Main Line Health appointed Anna Michelle Brandt president of its Lankenau Medical Center in Wynnewood, the nonprofit health system announced Monday.
Brandt mostly recently worked as chief operating officer at University Hospital, a 519-bed academic medical center in Newark, N.J., which Main Line’s new CEO Ed Jimenez led before taking over at Main Line.
The new Lankenau president also worked previously with Jimenez at UF Health Shands Hospital in Florida.
Brandt succeeds Katie Galbraith, who left Lankenau in September after about three years to lead New England Baptist Hospital in Boston.
Lankenau, a level 2 trauma center, sits in Lower Merion Township at the intersection of West Philadelphia and Montgomery and Delaware Counties.
“Why would you not want to study the thing that lets you study,” said Schechtman-Taylor, a senior from New York City. “The brain, that’s our entire world.”
Neuroscience has become the most popular major on the highly selective liberal arts campus on Philadelphia’s Main Line, counting nearby Bryn Mawr College students who also take classes at Haverford. And it’s only been around since 2021 when the two colleges — which have had a minor in the discipline since 2013 — decided to administer the joint major.
At Haverford, there were 24 majors the year it started; now there are 60. Bryn Mawr saw similar growth and currently has 49. Enrollment in Haverford’s neuroscience classes including both Bryn Mawr and Haverford students grew from 154 in 2014 to nearly 800 last fall.
“We knew that neuroscience was going to be popular, but we did not anticipate this growth,” said Helen White, Haverford’s provost, who noted the school recently hired another neuroscience professor to accommodate more students.
The major’s popularity is also growing at schools around the Philadelphia region — and across the country. Students and professors say neuroscience is popular because it’s interdisciplinary, involving psychology, biology, and chemistry, and can lead to a variety of careers. It can also be personal, because it involves studying diseases like Alzheimer’s and Parkinson’s, which have no cures, and the treatment of strokes and traumatic brain injuries.
