The University of Pennsylvania, German biotech firm BioNTech, and Osage University Partners, a Bala Cynwyd venture capital firm, have formed a $50 million fund to back early-stage life sciences startups at Penn, the partners announced Friday.
The announcement came on the eve of the much-hyped annual J.P. Morgan Healthcare Conference in San Francisco, which starts Monday. The conference has become a way to measure the mood of the biotech sector, which has slumped after investment peaked in 2021. It’s been particularly difficult for early-stage biotech companies to raise money in recent years, according to a recent J.P. Morgan report.
For Penn scientists and company founders, the so-called Penn-BioNTech Innovative Therapeutics Seed Fund, or PxB Fund for short, will step into that gap. It is designed to invest in companies that are developing new therapeutics, diagnostics, and research tools.
The announcement did not include a breakdown of how much money each of the three backers provided. Osage University Partners, which has $800 million under management and had previously invested in at least 10 Penn spinouts, will run the fund.
“Penn has a remarkable track record of creating cutting-edge startups,” Marc Singer, an Osage managing partner, said in a statement.
Penn was among the first six universities Osage partnered with 15 years ago when it started investing in spinouts from research universities, while allowing the institutions to share in some of the profits. This was at a time when few universities were investing in their own startups.
Penn’s evolution as an investor in its own startups
For Penn, that began changing about a decade ago. The university’s first investment in one of its own faculty-member spinouts came in 2016, when it invested $5 million in Carl June’s Tmunity Therapeutics. In 2018, Penn Medicine agreed to invest an additional $45 million in Penn biotech companies over three years in conjunction with outside funds.
In December, Penn announced a $10 million fund that will make seed investments of up to $250,000 in companies that have at least one founder affiliated with the University of Pennsylvania. That fund is for the entire university, not just life sciences.
PxB is another part of what John Swartley, Penn’s chief innovation officer, called in an interview Friday a “constellation of different support structures and funding sources that our companies can draw upon in order to advance their opportunities and agenda.”
Anna Turetsky, a biotech investor in New York who received her undergraduate degree at Penn and has a doctorate in biophysics from Harvard University, has joined Osage and will serve as PxB’s general partner.She said PxB is a 10-year fund and is expected to build a portfolio of around 15 companies in the early years.
“Part of why this is a fantastic time to start this fund is that there has been a gap in venture funding for early stage startups over the last few years. Everyone wants to see clinical data these days,“ Turetsky said. If that continues, ”then in a few years, there will be no early-stage clinical companies,” she said.
Germany’s BioNTech, which partnered with Pfizer on one of the COVID-19 vaccines that used mRNA technology developed at Penn, will use the fund to deepen its longstanding ties to Penn researchers.
Philadelphia’s place in biotech
Some observers of Philadelphia’s biotech sector have lamented the relative lack of local investors, which are abundant in places like Boston and San Francisco and have helped turn those metro areas into leading innovation centers.
Quaker BioVentures was a local investment fund that raised $700 million in the early 2000s to buy into biotech firms in Philadelphia and elsewhere, but was not successful for its investors, which included Pennsylvania state pension funds.
Others, when asked why the Philadelphia region trails Boston, San Francisco, and San Diego, as a biotech hub, point to the need for a deeper pool of management talent.
“Part of our hope with the fund is to create some companies, start from scratch, take technology, find management teams, start them in Philadelphia. Hopefully, that will create a new crop of managers,” he said.
Anna Stone was doing the first rounds of her nursing shift at St. Luke’s Upper Bucks Campus when she noticed a patient’s heart rate was elevated, a sign that they could be at risk of a cardiac emergency.
Before she could look into the patient’s chart and decide whether to call for help, a critical care doctor came rushing to the patient’s bedside.
A drop in the patient’s oxygen levels had been detected by a monitor that uses artificial intelligence to continuously evaluate vital signs. This triggered an automatic alert for the hospital’s critical care team to send help.
The AI tool is intended to help doctors and nurses more quickly identify patients whose condition is deteriorating — often before signs of distress are visible to medical staff — and intervene sooner.
The approach contributed to a 34% decline in cardiac arrests, and a 12% drop in patients crashing so hard and fast that they required rapid response transfers to the ICU between 2022 and 2024, according to St. Luke’s.
Survival rates among cardiac arrest patients rose from 24% to 36%.
St. Luke’s experiment with a program called the Deterioration Index, created by healthcare software giant Epic, is among the latest ways hospitals are bringing artificial intelligence into their patients’ rooms.
In other Philadelphia-area initiatives, Jefferson Health and Penn Medicine recently debuted an ambient listening tool that records conversations between doctors and patients, distilling the critical details into a well-organized visit note.
