The volume at Mercy Fitzgerald was likely buoyed by the closure of the bariatric surgery program at nearby Crozer-Chester Medical Centerin Upland.
Tower did not provide details on the Reading closure, which was part of cutbacks Tower announced in early November. The program closed last month after a 60-day notice tothe state health department.
Main Line Health, which only offers bariatric surgery at Bryn Mawr Hospital, said surgeries have declined, but provided no details.
Virtua Health did not provide comparable data but said that its Virtua Complete Weight Management Program, which opened in spring 2024 to expand into medication treatments, experienced a 35% increase in visits last year.
The number of bariatric procedures is also down at Temple University Health System, but patients with complex conditions and more severe obesity are still coming to Temple for surgery, said David Stein, who is surgeon-in-chief at Temple University Hospital.
To adapt to this rapid change in medicine, Temple is adopting a multidisciplinary approach to the disease, building on what is done in cancer care, Stein said.
Jefferson Health did not respond to requests for information about its bariatric surgery program.
How health systems are responding
While full-scale closures like Reading’s are unusual, cutbacks are occurring broadly.
When the bariatric surgeon at Penn Presbyterian Medical Center retired amid declining numbers of surgeries across the entire system, Penn did not replace him, Williams said.
Penn does the procedures locally at the Hospital of the University of Pennsylvania and at Pennsylvania Hospital.
“If the numbers were to continue the way they are now,” Williams said, “we may want to consolidate into one of our hospitals in the city.”
Outside of Philadelphia, Penn has bariatrics programs at Lancaster General Hospital and Penn Princeton Medical Center.
After Jefferson Health acquired Einstein Healthcare Network in late 2021, it consolidated bariatric procedures at Jefferson Abington Hospital, according an Inquirer analysis of inpatient data through 2024 from the Pennsylvania Health Cost Containment Council.
Jefferson did not respond to a request for information about the changes.
Piotr Krecioch is a bariatric and general surgeon at Roxborough Memorial Hospital in Philadelphia.
Not the end for bariatric surgery
GLP-1s don’t mean the end of bariatric surgery, even though the procedures are not likely to return to previous peaks, physicians said.
Some patients don’t respond to GLP-1s and others can’t tolerate them, which means they remain candidates for surgery, Williams said. Surgery is still recommended forpatients who are considered severely obese,with body-mass indexes over 50,he added.
Outcomes cannot yet be compared over the long-term. Ramachandra and other doctors are keeping their eye on the ratio of fat loss and muscle loss in patients taking GLP-1s compared to those who have bariatric surgery. Losing muscle can lead to falls and fractures.
A study published last month in the Journal of the American Medical Association found that bariatric surgery is associated with a favorable ratio of fat loss.
At Roxborough Memorial Hospital, Krecioch, who also works as a general surgeon, sounds optimisticas he works on his new program.He became a Roxborough employee in April 2024 after eight years at Mercy Fitzgerald, where he worked with Ramachandra.
Krecioch’s strategy for years has been to offer weight management services in addition to surgery. Patients come for a GLP-1, giving him a chance to build a long-term relationship.
“I have a feeling that these people are going to come back to my office,” he said. ”I’m gonna keep seeing them, and that they will actually convert to bariatric surgery at some point.”
Editor’s note: This article has been updated with information from Temple University Health System.
Philadelphia biotechs are worried about losing a key source of federal funding for early-stage innovation.
Known as “America’s seed fund,” the Small Business Innovation Research (SBIR) and Small Business Technology Transfer (STTR) programs helpsmall companies develop innovative technologies. In recent years, they’ve allocated $4 billion annually to more than 4,000 businesses nationwide. However, after Congress failed to reauthorize the decades-old programs last fall, their funding officially expired in September.
The fallout has affected more than a dozen local life sciences companies, raising concerns about whether they can maintain staffing and make up for thedelay in funds promised months ago, said Heath Naquin, senior vice president of innovation and new ventures at University City Science Center, a nonprofit commonly known as the Science Center that provides startup support.
For many, staffing and financing plans could be disrupted by funding shortfalls, as companies either haven’t gotten their payment yet or can’t get their funding for next year approved, he said.
An exact figure is unknown, but Naquin estimated that some affected companies could be short up to a million dollars for the year.