“I would say about 90% of my students are coming into my lab because they have someone in their family with one of these diseases,” said Rob Fairman, a Haverford biology professor whose research focuses on neuroscience.
Haverford senior Alina Schechtman-Taylor, 21, of New York City, works as a teacher assistant in professor Laura Been’s lab.
A growing major
In 2008, 110 colleges nationally offered neuroscience majors; now, it’s about 330, said Raddy Ramos, associate professor in the Department of Biomedical Sciences at the New York Institute of Technology. Ramos, who coauthored studies on the topic, said there were more than 2,000 neuroscience graduates in 2008; in 2019, that number had grown to more than 7,200.
window.addEventListener(“message”,function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r,i=0;r=e[i];i++)if(r.contentWindow===a.source){var d=a.data[“datawrapper-height”][t]+”px”;r.style.height=d}}});
Pennsylvania is a hot spot, with 36 colleges having programs in 2022-23, Ramos said — more than than any other state.
Drexel University, which has had a minor since 2015, launched its undergraduate major in neuroscience in 2024.
“We have seen a 45% increase in applications over the last two years,” a university spokesperson said.
Pennsylvania State University in November announced it was launching two new undergraduate majors in neuroscience, one offered by the biology department and the other by the biobehavioral health department.
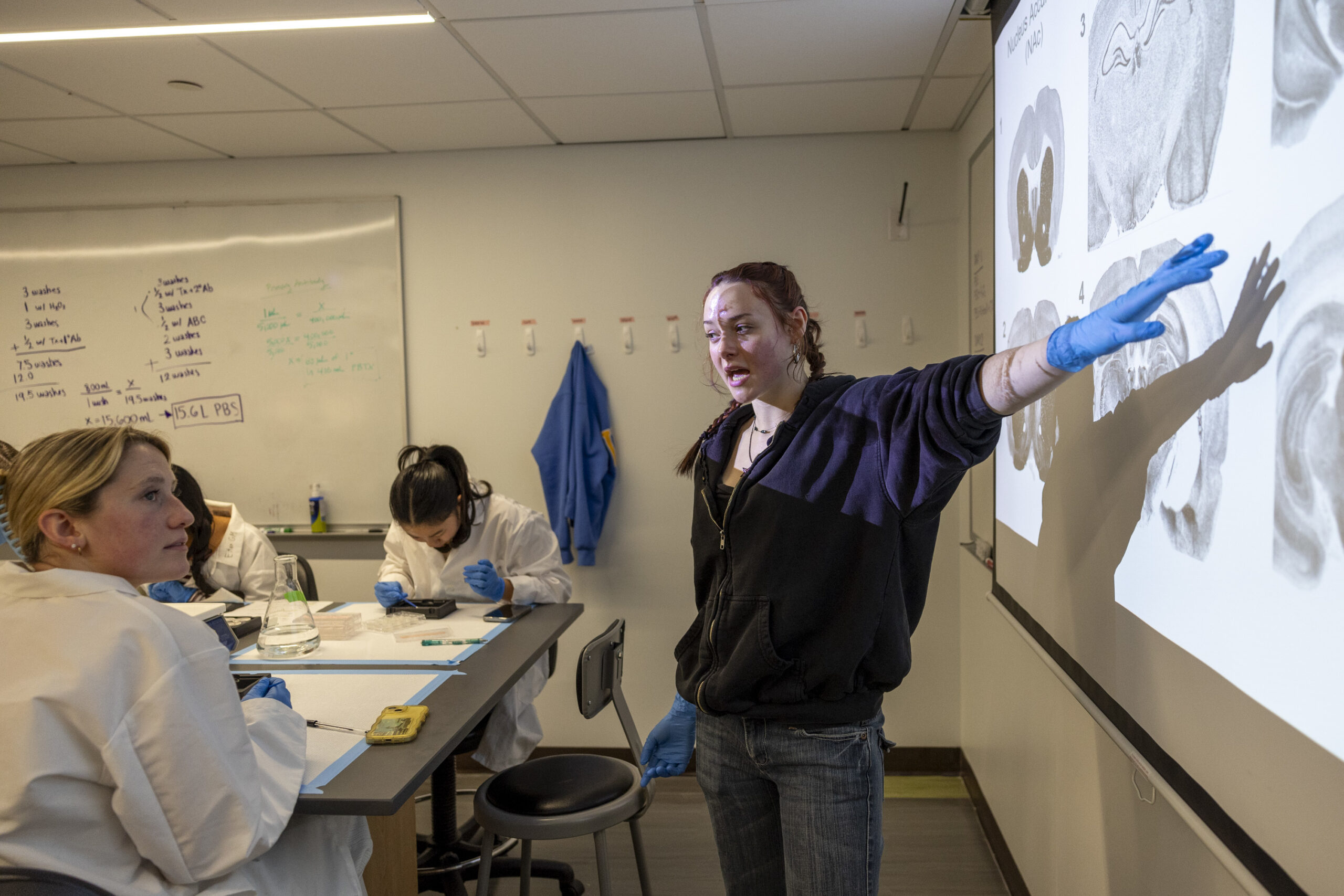
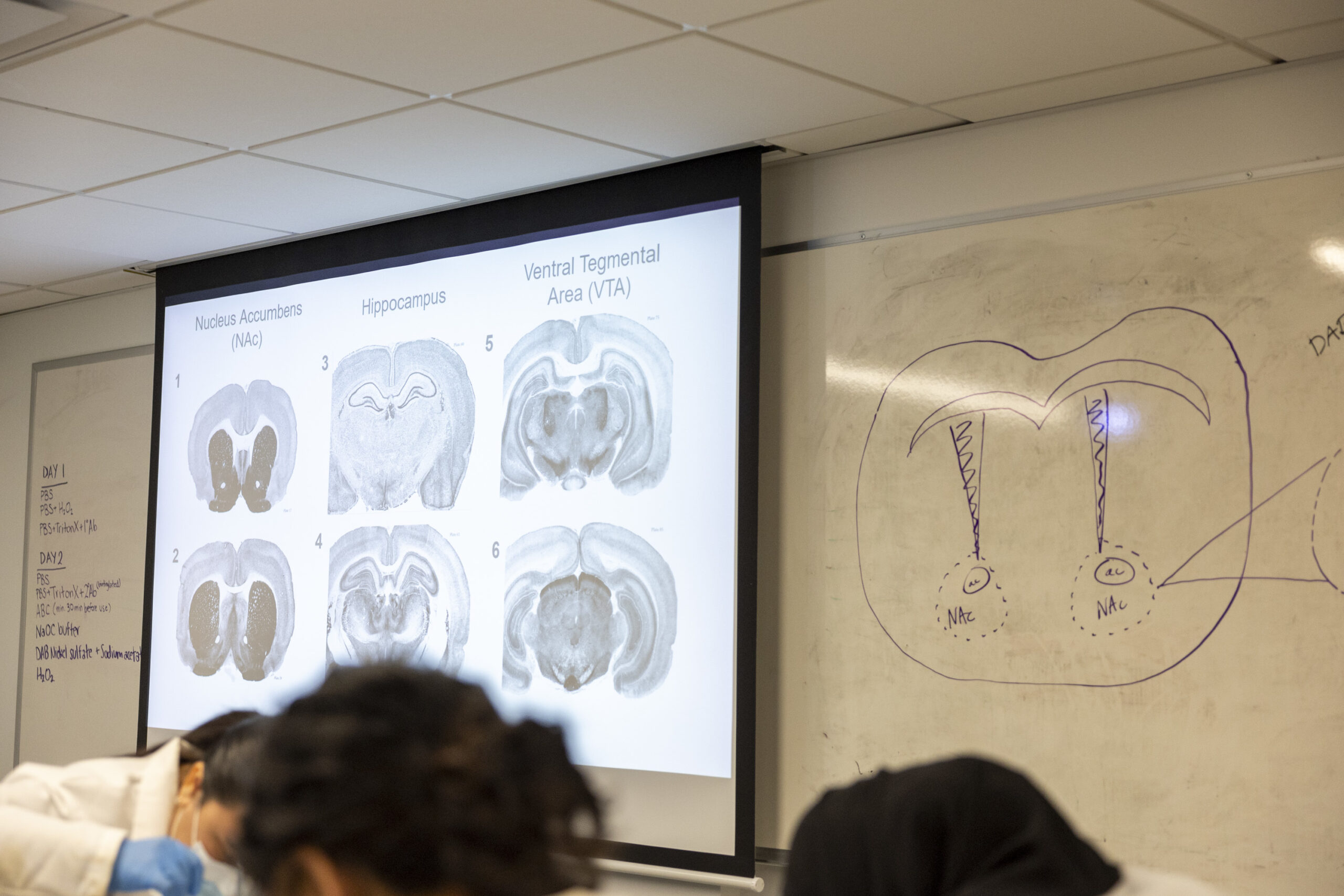
Students look for sections of rat brains that match the sections projected on the screen in a Haverford College lab.
Neuroscience has become especially popular among pre-med majors, school officials say. Otherpotential career paths include biotechnology, pharmacology, psychology, and neuroengineering, while somestudents go on to law school, business, or public policy.
“There’s a lot more awareness that mental health conditions are due to changes in the brain, and people want to understand that,” said Lisa Briand, associate professor and program director for Temple University’s neuroscience program.