St. Luke’s has been using its AI monitoring system across all 16 of its campuses, including Quakertown, Upper Bucks, and Grand View, which the health system acquired in July.
The health system’s initiative was recognized by The Hospital and Healthsystem Association of Pennsylvania, the region’s largest industry group for hospitals, with an award honoring safety and quality initiatives that improved patient care while reducing hospital costs.
Using AI to predict emergencies
The monitoring device, which attaches to a patient’s finger, records and continuously updates patients’ electronic medical records with vital metrics such as heart rate, blood pressure, and lab work results.
Using this matrix of data points, it assigns each patient a “deterioration index” — a score between 0 and 100 indicating their overall stability — and automatically alerts critical care when the score rises too high.
Matthew Zheng, a doctor at St. Luke’s Upper Bucks, holds the monitoring device used to continuously track patients’ vital signs.
It is not intended to replace in-person monitoring, but serves as an extra set of eyes when nurses are away from their bedside.
What’s more, the sophisticated technology is capable of picking up on nuanced changes in a patient’s status before they show physical signs of distress.
“We would ideally like to intervene on these patients before they reach a point where the intervention isn’t that helpful,” said Matthew Zheng, a critical care doctor at St. Luke’s Hospital — Upper Bucks. “Our nurses work very hard, but they can’t be in the same room all the time.”
When a patient’s “deterioration index” rises above 60, the device sends an alert to the hospital’s virtual response center — a remote hub where a nurse monitors three screens showing the status of all patients.
Alerts may also be sent directly to a patient’s care team or the rapid response unit, if the AI monitoring detects that a patient is quickly deteriorating and needs emergency care.
“What that’s allowed is for us to have a proactive response instead of being reactive to patients,” said Charles Sonday, an associate chief medical information officer at St. Luke’s who leads AI initiatives.
Stone, the Quakertown nurse, said having the tool to constantly watch over patients while she’s out of their room is reassuring.
Doctors like that it enables them to quickly get up to speed on the status of a patient they transferred out of the ICU, and respond more immediately to their new medical needs, said Zheng, the critical care doctor.
St. Luke’s plans to continue fine-tuning the technology, and customize it to meet the unique patient profiles of each of its campuses, which span 11 counties and two states, from the Lehigh Valley to New Jersey.
The social and economic factors that affect patient health, such as pollution, and illness rates, vary significantly across the health system’s sprawling network, Sonday said.
The system will also explore customizing the tool for specialty services, such as pediatrics and behavioral health.
ChristianaCare, Delaware’s largest health system, received a one-notch credit-rating downgrade from Standard & Poor’s, to “AA” from “AA+’.
S&P attributed the downgrade of the nonprofit health system’s rating to inconsistent operating performance in recent years and the planned addition of $350 million in debt early this year through a bond offering, according to a report Tuesday.
In the year ended June 30, 2025, ChristianaCare’s financial results were weaker than expected because of low surgical volume related to physician turnover, S&P said. Another factor was higher-than-anticipated medical malpractice reserves, S&P said.
One of ChrisitianaCare’s financial strengths is that it typically gets half of its revenue from private insurers, which pay higher rates and are more profitable than Medicare and Medicaid, S&P noted.
Despite its strong financial condition, ChristianaCare has a relatively small service area, given its concentration in northern Delaware, compared to other health systems with “AA” ratings, S&P said. If ChristianaCare’s expansion into Southeastern Pennsylvania is successful, it would help alleviate that problem, the agency said.
ChristianaCare opened a micro-hospital in western Chester County last summer and is building a second one in Aston, Delaware County. It also has plans to put one in Springfield Township. In addition, ChristianaCare spent $50 million to step into the leases that the bankrupt Crozer Health had at five outpatient facilities in Broomall, Glen Mills, Media, and Havertown.
S&P said ChristianaCare has no plans for significant acute-care hospital expansion.
Last month, ChristianaCare and Virtua Health, South Jersey’s largest health system, ended negotiations on a possible merger.
University of Pennsylvania researchers recently won a $25 million grant to see if they can fight heart disease with a game that promotesa healthy behavior — walking.
The intervention works by tracking how many steps a person takes each day and assigning points and levels accordingly. Participants get text messages with their daily tally.
The Penn team previously tested the concept in a clinical trial with 1,062 patients and found the approach increased participants’ activity by an average of nearly 2,000 steps daily.
Now, with funding from the nonprofit Patient-Centered Outcomes Research Institute, they hope to show that their game cannot only promote exercise, but can alsoreduce the incidence of heart events.
Dozens of studies have already shown that people who take more steps a day experiencefewer heart attacks and strokes. However, these findings have largely been based on observational data, which is not proof of a cause-and-effect relationship.