At the same time, the city of Philadelphialaunched last spring a new program that provides additional funding to those who have already earned SBIR/STTR grants. The 21 awardees who will share $450,000 from the city were announced publicly in January.
The citymoney is earmarked for technical assistance, such as the cost of attorneys, marketing, and anything else needed for commercialization, while SBIR/STTR money normally goes toward research and development.
“There is no overnight solution to SBIR right now,” said Tiffany Wilson, chief executive officer of the Science Center, which is partnering with the city to implement the program. “It’s just another layer of uncertainty that we’ve got to navigate through.”
New city-led program
Pennsylvania is not one of the dozens of states that offer matching programs to supplement the federal SBIR/STTR funds.
To fill that gap, Philadelphia launched its new city-level program, which is one of the first in the nation and the only one of its kind in the state.
The idea was to boost companies already vetted by the federal government that could still benefit from smaller amounts of money.
“Life science companies need millions of dollars, but this was a way that we could help Philadelphia-based companies thrive,” said Rebecca Grant, who runs the program and serves as senior director of life sciences and innovation for the city.
This year, the city offered funding to all eligible applicants.
The $450,000 is doled out in three tiers: companies with the earliest stage grants received $20,000 while those in the next phase received $40,000. Those whose grants were no longer active received $2,500.
The program is still a pilot, and city leaders hope to run it on an annual basis, Grant said.
Naquin has heard from at least three companies in the last six months that are formally considering moving to Philadelphia as a result of the program’s existence.
The SBIR/STTR grants are valuable to early-stage biotechs for two reasons: They provide funding without asking for ownership or equity in return, and signal to potential investors that the company is less risky, Wilson explained.
The programs traditionally have been reauthorized every few years without major lapses. However, recent debates over reforms have created a deadlock.
Policymakers from both parties want to address companies that are repeatedly going back for more funding, concerns over foreign involvement, and how to better support commercialization, Naquin said.
“We’re still in a waiting game,” he said, adding that the programs were not reauthorized in the latest government funding bill passed this week.
With the SBIR/STTR pipeline stalled, the Science Center has had to pivot. Federal support for science has been particularly precarious under President Donald Trump’s second administration, with widespread cuts and pauses to millions of dollars worth of programs and grants.
Late last year, the center launched aninitiative to help startups figure out which agencies still have available funding opportunities.
The aim is to help them better shop around for the grants that they can apply to, Wilson said.
Jefferson Health is boosting emergency department capacity at Abington Hospital to enable it to receive 100,000 visits annually, up from 80,000 now, the nonprofit health system said Tuesday.
The department, which is also a Level II trauma center, will be named the Goodman Emergency Trauma Center in honor of an unspecified donation from Montgomery County residents Bruce and Judi Goodman. Bruce Goodman is a commercial real estate developer and a longtime Abington board member, Jefferson said.
Jefferson, which acquired Abington in 2015, described the Goodman gift as the cornerstone of a $30 million ongoing fundraising campaign for the hospital’s emergency department.
The project will reconfigure more than 24,000 square feet of existing clinical space and reallocate 10,000 additional square feetfrom a courtyard and a gift shop to the ED to expand capacity from 80 to 116 treatment spaces, Jefferson said.
Also last year, Jefferson announced $19 million in upgrades to the emergency department at Thomas Jefferson University Hospital in Center City. The system also added a 20-bed observation unit in the ED at Jefferson Einstein Philadelphia.
Competition at Philadelphia-area medical schools intensified in 2025, with programs seeing about 50 applicants for every open spot.
That’s the highest demand since 2022, with the number of applications bouncing back after a three-year decline, recently released data from the Association of American Medical Colleges(AAMC) shows.
The annual report offers a look at the composition of the nation’s future doctors through the demographics of the applicants and enrollees at M.D. degree-granting medical schools across the United States and Canada.
It showed increased class sizes and strong female enrollment across the Philadelphia area’s five M.D. degree-granting schools: University of Pennsylvania, Thomas Jefferson University, Temple University, Drexel University, and Cooper Medical School of Rowan University.
And the fraction of first-year medical students from Pennsylvania who identified as Black or African American, excluding the mixed-race student population, fell from 6.9% to 5.4% between 2023 and 2025.