At Temple, neuroscience has become the fourth largest of 30 majors in liberal arts, Briand said. The psychology department a few years ago changed its name to psychology and neuroscience, she said.
At the University of Pennsylvania a decade ago, 100 to 120 neuroscience majors graduated annually, said Lori Flanagan-Cato, associate professor of psychology and codirector of the undergraduate neuroscience program.
“Twice in the past 3 years we have had over 150,” she said.
Swarthmore College, a highly selective small liberal arts college, graduated 10 to 12 neuroscience majors a year about a decade ago, said Frank Durgin, professor of psychology who oversees the program.
“This year, we anticipate graduating 24 majors,” he said. “Next year, it’s 30.”
The college has added two professors in the last two years to accommodate growth, he said.
Why students study neuroscience
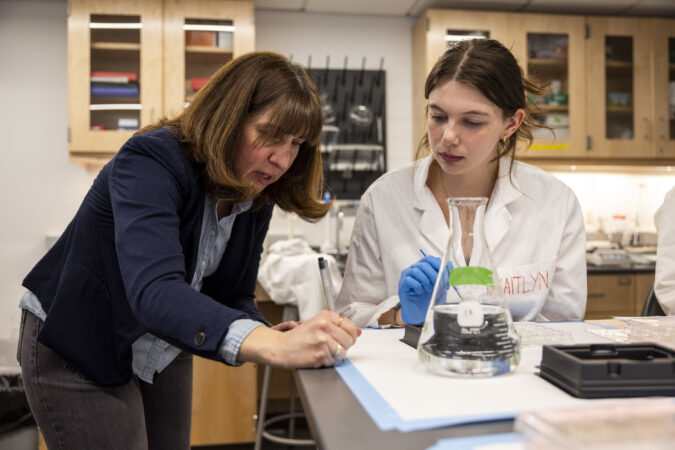
In a lab at Haverford one afternoon last month, 16 students in white lab coats poked with paintbrush tips at thin slices of rat brain in preservative fluid, preparing to stain them to look for which neurons were activated. Some of the rats received the drug Ritalin, commonly used for attention deficit disorder, while others did not. Students were trying to discern differences in their brains when they performed certain tasks, said Laura Been, associate professor of psychology and director of the bi-college neuroscience program.
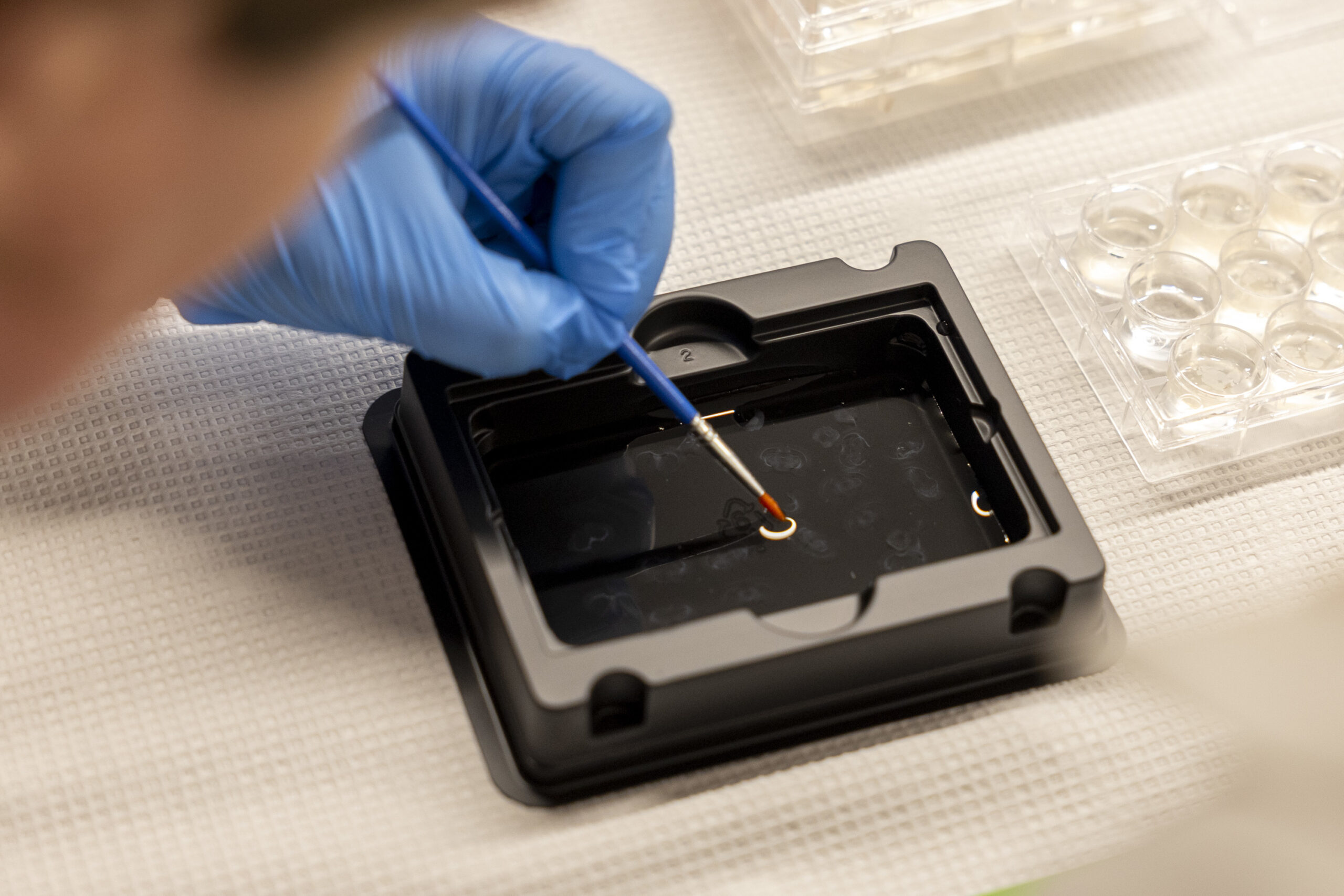
A neuroscience student works with sections of rats’ brains in a lab at Haverford College.