The Penn team will be using the $25 million grant to pursue the gold standard for establishing scientific causality: a randomized controlled trial. Patients will get divided into two groups — one gets to play the game, and the other does not — so researchers can compare their outcomes.
Theclinical trial involving 18,000 participants will launch in a year and a half and runfor roughly five years. Patients will be recruited through a partnership with the private healthcare system Ascension, which spans 15 states and the District of Columbia.
Scientists theorize that walking could help by reducing blood pressure, blood sugar, and inflammation. Activity may also improve the way muscles get oxygen from the blood, “so that your heart doesn’t have to work as hard,” said Alexander Fanaroff, a Penn cardiologist and one of the lead researchers on the project.
The researchteam will see whether the participants who had access to the gamesustained significantly fewer instances of stroke, heart attack, or heart failure.
Only people with an elevated risk of heart disease can take part in the trial.
Making walking into a game
As a cardiologist, Fanaroff spends a lot of time telling patients to exercise more.
It doesn’t always work.
“The hardest thing for people to do is change their behavior,” he said.
The Penn team has spent the last decade using concepts from behavioral economics — a field that combines psychology and economics to understand human decision-making — to hone an intervention to promote exercise.
The current program design, which works like a game, is the product of three previous clinical trials that showed the potential of Penn’s game-based approach to improving physical activity.
Here’s how it works:First, participants establish their baseline step count over two weeks, and then set a goal to increase their daily stepsby 33% to 50%.
Each week, patients are given 70 points — that’s 10 per day. Every day that they meet their goal, they keep their points. If they fail to keep up, they lose 10 points.
They move up or down levels each week, based on the cumulative points.
Patients need only to own a smartphone to participate, since their steps are tracked by thebuilt-in sensors now in most devices.
Daily results aredelivered through text.
“If you have an app on your phone, you might not look at it, but if you’re getting a text message every day, you’re engaged,” Fanaroff said.
Participants also identify a support partner, such as a family member or friend, who will get weekly email updates on how the person is doing in the game.
The study is entirely remote, with patients enrolling via a web platform.
Participants who are not sorted into the game approach will receive “usual care,” which consists of medical providers simply telling patients to be more physically active. They will also download a standard exercise app, which normally monitors their steps without turning it into a game.
This includes anybody who has ever had a heart attack or stroke, or received a stent, Fanaroff said. It also includes almost all people over 65 with multiple cardiovascular risk factors such as high blood pressure, high cholesterol, obesity, or diabetes.
“It’s not everybody, but it is a good-sized chunk of the population,” he said.
If successful, he hopes the evidence could convince insurers to fund programs that increase physical activity.
The Penn team estimates the game could be delivered for less than $50 per person.
“If it’s effective at reducing cardiovascular events, it would actually probably be cost-saving to the health system,” Fanaroff said.
He also hopes the results can guide doctors to bettercounsel patients.
“We just don’t know the best way to get people to increase physical activity at all, so all we wind up doing is telling people, ‘Physical activity is important for your health,’” he said.
Despite being one of the rockiest years yet for science — marked by millions of dollars in funding cuts and controversial shake-ups to the federal infrastructure — Philadelphia scientists still managed to celebrate many wins in 2025.
They also won national and international honors for work in physics, cancer research, and drug repurposing. And although no local scientists won a Nobel Prize this year, two at Monell Chemical Senses Center were recognized by its satirical counterpart, the Ig Nobel Prize.
Here are five notable Philly science wins from 2025:
1. Baby KJ is successfully treated with personalized gene editing therapy
Philadelphia-area child KJ Muldoon,now 16 months old, has already been called a “trailblazing baby” by the top scientific journalNature and recognized by the publicationas one of 10 people who helped shape science in 2025.
This international recognition came after his life-threatening genetic condition was successfully treated with a personalized gene editing therapy earlier this year by doctors at Children’s Hospital of Philadelphia and the Hospital of the University of Pennsylvania.
Baby KJ was born in August 2024 with a metabolic disorder that prevented his liver from being able to process protein. Called severe carbamoyl phosphate synthetase 1 (CPS1) deficiency, the disorder puts babies at risk of severe brain damage and is fatal more than half the time.
With few options to treat him, the CHOP and Penn team — led by doctors Kiran Musunuru and Rebecca Ahrens-Nicklas — opted for a gene-editing technology known as CRISPR to create a customized drug for KJ that would fix the genetic mutation that was driving his disease.
After receiving three doses, KJ was able to return home in June — ending his 307-day-long stay at the hospital. Though not a cure, the medication has dramatically improved his liver function and made the effects of his disease milder, doctors say.