The racial demographics of entering studentsare seeing increased scrutiny in light of the 2023 Supreme Court decision that effectively ended affirmative action, barring race from being used in higher education admissions.
The percentage of first-year medical students from Pennsylvania who are Black is lower this year than the national average. Pennsylvania also lags behind the national average for first-year enrollment of Hispanic or Latino medical students.
This data reflects the results of the application cycle that concluded last spring. Next year’s prospective medical school students are currently in the thick of admissions season, awaiting interviews and offers.
Here’s a look at the key trends we’re seeing:
Applications back up
Demand for spots at Philadelphia area-medical schools is back up after a three-year decline. There were nearly 5,000 more applications last cycle, a 9.3% increase, with all schools except Cooper seeing a boost.
Jefferson’s Sidney Kimmel Medical College helped drive growth the most, with a 16% increase in applications compared to the previous year.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
More medical students being trained
Orientation icebreakers might take a bit longer to get through at area-medical schools as first-year classes continue to get bigger.
In 2025, Philadelphia-area schools enrolled 1,089new medical students, compared to 991 in 2017. Drexel University College of Medicine contributed to half of that growth, adding 49 seats to its recent entering class compared to that of 2017.
Penn’s Perelman School of Medicine was the only school that did not increase its class size in 2025.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Female enrollment remains strong
More female students have entered Philly-area medical schools over the last decade.
In 2025, 55.4% of first-year enrollees at Philly-area medical schools were female, compared to 47.7% in 2017.
Drexel saw the biggest rise, with 181 women entering in 2025, compared to 120 in 2017.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
The rollout of so-called virtual nurses in hospitals remains a mixed bag, University of Pennsylvania researchers have found in the largest survey to date on nursing care delivered remotely through a screen.
One hospital staffer said virtual nurses are a huge help getting patients checked in.
Another said they worry hospitals are trying to cut corners by keeping floors fully staffed by using virtual nurses.
And sometimes, patients think the virtual nurse is a television advertisement and try to press fast forward, researchers were told.
A new study out of University of Pennsylvania School of Nursing surveyed 880 registered nurses in 10 states, including Pennsylvania, about the virtual nursing programs that have sprung up at health systems across the country.
About half — 57% — of the nurses surveyed said virtual nurse programs did not reduce their workload, with some saying they felt virtual nurses created more work.
But similar numbers also said they thought virtual nurse programs improved the quality of care patients received.
Others said they didn’t think the technology had any impact — positive or negative — on quality of care, according to a study of results published online in December in JAMA Open Network.
“It can be beneficial or a headache,” one nurse interviewed by Penn researchers summed up.
Virtual nursing programs became more widespread during the COVID-19 pandemic, when health systems needed to limit physical interaction to protect patients and medical staff, and have continued to expand in Philadelphia and across the country. Administrators embracing technology and artificial intelligence say they can help streamline administrative responsibilities that can burden staff, provide extra patient oversight, and improve how quickly clinicians can respond to emergencies.
Local examples include Penn Medicine’s use of virtual nurses to monitor patients at risk of falling or pulling out tubes and wires. Jefferson Health assigns a virtual nurse to patients who doctors have decided need to be monitored around the clock.
And virtual nurses handle administrative work, like reviewing medications and giving discharge instructions at Virtua Health hospitals in New Jersey.
The new study from Penn is among the largest to date to evaluate how well the programs are meeting goals, and the mixed results should be a warning to hospital administrators to proceed cautiously, researchers say.
“Virtual nursing programs have been heralded as an innovative silver bullet to hospitals’ nurse staffing challenges, but our findings show that most bedside nurses are not experiencing major benefits,” said lead author K. Jane Muir, an assistant professor of nursing in the university’s Department of Family and Community Health.
Virtual nursing on the rise
Virtual nurses at Virtua Health appear on the television in a patient’s room.
Virtual nursing refers to patient-care responsibilities managed by a team of nurses stationed at a remote hub, where they monitor screens and electronic information feeds.
They are not intended to replace bedside care, but rather to serve as an extra set of eyes to monitor patients.
If a patient who is known to be unsteady on their feet moves as if to get up from bed, a virtual nurse could speak through a screen or sound system asking if they need something and call a nurse on the floor to help them. If the patient falls, a virtual nurse can quickly alert medical staff.
Virtua Health officially launched its program last year.