“We can … try to learn something more about how this sort of drug treatment impacts the brain,” said Been, whose area of interest is behavioral neuroendocrinology, which looks at the relationship between hormones, the brain, and behavior.
Students in Been’s class had varied reasons for studying neuroscience.
Emily Black, visiting assistant professor of neuroscience at Haverford College, helps Savannah Shaw, 22, of Downingtown, during neuroscience lab work. “I really like the variety of the classes we can take in the major,” said Shaw, a senior who plans to go to medical school, possibly to become a neurologist. “You can go more the psychology route or go more biology.”
Sophia Lipari, 21, a junior from Jacksonville, Fla., whose father is a reproductive endocrinologist, is interested in hormones and the field of fertility.
Riley Fass, 20, a junior from Claremont, Calif., wants to be a special-education teacher. She already sees the connection between neuroscience and her job as a teacher’s assistant at a school where children have traumatic brain injuries and cerebral palsy.
“The topics we discuss — an injury here will result in this — I can actually see it in my students,” she said.
Iris Goxhaj (left), 21, of Northeast Philadelphia, and Riley Fass, 20, of Claremont, Calif., work with sections of rats’ brains in a lab at Haverford College.
Deeya Abrol’s interest was stoked when she worked with a child on the autism spectrum as a swim instructor. Abrol, 22, a senior from Los Gatos, Calif., plans to go to medical school.
Schechtman-Taylor meanwhile wants to pursue biomedical engineering and specifically developing medicines for the treatment of neurodegenerative disorders.
“I want to work on the treatment side,” she said.
Fairman, the Haverford biology professor, said a recent graduate’s mother had died of Huntington’s disease, meaning she has a 50% chance of getting it, he said. She worked in his lab and wanted to be involved in hisresearchon protein clumping in the brain and its effect on diseases such as Parkinson’s and Alzheimer’s.
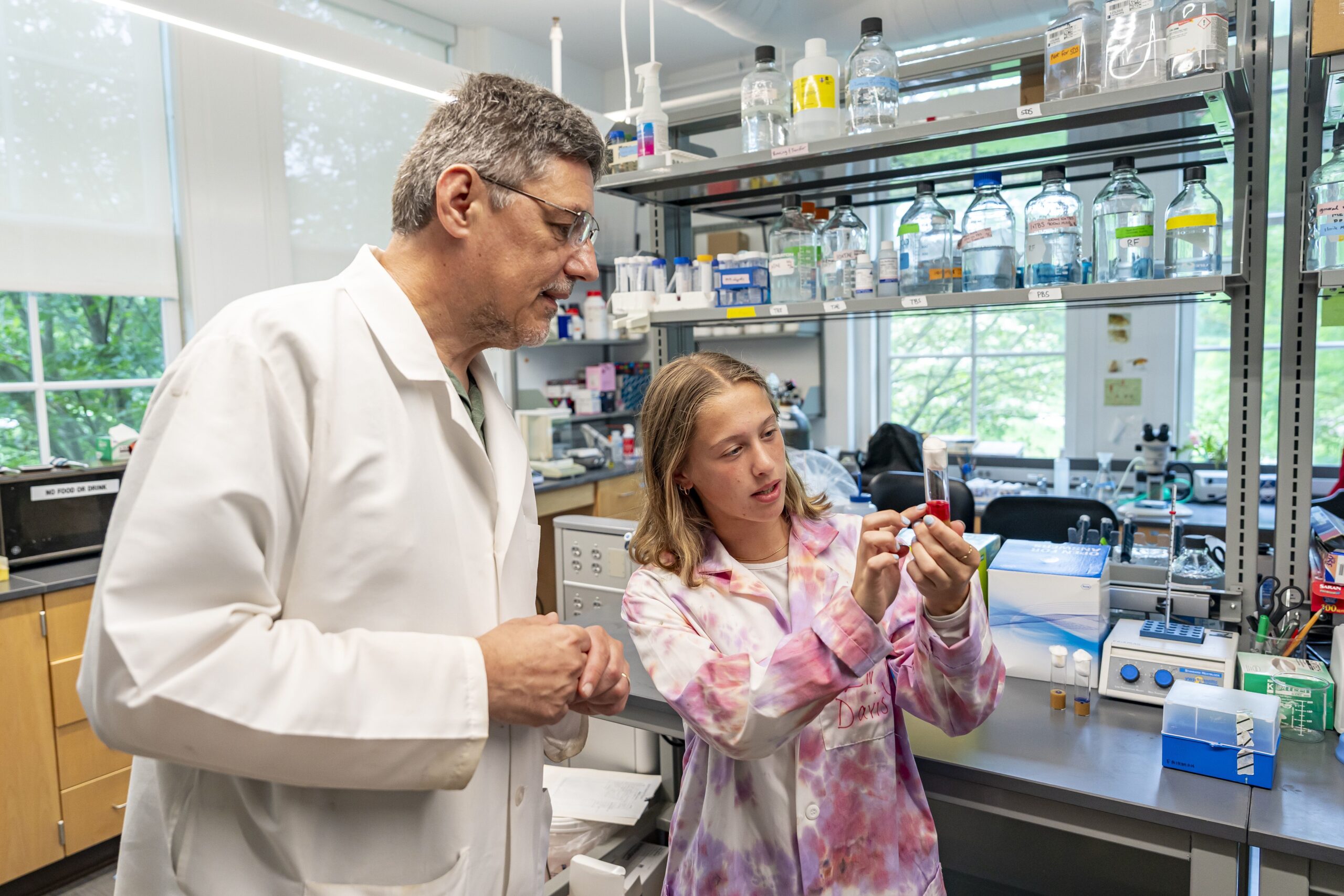
Rob Fairman, a professor of biology at Haverford College, and student Liv Davis are testing the effects of natural products on animal models with neurodegenerative diseases.