2. Penn physicists share the Breakthrough Prize in Fundamental Physics
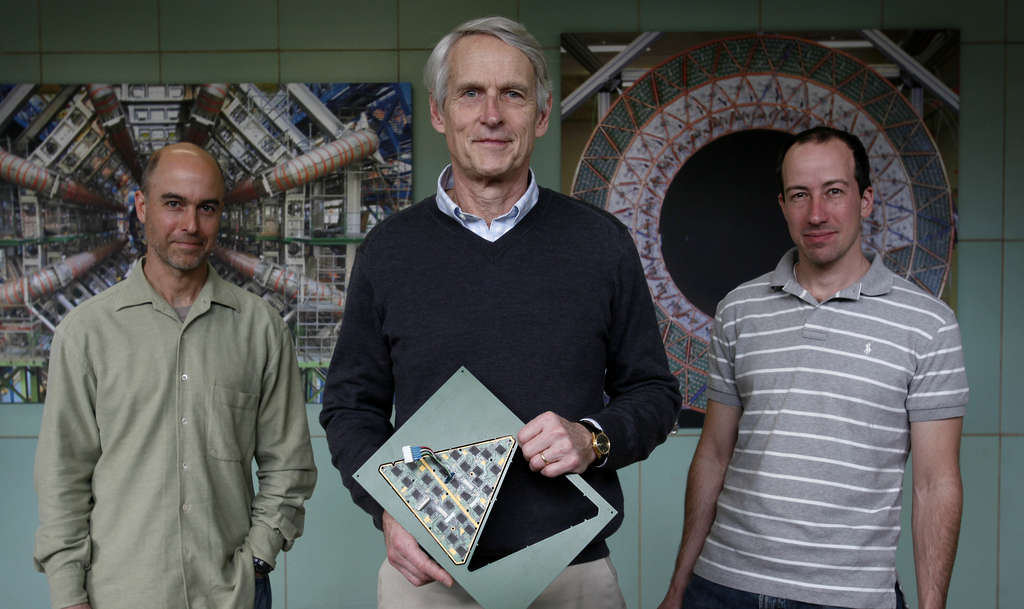
Penn particle physicists (from left) Joseph Kroll, Brig Williams, and Elliot Lipeles, pictured in 2011. They are part of the ATLAS research team that helped discover the Higgs boson, an elementary particle, and were honored with the 2025 Breakthrough Prize for their ongoing Higgs research.
This year, Penn physicists shared one of science’s biggest honors: the Breakthrough Prize.
They were among 13,000 scientists across more than 70 countries to be recognized for their involvement in particle physics experiments at the European Organization for Nuclear Research, known as CERN, in Switzerland.
These decades-long research collaborations have explored the fundamental structure of particles that make up the universe, using CERN’s Large Hadron Collider, a 17-mile-long particle accelerator.
The Penn team — consisting of more than two dozen scientists, including Joseph Kroll, Evelyn Thomson, Elliot Lipeles, Dylan Rankin, and Brig Williams — was specifically part of the ATLAS Experiment, which played a key role in the discovery of the Higgs boson particle, a critical particle in modern particle physics theory. The Higgs discovery helped confirm how fundamental particles acquire mass.
3. David Fajgenbaum honored for drug repurposing research
David Fajgenbaum was diagnosed with Castleman disease, a rare lymph node disorder with limited treatment options. When chemotherapy didn’t work, the third-year medical student worked with his doctors to discover that a medication approved for preventing organ rejection in transplant patients could help him, too.
Penn immunologist David Fajgenbaum received one of the nation’s oldest science prizes, the John Scott Award, this year for his pioneering work repurposing existing drugs for new uses.
He entered this field 15 years ago after a rare and deadly diagnosis of idiopathic multicentric Castleman disease nearly killed him. The disease had no approved treatment nor any treatment guidelines at the time.
Then a medical student at Penn, Fajgenbaum started collecting samples of his blood to test for abnormalities. The data helped him identify an existing drug called sirolimus — primarily given to organ transplant recipients — which has put him in remission for the last decade.
Now through his nonprofit Every Cure, Fajgenbaum has made it his mission to use AI technology to match available medications with rare, hard-to-treat diseases.
He published a case study in the New England Journal of Medicine in February, where his AI tool helped identify an off-label treatment for another patient with Castleman disease who, at the time, was entering hospice care after all available treatments had failed. As of that study’s publication, the patient has been in a yearslong remission.
4. Lilly Gateway Labs biotech incubator coming to Philly
Eli Lilly is opening a branch of Lilly Gateway Labs, an incubator for developing biotech companies, in Philadelphia, the Indianapolis company announced Wednesday. The site, in a new life sciences building at 2300 Market St. in Philadelphia, is the fifth in the United States for the pharmaceutical giant.
Pharmaceutical giant Eli Lilly & Co announced in November its plans to open a Lilly Gateway Labs site — an incubator for early-stage biotech companies — in Center City.
