A woman in her mid-50s was my fifth patient on a long day treating people with severe chronic pain, all with similar stories. An automobile accident 25 years before left her with severe lower back and neck pain.
At the time of her accident, she was a mother with three small children. Her primary care physician had been treating her for all this time with a relatively high and stable dose of opioid pain medications.
Prescription painkillers were viewed differently when she first began taking these potent medications. It was a common and legitimate medical practice to offer higher doses of opioid medications — so long as the patients required them for pain relief, didn’t abuse them, and didn’t have any concerning side effects.
These medications had given this patient significant relief and had allowed her to raise her children and live a relatively normal life.
With her primary care physician now retiring, she was looking for a doctor willing to allow her to continue her medications, and even slowly taper them under supervision. But she couldn’t find a provider, not even one specializing in pain management, willing to take her on as a new patient.
Eventually, she found her way to me through a referral. I specialize in carefully treating patients with severe pain with the medications that they require to relieve their suffering.
I had heard nearly identical stories from the four patients that I had already treated that morning, all suffering from severe chronic pain. They had previously sought relief through surgery or nerve blocks and procedures like spinal cord stimulators, but they still were suffering from unrelenting pain.
My medical opinion was that the only option available to them at this stage was opioid medication. They had ended up in my clinic, however, because the pain specialists they had been seeing were not willing to increase their doses, even under close supervision.
Twenty-five million Americans suffer from high impact chronic pain — defined as daily pain that negatively affects their quality of life and ability to work. In the 1990s and early 2000s, improper prescribing of opioids by inadequately trained healthcare providers — along with immoral actions and misleading information from some pharmaceutical and medication-supply companies — led to the “opioid crisis.”
Many unwitting patients became addicted to these substances and suffered great harm.
Today, however, I am seeing a new crisis among patients who truly suffer from debilitating, life-limiting, and sometimes life-destroying pain. They cannot get the care they need.
Chronic pain patients are maligned, misjudged, disrespected, and often treated in a punitive way. The overwhelming majority of patients with chronic pain, who are treated appropriately by highly skilled and empathetic physicians, use these medications to help ameliorate severe pain, not because they are looking to get high or satisfy an addiction.
When treated with expertise, they obtain great benefit, and many can resume something of a normal life.
The woman and the four patients whom I had already treated that morning each benefited from higher levels of medication. Each tolerated them without adverse effects, and none abused, diverted, or misused the medications. What had led to our medical system being unwilling to give them the treatment they needed?
Concern about regulatory oversight and potential civil and criminal legal issues have prompted many physicians, including pain specialists, to stop prescribing opioid pain medications. (I cannot explain this contradiction — how can a pain physician not prescribe effective pain medications?)
Many pharmacists also tell me that they are reluctant to dispense these medications, even if the patient has an appropriate prescription from a qualified physician. The pharmacists say that they are under scrutiny by the Drug Enforcement Administration and that their suppliers can be threatened with disciplinary actions if they fill even completely proper prescriptions above their quota.
It’s not unusual for my patients to tell me that they had to call 25 to 50 pharmacies before they found one to fill their prescriptions.
In Pennsylvania, the recent closure of Rite Aid pharmacies has exacerbated the problem. Patients who had been getting their pain medications from Rite Aid are now searching for alternatives. But most of the remaining pharmacies have reached their quotas of controlled medications such as opioids with established patients and are not able to serve new patients.
In some particularly egregious situations, pharmacies have had their entire supply of controlled substances suspended for seemingly minor issues.
I am a pain specialist, caring for many patients with severe pain. Most of my patients have exhausted or failed other potential therapeutic options. Over 90% of my patients who use opioid medications as their last available option get significant pain relief and have improved quality of life.
Yet due to the current situation, I now have many patients who are struggling to obtain these valuable medications, with many also having to deal with symptoms of withdrawal.
Many of my patients often wonder to me why they are punished because of others’ misdeeds and say that they have done nothing wrong and have simply been unfortunate to have suffered injuries and illness, that it’s not fair and is cruel.
It’s time that we begin to correct this travesty. We can treat these patients with expertise. The “opioid crisis” will not worsen by proper and dignified treatment of patients with chronic pain. They certainly deserve our care and their prescribed, helpful medications.
Ira Cantor, M.D., is an internal medicine physician specializing in pain management at Steiner Medical & Therapeutic Center in Phoenixville.
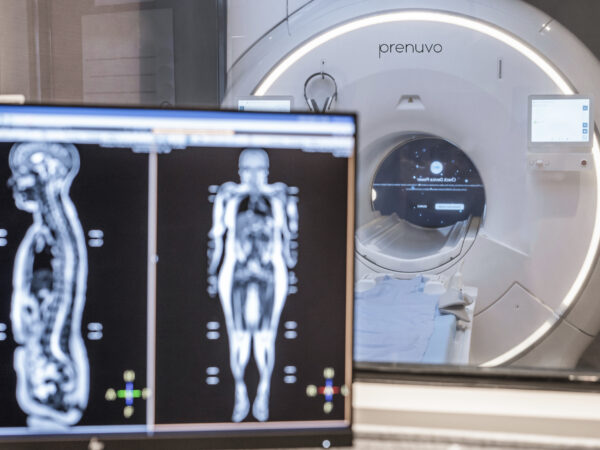
Philadelphia is the newest destination forLilly Gateway Labs, an incubator for early-stage biotech companies backed by pharmaceutical giant Eli Lilly & Co., the companyannounced Wednesday.