Junior Liv Davis, 21, wanted to help find a cure for Parkinson’s, which struck her grandmother in 2020.
“She’s had two falls in the last year and a half because it’s progressed pretty quickly,” said Davis, of Lanoka Harbor, N.J. “It’s hard to see someone you love so much live with it, but it makes it all the more rewarding to work toward fixing it.”
Davis, who has worked in Fairman’s lab since her freshman year, tried to get into an introduction to neuroscience class early on. But there wasn’t room. She ended up majoring in biology, which she thinks probably would have happened anyway.
About half the students working in Fairman’s lab are neuroscience majors, he said.
Davis is currently studying the effect of a chemical on sleeping fruit flies that have been genetically modified to carry the protein associated with Parkinson’s.
Last summer, she received an inaugural research fellowship funded by Shamir Khan, a Haverford alumnus and psychologist who was diagnosed with early-onset Parkinson’s.
Her grandmother was glad she could continue the research, said Davis, who plans to become a doctor.
“She always jokes with me,” Davis said. “‘Give me a spoonful of that chemical, whatever it is. If you need a test subject, you let me know.’”
At AMS Surgery Center in suburban Montgomery County, patients can park right in front of the entrance, walk through just a few doors, and undergo cardiac procedures in a sterile operating room with equipment as high-tech as in any hospital procedure room.
In the year and a half since its first patient underwent a cardiac catheterization, the center has performed more than 1,000 cardiac procedures that previously required patients to go to full-service hospitals.
The Horsham center showcases a new front as sophisticated healthcare procedures move to freestanding outpatient medical facilities, promising to save patients money. The shift also adds to the financial pressures facing the region’s hospital-centered health systems.
Four centers have opened or are in the final stages of approvals in Southeastern Pennsylvania. Their arrival comes after state lawmakers in 2022 broadly expandedthe types of procedures allowed outside hospitals to include cardiac catheterizations, pacemaker implants, and other treatments that until then had to be done in a hospital.
Pennsylvania is the first Northeastern state to allow the minimally invasive procedures in freestanding surgery centers, but Southern states like Florida, Louisiana, and Texas have permitted the practice for decades, experts said. Research has found surgery centers generally are as safe as outpatient departments in hospitals.
An independent physicians group, Bryn Mawr Medical Specialists Association, opened Heart & Vascular Center of the Main Line — the Philadelphia region’s first such center — in late 2022. in Bryn Mawr. AMS Surgery Center in Horsham performed its first procedure in the fall of 2024, initially treating only Medicare patients. Itadded patients with private insurance last summer.
The market has continued torapidly expand:ReVaMP Heart & Vascular Surgery Center in Center City started treating Medicare patients last fall. The Ambulatory Cardiovascular Center of Pennsylvania, near King of Prussia, expects to perform its first procedures on patients next month.
Medicare pays the centers about a third less than hospital outpatient departments for the same procedures, but the centers have significantly lower costs, allowing them to be profitable. Medicare pays physicians the same wherever procedures are done.
Independent cardiology groups traditionally have performed interventional procedures, such as implanting stents and pacemakers, in hospitals. Some are jumping at the opportunity to expand through the surgery centers, where they can have a financial stake in the entire operation.
“We’ve always been very fiercely independent, fiercely entrepreneurial, and patient-centered,” said Richard Borge, an AMS interventional cardiologist who is medical director for the group’s surgery center.
How much cardiac care — among the most profitable business lines for hospitals — will move out of hospital outpatient departments remains unknown. But cardiac surgical clinics will not take over heart care to the extent seen when outpatient orthopedic centers began offering hip and joint replacements,predicted Lauren Clementi, a senior vice president at Kaufman Hall, a Chicago consulting firm.
“This one’s a little trickier because the acuity of patients,” she said.
Cardiologists will continue treating many patients with complex medical needs in hospitals, which remain the only option for riskier procedures such as open-heart surgeries.
Gregory Schmitt went to AMS Surgery Center to undergo procedures for a heart stent and stents in both legs.The retired machine-shop owner, who lives in Ivyland, called such centers great for patients.
“I highly recommend it. It’s much easier than trying to navigate a hospital,” Schmitt said.
How we got here
Healthcare has been shifting awayfrom requiring overnight hospital stays, even for common procedures like cataract surgery.The trend starteddecades ago with same-day procedures in hospitals, followed by the rise of freestanding surgery centers.
In cardiology, people now commonly receivestents and pacemakers as outpatient care. But until recently, doctors had to implant the devices in a hospital.
“Once upon a time, every patient we cathed had to spend the night in the hospital,” said veteran cardiologist Mark Victor, referring to cardiac catheterization.
With the rise of outpatient procedures,Victor said, the question for many clinicians became: “If they’re hospital ambulatory, why do they have to be in the hospital at all?”
Victor has long advocated for the adoption of outpatient cardiology proceduresas the CEO of Cardiology Consultants of Philadelphia. Thelarge cardiology practice joined last year a national private-equity backed group, Cardiovascular Logistics, and will soon start performing surgical procedures at the center opening near King of Prussia.