The incubator, which will be Lilly’s fifth in the United States, will span 44,000 square feet on the first two levels of 2300 Market St. Since the program’s launch in 2019, companies at the other locations (in Boston, South San Francisco, and San Diego) have raised more than $3 billion from investors toward more than 50 therapeutic programs, according to Lilly.
Lilly plans to house six to eight companies at the Philadelphia location, with the goal of welcoming the first startups in the first quarter of 2026.
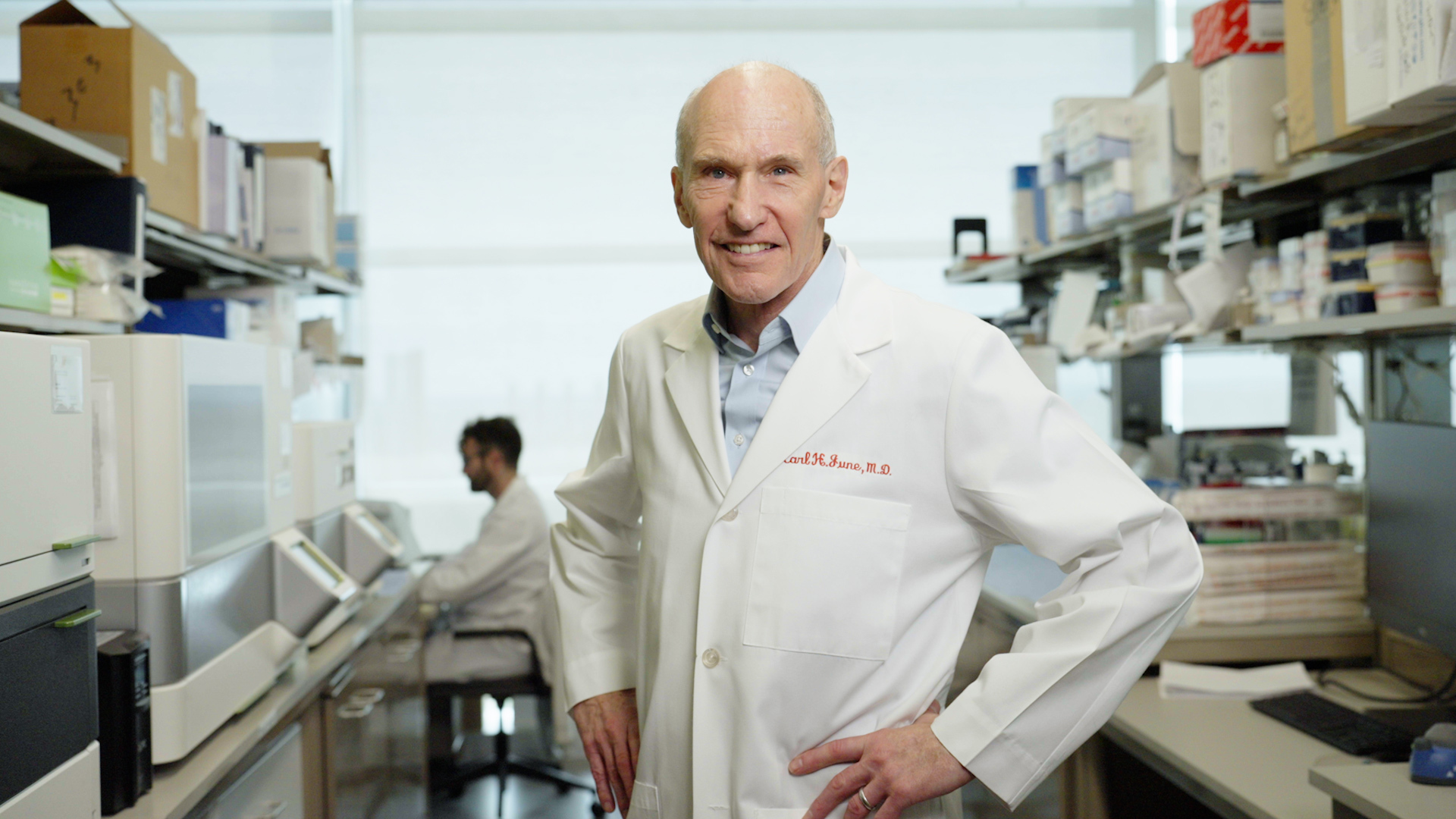
5. Carl June wins international honors for CAR-T research
Carl June won international prizes for his cancer research at the University of Pennsylvania.
Penn cancer scientist Carl June added two more international prizes to his trophy case in September for his pioneering work engineering the body’s immune system to fight cancer.