The Center City incubator will be Lilly’s fifth in the United States. Biotech hotbeds Boston, South San Francisco, and San Diego already have them. (South San Francisco has two.) Companies at those locations have raised more than $3 billion from investors since the program started in 2019, Lilly said.
Lilly’s Philadelphia operation will occupy 44,000 square feet on the first two levels of 2300 Market St. in Center City.
Lilly expects to house six to eight companies there, aiming to welcome the first startups to the site in the first quarter of next year, said Julie Gilmore, global head of Lilly Gateway Labs. She did not identify prospects.
Typically, Gateway Labs residents are at the stage of raising their first significant round of capital from investors, called Series A, and are two or three years from clinical testing, she said.
The arrival of high-profile Lilly, which has seen resounding success with its GLP-1 drugs for diabetes and weight loss, could turn out to be a shot in the arm for a local biotech scene. Philadelphia has a growing biotech sector but has lagged places like Boston, despite the presence of world-class scientists atlocal research universities.Their work has fueled groundbreaking discoveries in cell and gene therapy, as well as vaccines.
But Lilly is interested in supporting ideas that go beyond the city’s cell and gene therapy strengths, said Gilmore. Gateway labs is part of Lilly’s Catalyze360 Portfolio Management unit, which provides broad support to fledgling biotech firms, including venture capital.
“What we like is to go after innovative science. Who are the companies trying to solve really hard problems?” Gilmore said. “And we do know that Philadelphia has had a ton of success in gene therapy and CAR-T and I hope we can find some great companies in that space, but we’re going to be open to other types of innovative science as well.”
Expanding Philly’s life sciences footprint
Indianapolis-basedLilly already has a small presence in Philadelphia with Avid Radiopharmaceuticals Inc., a company it acquired in 2010. Avid still operates in University City. Lilly’s chief scientific officer, Daniel Skovronsky, founded Avid in 2004 after receiving a doctorate in neuroscience and a medical degree from the University of Pennsylvania.
Lilly is interviewing people to lead Philadelphia’s Gateway Labs location. They like to hire people who are familiar with the local universities and venture funds for those jobs, but that’s not all that matters. “We’re also looking for somebody who’s got deep drug development expertise,” Gilmore said.
Lilly’s incubator adds to the life sciences activity at 23rd and Market Streets.
Breakthrough Properties, a Los-Angeles-based joint venture of Tishman Speyer and Bellco Capital, announced plans for the eight-story, 225,000 square-foot building in 2022. Last week, Legend Biotech, which is headquartered in Somerset, N.J., celebrated the opening of a new cell therapy research center on the building’s third floor.
Lilly Gateway Labs companies agree to stay for at least two years, and they can apply for up to another two years, Gilmore said.
“The goal is, a company moves in and they can just worry about their science, worry about their team, and moving their mission forward, and we try to take care of everything else,” she said.
Ronald Klein was biking around his neighborhood in North Wales in 2006 and tried to jump a curb. “But I was going too slow — I didn’t have enough momentum,” he recalled.
As the bike toppled, he thrust out his left arm to break the fall. It didn’t seem like a serious accident, yet “I couldn’t get up,” he said.
At the emergency room, X-rays showed that he had fractured both his hip, which required surgical repair, and his shoulder. Klein, a dentist, went back to work in three weeks, using a cane. After about six months and plenty of physical therapy, he felt fine.
But he wondered about the damage the fall had caused. “A 52-year-old is not supposed to break a hip and a shoulder,” he said. At a follow-up visit with his orthopedist, “I said, ‘Maybe I should have a bone density scan.’”
As Klein suspected, the test showed he had developed osteoporosis, a progressive condition, increasing sharply with age, that thins and weakens bones and can lead to serious fractures. Klein immediately began a drug regimen and, now 70, remains on one.
Osteoporosis occurs so much more commonly in women, for whom medical guidelines recommend universal screening after age 65, that a man who was not a healthcare professional might not have thought about getting a scan. The orthopedist didn’t raise the prospect.
When they do, “men have worse outcomes,” said Cathleen Colón-Emeric, a geriatrician at the Durham VA Health Care System and Duke University and the lead author of a recent study of osteoporosis treatment in male veterans.
“Men don’t do as well in recovery as women,” she said, with higher rates of death (25% to 30% within a year), disability, and institutionalization. “A 50-year-old man is more likely to die from the complications of a major osteoporotic fracture than from prostate cancer,” she said.
(What’s “major”? Fractures of the wrist, hip, femur, humerus, pelvis or vertebra.)
In her study of 3,000 veterans ages 65 to 85, conducted at Veterans Affairs health centers in North Carolina and Virginia, only 2% of those assigned to the control group had undergone bone-density screening.
“Shockingly low,” said Douglas Bauer, a clinical epidemiologist and osteoporosis researcher at the University of California-San Francisco, who published an accompanying commentary in JAMA Internal Medicine. “Abysmal. And that’s at the VA, where it’s paid for by the government.”
But establishing a bone health service — overseen by a nurse who entered orders, sent frequent appointment reminders, and explained results — led to dramatic changes in the intervention group, who had at least one risk factor for the condition.