Virtual nurses make sure patients have the appropriate medications before going home, know their discharge instructions, and have a follow-up appointment scheduled. They work in partnership with the bedside nurse, who focuses on the physical tasks in caring for a patient, while the virtual nurse handles the majority of the discussion.
“It’s something that our patients are requesting and they’ve come to expect,” said Kristin Bloom, a nurse by training who serves as assistant vice president of clinical operations for Virtua’s Hospital at Home program.
Virtua also uses virtual nurses in its intensive care units to help monitor and identify early signs of deterioration. These nurses have access to bedside cameras and can view the patient’s heart rhythms, lab results, and vital signs.
Participants in the Penn survey, conducted in late 2023 and early 2024, did not include nurses working in New Jersey, where Virtua’s hospitals are based.
Virtual nursing challenges
Nurses surveyed by Penn’s researchers said they appreciated the extra set of eyes on patients, but not all were convinced that the virtual monitor was any more effective than bed alerts that can sound when they sense a patient leaving, according to the study.
Karen Lasater, an associate professor of nursing and co-author of the study, urged health systems to include in-hospital nurses when shaping their virtual care programs.
She said including bedside nurses in the conversation about what’s working and not working is “imperative.”
“It’s important that nurses have a seat at the table,” Lasater said.
Nurses surveyed also expressed concern that health systems were using virtual workers to avoid hiring more on-site staff.
Bedside nurses questioned why they were being asked to take on more responsibility because administrators said they couldn’t afford to hire more staff, yet still found funding to build virtual programs.
“They felt like investments in virtual nursing was a workaround,” Lasater said. “Why did they have money to invest in virtual nurses who couldn’t do all the work of the bedside nurses, but couldn’t invest in more bedside nurses?”
At Virtua, administrators have turned to veteran bedside nurses to staff their virtual nursing program.
“It’s an avenue to retain our experienced nursing staff,” Bloom said.
Philadelphia-area hospitals have seen some virtual nursing challenges. In 2024, for instance, Jefferson Abington Hospital was cited by the Pennsylvania Department of Health after inspectors said the power cords attached to the monitors for virtual nursing created a strangulation risk for behavioral health patients.
The hospital treated the incident as a learning experience, adjusting how the mobile monitors are used.
The technology can also be confusing for some patients, who may not grasp the concept of a virtual nurse or may get conflicting instructions from their virtual and bedside nurses, Lasater said.
Penn initially planned to use virtual nurses to help monitor behavioral health patients, who often require one-on-one monitoring around the clock.
But staff found that patients who were experiencing behavioral or mental health challenges were too often confused or unsettled by virtual nurses, and unable to follow their instructions, Bill Hanson, Penn’s chief medical information officer, told The Inquirer in 2024.
“We’re all learning as we go,” he said at the time.
The Wistar Institute’s long-standing president and CEO Dario Altieri will step down at the end of the year after leading the independent biomedical research institute for 11years, officials announced Monday.
Wistar plans to launch a national search for his successor, but did not share further details.
Altieri joined Wistar in 2010 as its cancer center director and first chief scientific officer. Five years later, he was promoted to the role of president and CEO.
During his tenure, the West Philadelphia-based institute’s annual budget quadrupled to more than $100 million, and its endowment tripled to $277 million, according to a news release.
The number of independent labs also grew from 30 to 41, and two new research centers were created.
Its cancer center, which Altieri directs, received its third consecutive renewal as a National Cancer Institute (NCI)-designated Basic Cancer Center with an “exceptional” rating.
“Due in large part to Dario’s efforts, Wistar is exceptionally well positioned for continued growth and success,” said Rick Horowitz, the board’s chair, in a statement.
The 67-year-old started his career in Milan, Italy, where he underwent his medical training. He has served in faculty roles at the Scripps Clinic and Research Foundation, Yale University, and the University of Massachusetts Medical School.
As a cancer biologist who still leads aresearch laboratory, he has authored more than 260 research papers and been listed as an inventor on 13 patents.
“[I] look forward to dedicating my time to the values of work that have defined me since I was a medical student: laboratory research, teaching and mentoring,” Altieri said in a Monday statement released by the institute.