June is known for developing the first FDA-approved CAR-T therapy, an immunotherapy in which regular immune cells are genetically modified to become cancer-killing super soldiers. It has revolutionized treatment for blood cancers, saving tens of thousands of lives since its first use in a 2010 clinical trial he co-led at Penn.
Though his past work is what won him the inaugural Broermann Medical Innovation Award and the 2025 Balzan Prize for Gene and Gene-Modified Cell Therapy this year, his lab has remained busy, working on ways to apply CAR-T to solid cancers, enhance the therapy for lymphoma, and even re-engineer cells inside the body.
June has also made moves on the biotech front: A company he co-founded with the purpose of applying CAR-T to autoimmune diseases, Capstan Therapeutics, was bought by AbbVie this summer for $2.1 billion.
Nemours Children’s Hospital is launching a new maternal and fetal health program designed to help families with complex fetal diagnoses get specialized care closer to home.
The Institute for Maternal Fetal Health will begin treating patients at Nemours’ flagship hospital in Wilmington in early 2026. The institute’s goal is to provide advanced care for mothers and babies with potentially life-threatening diagnoses, such as congenital heart disease, metabolic disorders, and genetic defects. They may otherwise have had to travel to farther-away hospitals in Philadelphia, Baltimore, Pittsburgh, or New York.
The institute will provide in utero surgery — procedures that are done on a fetus before birth to correct certain debilitating birth defects, such as spina bifida, which is when the spinal column does not completely close and leaves the spinal cord exposed.
It will also offer more education and resources for other family members, especially other children, to help them cope with a fetal diagnosis.
“Our biggest impetus is to help families stay closer to home,” said Julie S. Moldenhauer, a maternal-fetal medicine specialist and the institute’s inaugural executive director.
Julie S. Moldenhauer, a maternal-fetal medicine specialist and fetal interventionalist, is the inaugural executive director of the Institute for Maternal Fetal Health.
Advanced prenatal care at Nemours
The new maternal fetal health institute builds on Nemours growth in the area. The Delaware-based nonprofit health system in 2024 took over pediatric offices previously operated by Crozer Health, which closed under bankruptcy earlier this year.
At its Wilmington hospital, Nemours is adding three new dedicated operating rooms for C-sections, complex deliveries, and fetal surgeries.
The institute will also include more patient rooms and neonatal stabilization rooms for babies who need extra support after birth.
A new wellness room will serve as a place for families to gather for a meal, play time, art therapy, or yoga.
A rendering of a shared patient space planned for the Institute for Maternal Fetal Health at Nemours Children’s Hospital in Wilmington, where families will be able to gather for a meal, play time, or planned activities.
Support for the whole family
For parents, a fetal diagnosis can result in excitement about a new baby being replaced by fear for their child’s health.
What’s more, getting the care they need may involve traveling from home for frequent appointments and procedures. That can be expensive for families who need to take time off work, pay for travel and hotel stays, and find childcare for any siblings remaining home.
“All those hopes and dreams can feel like they’re a candle being blown out,” Moldenhauer said. “Building a beautiful nursery becomes — how are we going to get back and forth to all these appointments?”
When families have to travel for advanced prenatal care, siblings who remain at home may feel left out or scared about whether their parents and the baby will be all right.
At its new institute, Nemours will offer support groups for grandparents, and education for siblings to demystify the medical process.
Psychologists can help couples who are struggling with their relationship during a complex pregnancy, or talk to children who are showing signs of being affected by their parents’ stress.
“Until you see your child with all the tubes in a NICU, in an incubator, it doesn’t feel real,” said Moldenhauer. “We want to fortify the whole family.”
A patient with no home to return to was pushed in a wheelchair to the curb outside Temple University Hospital. Staffers left him sitting on a bench, even though he was considered at a high risk of falling.
An hour later, a security officer found the man had fallen and was lying on the ground.
He was shaking when the guard brought him back into the hospital, but didn’t respond to a nurse’s questions. So hospital staff again sent him away — this time leaving him alone in a wheelchair outside the emergency department.
He was found there five hours later, slumped over, unresponsive, and without a pulse. He died the following week.
Temple’s treatment of the patient during the Oct. 3 incident prompted state and federal investigations. In a report released earlier this month, the Pennsylvania Department of Health cited Temple for violating state rules that require hospitals to provide emergency care.
Experts say the hospital’s actions amounted to “patient dumping,” a practice prohibited under a federal law that requires hospital emergency departments to medically screen and stabilize all patients.
The Centers for Medicare and Medicaid Services (CMS), which oversees hospital safety nationally, confirmed it is also investigating, but has not released details.
Hospitals that violate the Emergency Medical Treatment and Labor Act, known as EMTALA, risk hefty fines or losing their Medicare license, though such penalties are rare.