In 2020, Medicare started paying for outpatient cardiac catheterizations — which entail running a catheter through a blood vessel in the thigh or wrist to examine the heart and install devices like stents.
Richard Borge is medical director of AMS Cardiology Surgery Center in Horsham, whose arrival is moving advanced cardiac care from hospitals to outpatient clinics.
Even then, Pennsylvania rules required cardiac catheterizations to occur in an acute-care hospital, according to Stephen Abresch, director of government affairs for the Ambulatory Surgery Center Association, a national trade group in Alexandria, Va.
Pennsylvania lawmakers cleared the way for expansion byeliminating that restriction in 2022 as part of a broad expansion of what the state’s surgery centers were allowed to do. “It had been a quarter century since the state had gone in and reviewed that,” he said.
The Heart & Vascular Center of the Main Line has scheduled its first cardiac ablations this week. Horsham’s AMSaims to start offering those procedures in June. Victor’s King of Prussia groupexpects to add ablations in the future as well.
Impact on hospitals
It is too soon to know how the new surgery centers will impact the region’s existing health systems. In some cases, independent cardiologists generate significant patient numbers forhospitals’ cath labs.
After Bryn Mawr Medical Specialists opened its cardiovascular surgery center near Main Line Health’s Bryn Mawr Hospital, the private group performed fewer procedures on low-risk patients at the hospital.
To sustain patient volumes, Main Line has increased collaboration with other physician practices, while continuing to treat an“older patient population, whose more complex health conditions require the advanced expertise and emergency support only a hospital setting can provide,” officials said in a statement.
In Horsham, most of the patients coming to AMS would have gone toJefferson Abington Hospital before the surgery center opened in partnership with Atria Health, a private-equity backed group, Borge said.
Jefferson declined to comment.
King of Prussia’s Ambulatory Cardiovascular Center of Pennsylvania is opening through anunusual four-way partnership involving Cardiology Consultants of Philadelphia, Cardiovascular Logistics, SCA (a unit of UnitedHealth’s Optum), and the University of Pennsylvania Health System.
“Ours is not going to seriously impact any one hospital system, which they’re all relieved about,” said Victor, who is also president of the Mid-Atlantic region for Cardiovascular Logistics. He said other health systems were invited to invest in the surgery center, but only Penn did so.
Penn declined to comment for this article. On the Alvarez & Marsal What’s Your Moonshot podcast, the health system’s chief operating officer, Michele Volpe, recently said the system needs ”to move a bit faster in taking much of the work that we are doing in inpatient ORs and moving them into outpatient or ambulatory freestanding ORs.”
AMS Cardiology’s ambulatory surgery center in Horsham is one of four new cardiovascular surgery centers in Southeastern Pennsylvania.
Center City’s ReVaMP Health & Vascular Surgery Center wantsto bring in cardiologists from nonaffiliated practices,and even the city’s big health systems. The facility opened last year, spearheaded by Re-Vasc Med Professionals’ two interventional cardiologists in partnership with Surgery Partners, a publicly traded manager of surgery centers nationwide.
“I’m 100% sure this is going to be the trend of the future,” Re-Vasc CEO and founder Jon George said.
A health insurer’s perspective
Richard Snyder, a top executive at Independence Blue Cross, the largest health insurer in Southeastern Pennsylvania, has for years watched joint replacements and other procedures shift from hospitals to lower-cost surgery centers.
The financial impact goes beyond the lower prices at surgery centers, he said, expecting that hospitals will not simply cede these patients to new competitors.
Some hospitals might decide to take a lower payment for outpatient procedures. “Traditionally, that happens when we have capacity in lower-cost settings,” he said.
At the same time, Medicare is pushing to pay the same price for services, wherever they are performed. “Hospitals, by necessity, will need to move some things to lower-cost settings in order to not lose money on them,” Snyder said.
University of Pennsylvania health expert Ezekiel Emanuel’s casual conversations often evolve into impromptu medical consultations.
People askEmanuel — an oncologist, bioethicist, and health policy scholar who helped write the Affordable Care Act — how to live healthier.
He said that “incessant asking” inspired him at a time when both information and misinformation are booming in the wellness space.
His new book, “Eat Your Ice Cream: Six Simple Rules for a Long and Healthy Life,” landed on bookshelves in January. He uses the pages toargue that the goal of life should not be to simply live the longest, but rather to lead a healthy and fulfilling life.
The Penn professor, who has antique maps in his office and has taught a course on Ben Franklin, weaves inhis appreciation for history throughout the book. Emanuel’s advicealso addresses contemporary issues such as vaccines and vaping. And hesharespersonal family stories involvinghis father (to whom the book is dedicated).
In one of his favorite anecdotes, he describes looking for a cheap car to buy with his bar mitzvah money. Thinking he found a great deal on a Volvo, Emanuel and his brother bought the car, brought it home, and realized it couldn’t go in reverse.
“My father says, ‘You guys are schmucks!’” he recalled.
That became the first of his six rules: “Don’t be a schmuck — avoid self-destructive risks.”
The Inquirer spoke with Emanuel about tips for livinga healthy life in a conversation lightly edited for length and clarity.
Why do you think wellness has become so big?
People feel like the world’s topsy-turvy. They’re not controlling it. It is controlling them. They want to assert control over the world, and one way they can do it is through wellness.
What have people gotten wrong about wellness?
Spending 10 hours a week on wellness, like some people recommend, is crazy. Just insane. You should not do that. You can spend two or three hours a week, get all the benefit you need, and focus your time on other things — your family, close friends, having a successful career, making the world better, making Philadelphia better. Those are the things that matter.
What does your first rule (Don’t be a schmuck) mean?
The first rule is, really, take reasonable risks, but not unreasonable risks.