Forty-nine percent of them said yes to a scan. Half of those tested had osteoporosis or a forerunner condition, osteopenia. Where appropriate, most of them began medications to preserve or rebuild their bones.
“We were pleasantly surprised that so many agreed to be screened and were willing to initiate treatment,” Colón-Emeric said.
After 18 months, bone density had increased modestly for those in the intervention group, who were more likely to stick to their drug regimens than osteoporosis patients of either sex in real-world conditions.
The study didn’t continue long enough to determine whether bone density increased further or fractures declined, but the researchers plan a secondary analysis to track that.
The results revive a longtime question: Given how life-altering, even deadly, such fractures can be, and the availability of effective drugs to slow or reverse bone loss, should older men be screened for osteoporosis, as women are? If so, which men and when?
Such issues mattered less when life spans were shorter, Bauer explained. Men have bigger and thicker bones and tend to develop osteoporosis five to 10 years later than women do. “Until recently, those men died of heart disease and smoking” before osteoporosis could harm them, he said.
“Now, men routinely live into their 70s and 80s, so they have fractures,” he added. By then, they have also accumulated other chronic conditions that impair their ability to recover.
With osteoporosis testing and treatment, “a man could see a clear-cut improvement in mortality and, more importantly, his quality of life,” Bauer said.
Both patients and many doctors still tend to regard osteoporosis as a women’s disease, however. “There’s a bit of a Superman idea,” said Eric Orwoll, an endocrinologist and osteoporosis researcher at Oregon Health & Science University.
“Men would like to believe they’re indestructible, so a fracture doesn’t have the implication that it should,” he added.
One patient, for example, for years resisted entreaties from his wife, a nurse, to “see someone” about his visibly rounded upper back.
Bob Grossman, 74, a retired public school teacher in Portland, blamed poor posture instead and told himself to straighten up. “I thought, ‘It can’t be osteoporosis — I’m a guy,’” he said. But it was.
Another obstacle to screening: “Clinical practice guidelines are all over the place,” Colón-Emeric said.
Professional associations like the Endocrine Society and the American Society for Bone and Mineral Research recommend that men 50 and older who have a risk factor, and all men over 70, should seek screening.
The task force’s position means that Medicare and many private insurers generally won’t cover screening for men who haven’t had a fracture, though they will cover care for men diagnosed with osteoporosis.
“Things have been stalled for decades,” Orwoll said.
So it may fall to older men themselves to ask their doctors about a DXA (pronounced DECKS-ah) scan, widely available at $100 to $300 out-of-pocket. Otherwise, because osteoporosis is typically asymptomatic, men (and women, who are also undertested and undertreated) don’t know their bones have deteriorated until one breaks.
“If you had a fracture after age 50, you should have a bone scan — that’s one of the key indicators,” Orwoll advised.
Other risk factors: falls, a family history of hip fractures, and a fairly long list of other health conditions including rheumatoid arthritis, hyperthyroidism, and Parkinson’s disease. Smoking and excessive alcohol use increase the odds of osteoporosis as well.
“A number of medications also do a number on your bone density,” Colón-Emeric added, notably steroids and prostate cancer drugs.
When a scan reveals osteoporosis, depending on its severity, doctors may prescribe oral medications like Fosamax or Actonel, intravenous formulations like Reclast, daily self-injections of Forteo or Tymlos, or twice-annual injections of Prolia.
Lifestyle changes like exercising, taking calcium and vitamin D supplements, stopping smoking, and drinking only moderately will help but aren’t sufficient to stop or reverse bone loss, Colón-Emeric said.
Although guidelines don’t universally recommend it, at least not yet, she would like to see all men age 70 and up be screened, because the odds of disability after hip fractures are so high — two-thirds of older people will not regain their prior mobility, she noted — and the medications that treat it are effective and often inexpensive.
Klein remembers attending a seminar to instruct patients like him in using the drug Forteo. “I was the only male there,” he said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism. The New Old Age is produced through a partnership with The New York Times.
Philadelphia’s nonprofit Center for Advocacy for the Rights and Interests of Elders, known as CARIE, is closing next Wednesday after nearly 50 years, the organization’s board announced Tuesday in an email to supporters.
Few details were available on what led to the decision to close abruptly the day before Thanksgiving. CARIE’s new executive director, Brian Gralnick, did not reply to an email or voicemail asking for more information.
Board chair Joan Davitt, an associate professor and geriatric scholar at the University of Maryland School of Social Work who lives in the Philadelphia area, also did not respond to requests for comment.
The organization lists 26 employees on its website. Its most recent audited financial statements show that it had $2.9 million in revenue and a $177,307 operating loss in the year that ended June 30, 2024.
An unaudited financial report for the seven months that ended in January warned that CARIE “was facing financial risks, including the potential default on its line of credit.” At the end of January, CARIE only had enough cash to pay its bills for two weeks, the report obtained by The Inquirer said.
This year, CARIE lost two of its largest contracts, effective next year. Those contracts were to provide long-term care ombudsman services for the elderly in most of Philadelphia and in Montgomery County. An ombudsman’s job is to provide independent advocacy for residents of long-term care facilities and to help resolve complaints about care and living conditions.
In Philadelphia, CARIE had provided the service since 1981, four years after its founding. Philadelphia Corporation for Aging, which manages the contracts, is still finalizing the selection of the new providers.