Temple acknowledged that its own protocols were not followed. Health system officials told state investigators the patient should not have been removed from the hospital without being evaluated and cleared by medical staff.
“The safety of our patients, visitors and staff is Temple’s highest priority,” the hospital said in a statement to The Inquirer. “We believe that everyone deserves high quality care.”
The hospital declined to say whether any of the staff members involved were disciplined or fired.
But such incidents are rarely the fault of one individual, legal experts and homelessness advocates said. Rather, they are a sign of systemic problems, such as understaffing that can leave staff overwhelmed, and bias among medical providers that can put vulnerable patients at risk of being dismissed.
“If you work in an environment where safety is prized and honored and enforced from the top down, everyone feels that’s their mission,” said Eric Weitz, a medical negligence lawyer in Philadelphia. “If that’s not a priority being set by leadership, then it’s no surprise the culture doesn’t reinforce it.”
Hospital administrators said the triage nurse who turned away the patient should have sought help, if the patient wasn’t responding to questions. The nurse said she was overwhelmed and working without sufficient support in one of the region’s busiest trauma hospitals.
“I was busy and alone,” she told state inspectors.
The incident violated Temple’s emergency department protocol, staff told Pennsylvania Department of Health inspectors.
Pa. Department of Health investigates Temple
To piece together what went wrong, Pennsylvania Department of Health inspectors watched security camera footage, interviewed staff members, and reviewed internal hospital reports. Their timeline shows a series of mistakes.
At about 3:15 p.m., an employee brought the patient in a wheelchair to a bench near the curb outside the hospital, and left him there on the mild October day with highs near 70 degrees.
He was being discharged to “the community” because he was experiencing homelessness, according to the inspection report. (The state report does not say whether staff attempted to place him at a skilled nursing facility, rehabilitation center or homeless shelter.)
The man sat alone on the bench for an hour before standing unsteadily, taking a few steps, and ultimately falling to the ground.
He managed to get back up, leaning against a tree for support, only to fall again. He was on the ground for 10 minutes before a security guard found him.
The guard brought the man back into the emergency department in a wheelchair about two hours after he had been released.
Back inside the hospital, the man followed orders to raise his arms for a security check at the door. Then he waited in line to be seen by the triage nurse responsible for checking in patients at the emergency department.
When he reached the front of the line, he did not respond to the nurse’s questions. “He was not answering any questions, just shaking,” according to a Temple incident report reviewed by inspectors. Staff said the patient was “not cooperating” and should be sent to the back of the line.
After two minutes with the nurse, a security guard moved his wheelchair to a corner of the emergency department near the entrance.
The man was once again wheeled outside the hospital a few minutes later and left alone.
He was found by medical staff around 9:30 p.m., slumped over in his wheelchair.
Staff began CPR, rushing him back inside for trauma care.
Pennsylvania Department of Health’s inspection report details how a patient in Temple’s emergency department was rolled away in a wheelchair without being evaluated.
The inspection report does not identify the patient’s name, age, or provide details on the medical condition for which he had been hospitalized. It also does not say what happened after he was found unresponsive. He died five days later, on Oct. 8.
Temple responds
Medical screening of every patient who comes to the emergency department is “explicitly required” under Temple’s EMTALA policies, according to the hospital’s response to the state findings.
“It doesn’t matter if they were just there an hour ago, every time they present, it is a new encounter and should be documented as such,” a Temple staffer said in an interview with inspectors.
The hospital told the state it would retrain staff on EMTALA rules, making clear that security officers cannot remove patients from the emergency department unless they have been evaluated and cleared for release by a medical professional.
A week after the incident, hospital staff were instructed to keep a log of patients who are removed from the emergency department and the name of the provider who approved their release. (Temple police may still remove patients from the emergency department if they are threatening the safety of other patients or staff.)
The hospital also said that it would order mobility evaluations for patients who are being discharged “to the community” if they had a high risk of falling, with a doctor’s sign-off required.
Temple treats some of Philadelphia’s most vulnerable patients in an emergency room that sees more than 150,000 visits a year, including high numbers of gunshot victims and people experiencing opioid withdrawal. It operates a Level I trauma center in a North Philadelphia community where 87% of patients are covered by publicly funded Medicare or Medicaid.
The emergency department is so busy that about 8% of patients choose to leave before being seen, according to CMS data, compared to about 2% of patients at hospitals nationally and across Pennsylvania.
The triage nurse on duty Oct. 3 is not identified in the inspection report.
Two healthcare lawyers who reviewed the state’s inspection report said the entire episode is troubling.
“It sounds like they violated every part of EMTALA,” said Sara Rosenbaum, professor emerita of health law policy at George Washington University.