The most dangerous thing most of us do in everyday life is turn the ignition on in our car. Driving is actually quite dangerous over a lifetime. And you have to compare the risk you’re willing to take to the risk of driving. I try to organize a chapter laying out unreasonable risks like BASE jumping [an extreme sport in which a person parachutes from a dangerous height]. Why is that so stupid? Well, look at the data. I try to make that assessment much more quantitative.
What is your second rule?
The importance of social relations.
It doesn’t get emphasized by almost anyone in the [wellness] field, and it’s vastly the most important for longevity, for health, and for happiness. We’ve got tons of data. There’s more than 3 million people who’ve been studied on the relationship between loneliness, social isolation, and ill health.
If you look at the Harvard Study of Adult Development, which started in the late 1930s, the single most important predictor of a long, healthy life with the fewest comorbidities is the number and quality of your social relationships.
Overall, a professor at Brigham Young University has summarized that being socially isolated is ‘like smoking 15 cigarettes a day.’
Tell us about your last four rules.
The third one is stay mentally sharp. If the body’s working fine, but cognitive decline has set in, that would be hell to me. I don’t want to live like that.
There are only a few people like Ben Franklin where it does not appear to decline at all. One of the things actually I learned after I finished the book is Franklin was the oldest person (aged 81) at the Constitutional Convention in 1787. He was still very nimble with his mind, able to put things together, to craft compromises and things.
Some of it’s obviously genes, but some of it’s also things you can do — what you can eat, how you exercise, your retirement, your strategies, social interaction, challenges, etc. The brain is a lot like muscle in that either you use it or you lose it.
The last three rules are the typical: eating well, exercising, and sleeping advice.
Are there things that you’d want the media to emphasize more when talking about wellness and health?
There are two really fundamental things on the ‘to do’ side for eating.
One is you should eat more fermented foods. Whether it’s yogurt or cottage cheese or aged cheeses or kimchi. It’s very important for the microbiome. In Philadelphia, one of our treasures is Di Bruno Bros.cheese shop. They have 200 cheeses on display. Go and get some cheese. It’s really good.
The other is that more than 90% of Americans don’t get enough fiber in their diet every day. You need to eat more fruits and vegetables. I start out every day by merging these two. This morning, I had a bowl of berries, or some kind of fruit, with yogurt, granola, and oats. I also added hemp hearts, which are high in protein, good fats, omega-3s and omega-6s. Then add a salad at dinner, and you pretty much have enough fruits and vegetables.
Can you explain the title of your book, “Eat Your Ice Cream“?
Ice cream is good. Dairy products are associated with higher height, especially if, early in life, you eat a lot of dairy. Second, [dairy consumption] is also associated with a lower risk of colorectal cancer, which is all in the news these days.
And most importantly, it’s about joy. It’s fun. Who doesn’t like ice cream? But it’s important to get good ice cream, not stuff with emulsifiers and fillers and all of that.
Have a little joy. It goes a long way toward making life lovely.
Q: I exercise most days, but the number on the scale never moves. What’s even the point?
A: Exercise is not very effective for weight loss, but it’s incredibly beneficial for your physical and mental health.
As a sports medicine physician, I spend my days treating injuries, studying human performance, and helping my patients move. I prescribe exercise for health and believe deeply in its power. The evidence is overwhelming: Exercise lowers cardiovascular risk, improves blood sugar control, strengthens bones, preserves cognitive function, and reduces the risk of depression, cancer, and early death.
But there is one area where exercise consistently falls short: weight loss.
A patient in her 50s recently came to me frustrated. She walked most days, strength trained twice a week, and followed a careful diet. Yet her weight barely budged. She asked me a question that I often hear: “What is the point of exercise if the scale doesn’t move?”
The irony was that almost everything important about her health was improving. The problem was that she had been conditioned to focus on the wrong number.
Why exercise doesn’t work for weight loss
In a culture that treats the gym as a calorie-burning machine, many people expect exercise to shrink their waistline. When it doesn’t, frustration follows. The truth is that our expectations are misguided. Large studies show that exercise alone usually produces modest weight loss, often just a few pounds over six months. That’s because your body will “correct” for the extra activity by increasing your appetite or by lowering the calories burned for other bodily functions.
In a 2024 randomized trial involving middle-aged adults who were overweight, participants assigned to regular exercise without changing their diet improved fitness and metabolic markers but lost little weight.
As we age, the challenge grows. Resting metabolism slows and the body becomes more efficient at conserving energy. Various factors influence this, including age-related sarcopenia, or muscle loss with aging. We have to exercise for longer or more intensely — to the point it may become unrealistic — to achieve a calorie deficit substantial enough for weight loss.
That does not mean exercise fails. It succeeds brilliantly. We have simply been asking it to do the wrong job.
Proven health benefits of exercise
Exercise shines when it comes to metabolic health. It improves insulin sensitivity and reduces visceral fat, the type of body fat that lies deep in the abdomen and is linked to heart disease and Type 2 diabetes. These benefits often occur even when body weight stays the same. Recent research shows that short bursts of movement built into daily life, “exercise snacks,” lead to significant reductions in disease risk, even in small doses.
Exercise makes people healthier even when it does not make them thinner. In fact, people who are fit tend to live longer than those who are not in shape, no matter what their body weights are.
This distinction is important in the age of GLP-1 medications and other weight loss drugs. For many, these treatments make losing weight easier than ever. They have changed the weight-loss equation for thousands of my patients. But weight loss alone is not health.
Rapid, medication-driven weight loss can carry hidden costs, including loss of muscle. Muscle is central to mobility, glucose control, and healthy longevity. Losing muscle while getting lighter may improve the scale but leaves people less resilient.