CARIE started providing ombudsman services in Montgomery County in 2022, but the county’s Office of Aging Services is taking the service back in-house on Feb. 1.
Menio’s successor, Whitney Lingle, lasted just 19 months. She was followed by an internal acting executive director for a year. Gralnick took over in September.
It’s official. Medicare costs will eat up much of older Americans’ Social Security cost-of-living increase next year.
The standard monthly premium for Medicare Part B, which covers outpatient care, doctors’ services, durable medical equipment and preventive service, will be $202.90 in 2026, the Centers for Medicare and Medicaid Services said on Nov. 14. That’s up $17.90, or nearly 9.7%, from $185.00 in 2025.
It’s smaller than the $21.50 increase the Medicare Trustees had forecast earlier but still the second largest dollar jump in program history behind 2022’s $21.60 gain and almost 3.5 times the 2.8% Social Security raise for next year. That means seniors will probably see a drop, again, in their standard of living, experts said.
Seniors were the only ones who saw an increase in poverty in 2024. All other age groups saw a decrease or stayed the same.
“The public is likely to perceive this Part B increase as taking a significant chunk of or even most of their COLA,” said Mary Johnson, independent Social Security and Medicare policy analyst. “In other words, another continuation in relentless cost increases battering consumer finances.”
Monthly Social Security checks will rise $56, on average, starting in January because of the 2.8% COLA, the Social Security Administration said. After the $17.90 increase in Medicare Part B, the average monthly COLA increase is cut to $38.10.
Hold-harmless provision
Such a large increase in Medicare Part B will likely trigger the hold-harmless provision for Social Security recipients with a Social Security benefit of $640 or less, Johnson said.
The Medicare hold-harmless provision prevents the Part B premium increase from being larger than the Social Security COLA. If a premium increase is higher than the COLA, the rule prevents the beneficiary from paying the full increase. The portion of the increase those beneficiaries don’t pay is spread out among others who aren’t protected by the rule.
For those people with a Social Security benefit of $640 or less, the 2.8% COLA next year would mean just less than an $18 per month increase in their Social Security checks. Without the hold-harmless rule, the Part B premium increase would swallow the entire COLA.
In 2022, only about 1.5% of Medicare beneficiaries had their Part B premiums limited by the hold-harmless provision, government data showed. Part B rose $21.60 to $170.10 in 2022 while the average monthly COLA increase boosted Social Security checks by $92.
In 2017, when Medicare premiums jumped 10%, or $12.20, to $134.00 and far outpaced the 0.3%, or $5 average, monthly COLA increase, 70% of Medicare Part B enrollees paid a lower-than-standard Part B premium due to the hold-harmless provision.
Hold-harmless rule isn’t panacea for all costs
The hold-harmless provision can protect seniors from Part B premium surges, but other costs may bite, Johnson said.
“If individuals have other automatic deductions such as for Medicare Advantage or Part D premiums, increases in those premiums could reduce Social Security benefits,” Johnson said. The optional Part D covers prescription drugs.
Some Part D plans are increasing premiums by as much as $50 in 2026, the maximum allowed under a Part D Premium Stabilization Demonstration Program, according to the nonprofit, nonpartisan research organization KFF.
“To complicate things, there are fewer stand-alone Part D plans to choose from,” Johnson said. The total number of prescription drug plans has dropped by half since 2024, KFF said.
Is everyone eligible for hold harmless?
Those who aren’t eligible for the hold-harmless provision include:
New Medicare enrollees
People who aren’t receiving Social Security benefits
High-income earners
What about deductibles?
In addition to higher premiums, higher annual deductibles next year will make health insurance even more expensive for Medicare enrollees.
The annual deductible for all Medicare Part B beneficiaries before insurance covers costs will be $283 in 2026, up $26 from $257 in 2025, CMS said.
Could it have been worse?
The Part B premium could have been higher, CMS said.
“If the Trump Administration had not taken action to address unprecedented spending on skin substitutes, the Part B premium increase would have been about $11 more a month,” CMS said. “However, due to changes finalized in the 2026 Physician Fee Schedule Final Rule, spending on skin substitutes is expected to drop by 90% without affecting patient care.”
Skin substitutes are materials like biologic, synthetic or biosynthetic products that mimic human skin and are used to cover and treat chronic wounds, such as diabetic foot ulcers. The Trump administration reclassified these bandages so they aren’t billed separately. CMS estimates the change would reduce Medicare spending on these products by nearly 90% in calendar year 2026.
Medicare Trustees also estimated earlier this year the standard monthly Part B premium would rise $21.50 to $206.50 in 2026 from $185 in 2025. That would have been more than the $17.90 increase to $202.90 in 2026.
For more than three decades, Marion Nestle has been telling people what to eat.
In the late 1980s, she edited the first Surgeon General’s Report on Nutrition and Health, then went on to cowrite the federal government’s Dietary Guidelines for Americans and cofound New York University’s influential food studies program.
Nestle, now an emerita professor at NYU, says her time in government opened her eyes to the multi-billion-dollar food industry’s enormous influence over Congress. By the early 2000s, she became a critic of the food industry and an advocate for major food reforms, which she made the case for in best-selling books.