The Children’s Hospital of Philadelphia and Denver-based Soar Autism Centers have opened in Newtownthe first of five planned early childhood autism centers in the Philadelphia region and expect the network could grow to more than 30 centers, officials said.
The 50-50 joint venture is designed to reduce wait times for therapy and to make it easier for families to access multiple types of therapy at one location while remaining connected to CHOP specialists.
“It can take a year to get into therapy on a regular basis,“ an extremely long time in a young child’s neurological development, Soar cofounder and CEO Ian Goldstein said.
Such wait times continue to frustrate families despite dramatic growth in the autism-services sector over the last 15 years or so, as states mandated insurance coverage and diagnosis rates soared with more awareness and an expanded definition of autism.
Nationally, applied behavioral analysis, commonly known as ABA therapy, has become popular for autism treatment, increasing nationally by 270% between 2019 and 2024, according to Trilliant Health, a Nashville data analysis firm. The volume of services provided locally — where companies including ABA Centers, Helping Hands Family, and NeurAbilities Healthcare have expanded — was not available.
The increase in diagnoses has outpaced the growth in available services, said Matthew Lerner, an autism expert at Drexel University, who is not involved with the newly launched CHOP-Soar Autism Centers.
When Lerner moved to the Philadelphia region from Long Island in 2023 and started getting plugged into the autism network, a few clinicians here would ask if he could connect patients with services in New York.
“I was coming from eastern Long Island, two hours east of New York City, and people were like, do you know anyone closer to you?” he recalled.
CHOP’s road to a joint venture with Soar
The freestanding, 10,000 square-foot clinic that opened on Jan. 5 in suburban Bucks County near CHOP Pediatric Primary Care Newtown has 35 to 40 rooms and an indoor playground for therapeutic uses.
CHOP, among the largest children’s health systems in the country, has longbeen concerned about limited access to autism care in the region, said Steve Docimo, CHOP’s executive vice president for business development and strategy.
The nonprofit hasprovided diagnostic services, but not the forms of therapy that the CHOP-Soar centers will offer. “The threshold to doing this on our own has always been high enough that it hasn’t been a pool that we’ve jumped in,” he said.
CHOP was in talks with Soar for three years before agreeing to the 50-50 joint venture with the for-profit company.CHOP’s investment will be its share of the startup costs for CHOP-Soar locations.
The partnership plan calls for five locations in the first two years. The partners did not say where the next four centers will be.
Soar has 15 locations in the Denver area, which has about half the population of the Philadelphia region, Goldstein said.
That comparison implies that the CHOP-Soar partnershipcould grow to30 centers, Goldstein added. He thinks the region’s needs could support additional expansion, sayingthe total could reach “into the dozens.”
The first CHOP-Soar Autism Center opened this month in Newtown. Shown here is the reception area.
That’s assuming CHOP-Soar provides high quality care for kids, an appealing family experience, and a system of coordinated care: “There will be a need to do more than five, and I think we’re jointly motivated to do so,” Goldstein said.
The CHOP-Soar approach
Families seeking care for an autistic child typically have to go to different places to get all the types of therapy they need.
Families “get behavioral analytics in one place, occupational therapy somewhere else, and speech language pathology in another place,” Docimo said.
Soar brings all of that together in one center. “If it can be scaled, this will fill a gap in our region in a way that I think will work very well for these families,” he said.
CHOP-Soar centers will emphasize early intervention and treat children through age six. “The brain has its greatest neuroplasticity” up to age 3, “so waiting a year is a really big deal,” Goldstein said. “You’re missing out on that opportunity to really influence the child’s developmental trajectory at a young age.”
Some autism services providers focus on ABA therapy, which breaks social and self-careskills, for example, down into components and then works discretely on each.
But Soar offers what Goldstein described as “integrated, coordinated care for the child.” That includes speech, occupational, and behavioral therapies.
With CHOP, medical specialties, such as genetics, neurology, and gastrointestinal care, can be tied in as well, Goldstein said.
It’s rare for autism providers to offer a wide variety of commonly needed services under one roof, said Lerner, who leads the A.J. Drexel Autism Institute’s Life Course Outcomes Research Program.
He said Soar’s evidence-based, multidisciplinary approachhas a lot to offer the region.
“A person diagnosed with autism will have complex care needs throughout their life, and a one-size-fits-all, one-intervention approach will not work,” he said.