The law does not require specific treatment, but mandates that hospitals evaluate everyone who walks in the door seeking care, and prohibits them from sending them away or transferring them until they are medically stable.
“They failed to screen him, threw an unstable person back on the street, and didn’t arrange a medically appropriate transfer,” she said.
What’s more, the hospital could be sued for malpractice over how it initially discharged the patient.
The incident appears to be “a classic EMTALA violation,” said Weitz, the Philadelphia lawyer who serves on Pennsylvania’s Patient Safety Authority, an independent state agency that monitors hospital errors.
The health department’s description of what happened is “almost eerily the exact fact pattern the law was passed to prevent,” he said.
Healthcare challenges for patients experiencing homelessness
People who are experiencing homelessness often receive subpar treatment when they seek medical care, research shows.
One study that analyzed thousands of California patient records found that those who were described in their medical records as “homeless” were more likely than patients who have a permanent legal address to be discharged from the emergency department, rather than being admitted for care.
In the Philadelphia region, caring for this population is increasingly challenging. The number of available shelter beds has declined in recent years, while the number of people who are considered unhoused has risen, according to Philadelphia’s Office of Homeless Services.
Stephanie Sena, CEO of Breaking Bread Community Shelter in Delaware County, said the colder months also see more people experiencing homelessness coming to hospitals to get off the street.
“If they say they’re sick, they might get a bed and be able to survive the night,” Sena said.
The pattern can make doctors and nurses less likely to believe patients when they report real medical needs. Especially when staff are overwhelmed in busy hospitals, patients experiencing homelessness may be at greater risk of getting denied or discharged when they need help, she said.
Sena said she was disappointed to hear about the Temple incident.
“It is tragic,” she said, “but also not at all surprising, unfortunately.”
Fox Chase Cancer Center was not cited by the Pennsylvania Department of Health for any safety violations between November 2024 and October of this year.
Here’s a look at the publicly available details:
Feb. 21, 2025: Inspectors came to investigate a complaint but found the hospital was in compliance. Complaint details are not made public when inspectors determine it was unfounded.
March 17: Inspectors came to investigate a complaint but found the hospital was in compliance.
April 15: The Joint Commission, a nonprofit hospital accreditation agency, renewed the hospital’s accreditation, effective January 2025, for 36 months.
Drexel University has signed a lease that will enable it to consolidate its College of Medicine research labs in University City, Drexel and the developers of a new building at 3201 Cuthbert St. said Thursday.
Drexel’s space in the $500 million building, a joint project from Gattuso Development Partners and Vigilant Holdings, is slated for completion in 2027. Drexel researchers moving from sites in Center City and East Falls are expected to fill four floors of the structure.
“By bringing our research spaces together in University City, we will create an environment that fosters greater interdisciplinary collaboration, accelerates innovation, and strengthens our collective capacity for discovery,” Drexel president Antonio Merlo said in a message to the school community.
Drexel will occupy 150,741 square feet of the 11-story, 520,000-square-foot building. The developers’ goal is to fill the rest of the building with life sciences tenants, though that could be harder than it was in 2022, when the building was announced as a partnership between Drexel and Gattuso Development.
The move of research labs to University City is part of a long-term plan to centralize the Drexel College of Medicine, which includes the combined operations of the former Hahnemann Medical College in Center City and the former Medical College of Pennsylvania in East Falls.
ChristianaCare and Virtua Health have ended merger negotiations that would have created a healthcare system with more than $6 billion in annual revenue and business in four states, the two nonprofits announced Thursday.
The nonprofits, the largest in South Jersey and the largest in Delaware, had disclosed a preliminary agreement to join forces in July. ChristianaCare and Virtua did not share specific reasons for dropping the idea.
They issued identical statements: “After thoughtful evaluation, both organizations have determined that they can best fulfill their missions to serve their communities by continuing to operate independently.”
It wasn’t obvious to industry insiders what advantages combining the two systems would have brought other than more revenue and the potential for some relatively small savings from greater scale.
Both systems are financially solid. Virtua has a AA- credit rating from Standard & Poor’s. The S&P rating for ChristianaCare is two notches higher, at AA+.
ChristianaCare explored an acquisition of Crozer Health in 2022, but decided not to go through with the deal. It won a May bankruptcy auction with a $50.3 million bid to assume Crozer leases at five outpatient locations in Delaware County. It has since opened 15 medical practices at those locations.
ChristianaCare previously acquired the shuttered Jennersville Hospital in Chester County and turned it into a micro-hospital. It plans two more micro-hospitals for Delaware County.
The five-hospital Virtua system had $3.24 billion in revenue last year. ChristianaCare, with three full-scale hospitals, had $3.3 billion in revenue in the year that ended June 30, 2025.