In 2002, Nestle published Food Politics, an exposé that argued that the food industry is at the root of many of the country’s nutritional problems. The industry rakes in ever-growing profits by churning out highly processed foods laden with additives, Nestle wrote, and then aggressively markets those foods to children and adults while lobbying against regulations and trying to co-opt nutrition experts.
Over the years, Nestle’s blunt nutrition advice, sharp criticism of food companies, and frequent media appearances made her one of the most recognizable names in nutrition. In 2006, she published one of her most popular books, What to Eat, which showed consumers how to navigate supermarkets and improve their health by deciphering food labels.
At age 89, Nestle, who lives in New York City and Ithaca, is still going strong. In November, she published her latest book: What to Eat Now: The Indispensable Guide to Good Food, How to Find It, and Why It Matters.
We wanted to know how Nestle’s knowledge of nutrition and the food industry affects her daily food decisions. So we caught up with her to find out what she eats in a typical day, which foods she loves and avoids, which “junk foods” she can’t resist, and whether she takes supplements or has advice on how to navigate grocery stores. This interview has been edited for length and clarity.
Q: What’s your general approach to food?
A: I follow Michael Pollan’s famous mantra: Eat food, not too much, mostly plants. And I define food as being unprocessed or as minimally processed as possible. Not ultra-processed. I really think that takes care of it. That doesn’t mean I’m perfect. I’m an omnivore. I eat everything. I just don’t eat very much in part because metabolism drops with age, and I don’t have much metabolism left.
I eat pretty healthy, but I don’t obsess about it. If I have a bad day of eating, I don’t worry about it. By this time, it’s pretty clear I’m not going to die prematurely. Obviously, what I’m eating is working for me because I’m 89 and I’m still here.
Q: What do you eat for breakfast?
A: I start with coffee between 8 and 9 a.m. I’ll have a couple cups of weak coffee with milk, no sugar. And then I’m at work. That’s when I do my writing. I don’t get hungry until about 10:30 or 11 a.m. That’s when I’ll usually have oatmeal or unsweetened Post Shredded Wheat cereal. It basically has one ingredient: wheat. I like the texture of Shredded Wheat and the way that it tastes. I add a little brown sugar, not much. I use a lot less sugar than what’s in presweetened cereals. And then I’ll add blueberries or whatever fruit is in season. That combination to me is really appealing.
I’ve never believed any of the research on breakfast being the most important meal of the day. Most of that was sponsored by cereal companies.
Q: What about lunch?
A: My lunches are totally irregular. Sometimes I’ll have a salad for lunch. Or if I’m having lunch with someone then I’ll eat whatever is in the restaurant. If I’m at home in New York City, I’ll harvest whatever is growing on my terrace. The peaches, cherries, raspberries, and blueberries that I was growing are long gone. But I’ve still got some lettuce and tomatoes, so I’m going to go out and pick those. I might cut up some cheese or have it with peanuts. And I might have some bread with that.
Q: What about dinner?
A: It depends. I just don’t eat that much. But I do really like salads. I can have salads twice a day. If I’m at home, I might have an egg. I might have crackers and cheese with that. I kind of like making meals based on what I have available. So, it depends on what I bought, what’s in the house, or what’s on the terrace. That’s my favorite way of cooking. We have a garden in Ithaca, there’s a garden on my terrace, and there’s a farmers market not very far from here.
I also go to a lot of neighborhood restaurants. I’m going to Mark Bittman’s restaurant this week — the kitchen that he started in the East Village where people pay according to their income. I’ll eat whatever they’re serving. One restaurant that I like a lot is il Buco Alimentari & Vineria. I love going there. They have a particular salad that I adore. It’s always so crisp, and they have wonderful pasta dishes.
Q: What are some foods that you love?
A: Fortunately, I like a lot of very simple foods. I like vegetables. I like eggs. I like cheese. I do eat some ultra-processed foods. But not a lot of them. I don’t like ultra-processed foods that have a long list of ingredients. Most of those don’t taste good to me. I do really like vegetables. I like the crunch, the flavors, and the colors. That makes it easy to eat healthy.
But I recognize that I’m privileged. I weigh basically what I weighed when I was in high school. I don’t have a weight problem. And I have an enormous amount of sympathy for people who do. I consider myself extremely fortunate. Is it genetics? I have no idea. My father died of a heart attack at the age of 47. He was an obese three-pack-a-day smoker. It’s hard to know where genetics fits into this.
Q: Do you have any favorite treats or desserts?
A: Ice cream. When I’m at home in New York City, I try to find ginger ice cream, which I like very much. It’s hard to find. But when I find it, I buy it. And then my partner and I make homemade vanilla ice cream in Ithaca. It’s only three or four ingredients. It’s ruined other ice creams for me because a lot of commercial ice creams have all these emulsifiers in them that keep the ice cream sticking together. Real ice cream completely falls apart if it’s left at room temperature and not eaten right away. It separates and liquefies. But I like that. I think it tastes better and has a better texture than the commercial ice creams that have emulsifiers. I like ice cream without the emulsifiers.
Q: What about snacks?
A: I like corn chips. Not too salty. Some corn chips are ultra-processed, although most are not. The ones I like are Wegmans. They only have a few ingredients — just corn, oil, and salt basically. I also like candy, particularly See’s Candies. The one See’s candy store in New York is just a couple blocks away from me. I normally get the peanut brittle. Sometimes the lollipops. I can have these things in the house and not feel like I have to eat all of them all at once. Not everyone can do that.
Q: Can you tell us about your new book?
A: It’s called What to Eat Now. It’s the updated edition of What to Eat, which was published 20 years ago. It’s a completely rewritten book. I thought it was going to be a six-month project, and it ended up taking me four years because so much has changed in grocery stores. There’s been a huge turnover in products. For example, “functional waters” that contain vitamins, minerals, cannabis, supplements, and other things have replaced Coca-Cola and plain water. Plant milks are new. The only plant milk that existed 20 years ago was soy milk. Now there are tons of others. Plant-based meats did not exist 20 years ago — at least not in the way that they do now.
Q: What is one takeaway from the book?
A: It’s not a book about personal diets. It’s a book about how to think about food issues. I think what to eat now boils down to eat food, not too much, mostly plants.
Q: Do you take any supplements?
A: I don’t take supplements because I eat a healthy diet. I don’t think I need them. But two out of three Americans take supplements. They make people feel better — and it’s hard to argue with that. Life is tough. If all it takes is a supplement to make you feel better, then I’m not going to argue with that. I used to be much more upset about supplements. But now it’s clear to me that they make people feel better. Whether that’s because they’re doing something or because they’re a placebo, it’s hard to know.
But I don’t trust what’s in them. There’s so much evidence that what the label says isn’t what’s actually in them. Many studies have found that a remarkable percentage of supplements do not actually contain what’s listed on their labels. I don’t want to put something in my body if I don’t know what’s in it. And there are things in supplements that are not supposed to be there — that’s what so many studies have found. It’s not true of all supplements. But it’s very hard to know which ones are OK and which ones are not. So I don’t take any of them.
Q: Do you have any advice for our readers?
A: Eating healthfully in today’s society is very difficult because you’re fighting an entire food industry on your own— and that industry is trying to sell you the most profitable, least healthy foods available. But one thing you can do is read food labels. There’s a lot of information on them. If you’re looking at a packaged food and you can’t recognize the ingredients, or if you can’t purchase the ingredients at a supermarket, then it’s ultra-processed. There are certain ingredients that are indicators of ultra-processed foods. That would be color additives, flavor additives, and emulsifiers such as mono and diglycerides, polysorbates and carrageenan, and texturizers such as agar. I always read food labels. If something has a lot of artificial additives and ingredients that I don’t recognize, then I’m not going to eat it.
Marathon weekend is finally here and while the races are unquestionably the main event, runners and spectators alike look forward to seeing fun signs along the route.
However, there are some exceptions. “There are two signs people hate,” said Gary Brown Jr., founder and co-leader of the local running group Chasing Trail Philadelphia, “‘You're almost there’, especially when you're at, like, you know, Mile 13, and then ‘Worst parade ever’.”
As a city, let’s not add to Gary’s list. Use our sign generator to get some ideas.
What kind of sign are you going for?
What type of sign do you want to make?
story continues after advertisement
If you have other ideas or see a particularly creative sign, drop us a line at interactives@inquirer.com.
Marathon weekend can look chaotic — thousands of runners, crowds along the Parkway, and traffic everywhere — but it can also be one of the most fun, kid-friendly days in Philadelphia.
Between the Nemours Children’s Run, the Health and Fitness Expo, easy cheering spots, and plenty of stroller-friendly food stops, there’s a lot for families to enjoy without getting overwhelmed.
Here’s how to navigate the Philadelphia Marathon with kids in tow.
📍 Eakins Oval (22nd St. & Benjamin Franklin Parkway)
Kids run age-specific, short-distance dashes along the Parkway and get an event T-shirt, a finisher medal, and special goodies.
Nothing is timed, so the emphasis is fun. Children may only run in their age group, and each child is limited to one race. A parent or guardian must be present, but adults can’t run with the kids.
Come early. Before the races, kids can enjoy:
sports zone (football, baseball, basketball, soccer)
Runners on Walnut Street in Center City during the 2024 Philadelphia Marathon Sunday, Nov. 24, 2024.
Best viewing spots with kids
The marathon route stretches across Center City, Fairmount, and Manayunk. These spots are easiest for families:
Chestnut Street at Mile 1: High-energy, big crowds, and runners come through early — good for short attention spans. There’s room on side streets for stroller parking.
34th Street / University City (around Mile 5 and Mile 13): Wide sidewalks, walkable from the Parkway, and you can catch runners twice here if you hustle.
Manayunk’s Main Street (Miles 19–21): The loudest, most festive part of the race — think music, costumes, cowbells. Great for older kids; may feel crowded for toddlers.
Kelly Drive (Miles 22–24): Quieter stretch with room to spread out. Better for small kids and families who want to avoid packed sidewalks.
Cheering tip for kids: Have them call out runners’ names from their bibs — runners light up when a kid yells their name.
Getting Around: Transit, biking, and parking for families
Getting to the start/finish near the Art Museum is doable — especially with public transit.
SEPTA (big perk for parents)
Children 11 and under ride free with a fare-paying adult. Buses that usually stop near the Parkway (7, 32, 33, 38, 43, 48, 49) may be detoured. Check SEPTA’s System Status before you head out.
Regional Rail is helpful if you’re heading to Manayunk to cheer between Miles 19 and 21.
Driving & parking
Road closures are extensive, so expect detours and delays. If you plan to drive with kids, park early.
Amanda Carter and her children, Quinn, 3, and Cameron, 5, pose for a photo at 16th and Arch Streets at the start of the 2024 Philadelphia Marathon Sunday, Nov. 24, 2024. The kids had masks with dad Ron Carter’s face. They’re from New York City and this is Ron’s first marathon. Amanda who had done three, says “’m usually the one running.”
Kid-friendly sign ideas
If your kid needs inspiration, try:
You’re super fast! Like superhero fast!
Don’t stop! You’re almost at the snacks!
Run like you’re chasing the ice cream truck!
Go Birds! (And go YOU!)
My arms are tired from holding this sign!
My mom trained for months — I made this sign in five minutes!
Or have them tap through our Sign Generator for more options.
The gyros platter from Moustaki.
Where to eat with kids along the route
Whether you need a quick warm-up or a post-race reward, we rounded up 10 family-friendly places along (or just off) the course — from dumplings and giant slices to pancakes, burgers, and big dining rooms made for strollers.
William L. Elkins, 93, of Coatesville, pioneering research immunologist at what is now the University of Pennsylvania’s Perelman School of Medicine, associate professor emeritus of pathology and laboratory medicine, innovative longtime Angus cattle rancher in Chester County, avid sailor, and veteran, died Tuesday, Nov. 11, of complications from pneumonia at Chester County Hospital.
The great-great-grandson of Philadelphia business tycoon William Lukens Elkins, Dr. Elkins fashioned his own distinguished career as a scientist, medical researcher, and professor at Penn from 1965 to 1985, and owner of the Buck Run Farm cattle ranch in Coatesville for the last 39 years.
At Penn, Dr. Elkins conducted pioneering research on how the human immune system fights infection and disease. He collaborated with colleagues in Philadelphia and elsewhere around the country to provide critical new research regarding bone marrow transplants and pediatric oncology.
His work contributed to new and more effective medical procedures at Penn, Children’s Hospital of Philadelphia, and elsewhere, and he instructed students and residents at Penn. But his lifelong love of the fields and rolling hills he roamed as a boy in Chester County never faded, he told Greet Brandywine Valley magazine in 2023.
Dr. Elkins was a lifelong outdoorsman.
“Farming is in my blood,” he said. “So even when I went to medical school and all that, the enthusiasm never left, and I wanted to go back to it.”
So he retired from medicine at 53, and he and his wife, Helen, bought nearly 300 acres of the old King Ranch on Doe Run Church Road in Coatesville. She kept the books and looked after the business. He became an expert on breeding cattle and growing the high-energy grass they eat.
Wearing floppy hats and riding a colorful ATV from field to field, Dr. Elkins worked his land for decades. He mended fences and tended daily to his 120 cows, heifers, and prize bulls.
He championed holistic regenerative farming and used new scientific systems to feed his cattle. He rejected commercial fertilizer and knew all about soil composition, grass growing, and body fat in cattle.
Dr. Elkins and his wife, Helen, married in 1966.
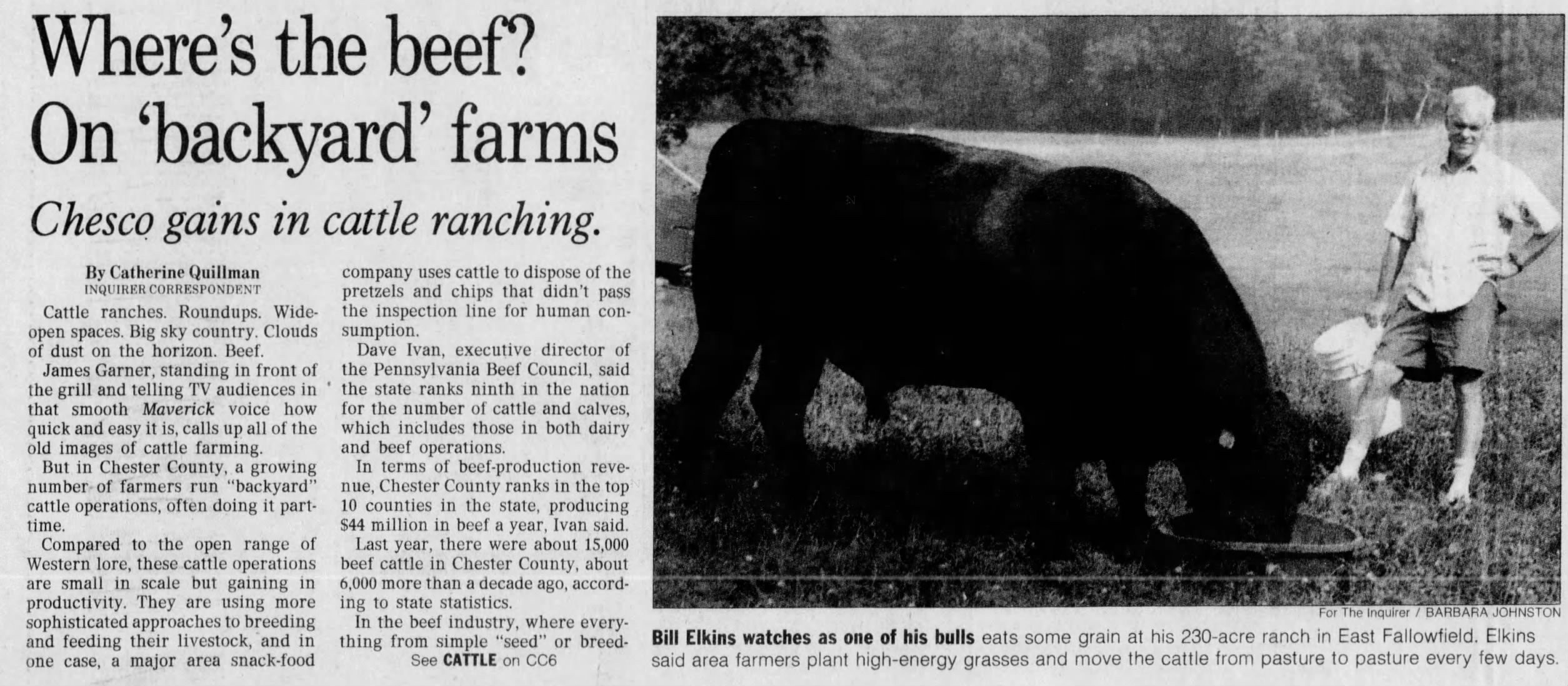
In a 1995 Inquirer story, he said: “Cattle are just like anyone else. If you just turn a few cattle out in a great big field, they will wander around, eat the grass they like best, and leave what they don’t want. That means the less desirable grasses tend to predominate.”
He traveled the country to confer with other cattlemen and helped found the Southeast Regional Cattlemen’s Association in 1994. He sold his beefsteaks, patties, jerky sticks, and kielbasa grillers to private customers online and to butchers and restaurants.
At least one local chef featured an item on the menu called Dr. Elkins’ Angusburger. Lots of folks called him Doc.
He earned his medical degree at Harvard University in 1958 and served two years in the Navy at the hospital in Bethesda, Md. He was a surgical intern in New York and discovered that he preferred the research lab. Before Penn, he worked at the Wistar Institute of biomedical research.
Dr. Elkins graduated from St. Mark’s School in Massachusetts in 1950.
Away from the lab, Dr. Elkins was an ocean sailor, expert navigator, and former boat club commodore. He was active with the Brandywine Conservancy, Natural Lands, and other groups, and was lauded by national organizations for his wide-ranging conservation and wildlife efforts.
He made his farm a haven again for the bobolink grassland songbird and other migratory birds and butterflies that had dwindled. “Buck Run Farm is more about growing grass and trees than beef,” he told Greet Brandywine Valley. “We’re blessed by the land.”
William Lukens Elkins was born Aug. 2, 1932, in Boston. He lived on the family dairy farm in Pocopson, Chester County, when he was young, went to boarding school in Massachusetts for four years, and earned a bachelor’s degree in biology at Princeton University.
He met Helen MacLeod at a party in Washington, and they married in 1966 and had a daughter, Sheila, and a son, Jake. They lived in Center City, Society Hill, and Villanova before moving to the farm. “He was easy to be with,” his wife said.
Dr. Elkins enjoyed sailing and fishing.
Dr. Elkins loved nature, fishing, and baseball, and he followed the Phillies, the Flyers, and other sports teams. “He had a wonderful bedside manner,” his daughter said. “He was a great listener. He really knew how to support people.”
His son said: “He was unassuming and direct. He spoke his mind. He connected with so many different people. He was curious about the world around him.”
His wife said: “He was thoughtful and always concerned about people. He had good humor. He was fun.”
In addition to his wife and children, Dr. Elkins is survived by five grandchildren and other relatives. A sister died earlier.
This article about Dr. Elkins and his ranch appeared in The Inquirer in 1995.
Tower Health’s preliminary financial report in August for fiscal 2025 showed a $5.9 million operating profit, a gain that came thanks for the sale of a shuttered hospital in Chester County.
But that apparent annual profit, the Berks County nonprofit’s first since 2017, turned into a $20.6 million loss when Tower released its annual audit.
Auditors from KPMG decided that Tower should boost medical malpractice reserves and give up on collecting millions owed by patients, Tower said in a statement.
“As part of our standard accounting process, the audited financials for the full year reflect increased malpractice insurance reserves and final adjustments to accounts receivable,” Tower said.
Most of the $26 million swing to a loss came from medical malpractice, but Tower also reduced what is called patient accounts receivable, representing unpaid bills, to $236.6 million from $251.6 million in August’s preliminary results, according to Tower’s audited financial statements that were published Friday.
Separately, Tower reported a $15.9 million operating loss for the three months that ended Sept. 30. That loss was a bit bigger than the $14.2 million loss in the same period last year. Tower’s revenue for the quarter was $501 million, up 4% from $479.8 million last year.
The results for the first quarter of 2026 did not include expenses for Tower’s layoff of 350 employees, or about 3% of its workforce, earlier this month. The cuts hit Pottstown Hospital particularly hard. Tower is eliminating 131 jobs there and eliminating some services.
The closures include the combined intensive care/critical care unit, the Pottstown location of the McGlinn Cancer Institute, and the hospital’s endoscopy center.
Two unions that represent Pottstown employees, the Pennsylvania Association of Staff Nurses and Allied Professionals and SEIU Healthcare Pennsylvania have decried the cuts and called on management to engage in discussions on how to preserve jobs and services.