That is why my advice often surprises patients. I would rather see someone mildly overweight and physically active than thin and inactive. The former usually has better fitness, stronger bones, more muscle, and greater protection against disease. The latter may look healthy but often carries hidden risks.
If the goal is long-term health, prioritize movement and muscle, not weight alone. Walk more. Lift weights. Climb stairs. Carry groceries. Build strength into daily life. Use exercise as a tool for healthy longevity, not as a stand-alone vehicle for weight loss.
For decades, we have equated thinness with health. It is time to change that. Consistent movement may or may not change your weight, but it always improves health. That is the outcome that truly matters.
Jordan D. Metzl, MD, is a sports medicine physician at Hospital for Special Surgery in New York. His newest book, “PUSH: Unlock the Science of Fitness Motivation to Embrace Health and Longevity,” explores the topics of fitness motivation and muscle maintenance for healthy longevity.
Jefferson Abington Hospital was cited by the Pennsylvania Department of Health for sanitation problems in its trauma center last year.
The incident was among more than a dozen visits health department inspectors made to the Jefferson Health facility between December 2024 and November 2025.
Here’s a look at the publicly available details:
Dec. 4, 2024: Inspectors followed up on a July 2024 citation for failing to report an incident in which a mental health patient ran away from the hospital and security staff left the hospital’s campus to apprehend them.
Dec. 23: The Joint Commission, a nonprofit hospital accreditation agency, renewed the hospital’s accreditation, effective September 2024, for 36 months.
Jan. 16, 2025: The hospital was cited for sanitation issues, including several dirty triage bays, a brown substance under a patient’s head and on the floor, and a black, sticky substance on a hospital bed wheel. Administrators retrained maintenance workers on cleaning protocol and assigned additional staffers to ensure daily cleaning.
Jan. 16: Inspectors came to investigate a complaint and for a monitoring survey but found the hospital was in compliance. Complaint details are not made public when inspectors determine it was unfounded.
Jan. 28: Inspectors visited for a mental health monitoring survey and found the hospital was in compliance.
Feb. 19: Inspectors came to investigate a complaint but found the hospital was in compliance.
March 12: Inspectors came to investigate a complaint but found the hospital was in compliance.
April 17: Inspectors followed up on the January citation regarding sanitation issues and found the hospital in compliance.
May 29: Inspectors came to investigate two complaints but found the hospital was in compliance.
July 16: Inspectors came to investigate a complaint but found the hospital was in compliance.
Sept. 5: Inspectors came to investigate a complaint but found the hospital was in compliance.
Sept. 18: Inspectors came to investigate a complaint but found the hospital was in compliance.
Nov. 5: Inspectors came to investigate a complaint but found the hospital was in compliance.
Jeff Galloway, an Olympic distance runner who inspired hundreds of thousands of Americans to exercise by extolling the virtues of taking walking breaks during races — or “Jeffing,” as adherents called his signature method — died Feb. 25 in Pensacola, Fla. He was 80.
Mr. Galloway died in a hospital after suffering a stroke, his son Westin Galloway told the Washington Post.
Mr. Galloway described himself as an average runner as a teen who enrolled in his first marathon in Atlanta “because of the size of the trophy” and, by persistence more than talent, ascended to the U.S. Olympic team. For the 1972 Olympics in Munich, he qualified for the 10,000-meter race and was an alternate for the marathon. The next year, he set a U.S. record in the 10-mile road race.
Despite reaching the peaks of his grueling discipline, Mr. Galloway became most widely known for a training program with an everyman philosophy that spoke to reluctant runners and preached, of all things, walking.
Mr. Galloway began pioneering what he called a “Run Walk Run” technique — taking breaks to walk during training runs and even races — in the 1970s as he taught running to beginners. He championed the method as a way to reduce injury, control fatigue and, most importantly, motivate newcomers to “get off of the couch and run.”
Legions of new runners did just that. Mr. Galloway’s philosophy, espoused in books and an online training program, has reached more than a million people, his organization has said, and changed how athletes approach distance running.
Mr. Galloway had “the ability to empower runners, or people that didn’t even see themselves as runners,” his son Westin said, “giving them the space to be the athlete or the person that they never thought they could be through the benefits of exercise.”
John Franks Galloway was born in Raleigh, N.C., on July 12, 1945. His father was an educator and a sailor in the Navy; his mother worked at a private school in Atlanta that his father founded.
Mr. Galloway, who grew up in Atlanta, was not initially a prodigious running talent. He enrolled in a track conditioning program in eighth grade because his school required sports participation each quarter and the track coach was rumored to be the most lenient of the sports instructors, he wrote on his website.
“I can identify with the struggles of sedentary, overweight adults and kids, for I was one,” Mr. Galloway wrote.
Two months of running through forest trails got him hooked. Mr. Galloway qualified for the state high school championships in Georgia his senior year, then attended Wesleyan University, where he studied history and was an all-American runner.
Mr. Galloway served for three years in the Navy after college, a tour that sent him to Vietnam. Upon returning to the United States in 1970, he enrolled in graduate school at Florida State University with the goal of qualifying for the upcoming Olympics.
Even after years of training, it felt like a long shot, Mr. Galloway wrote. On a 90-degree summer day at the 1972 national championship in Seattle, he squeaked onto the 10,000-meter Olympic team in a close race — perhaps because he took it slow.
“Many of the runners had started too fast, and I did not,” Mr. Galloway recalled on his website. “I found myself catching up to the stragglers, passing one, then another.”
As a fitness boom took hold in the U.S. after the Munich Olympics, Mr. Galloway founded a running store, Phidippides, opened vacation fitness camps, and wrote several books about running. “Jeffing,” or “the Galloway method,” became his most famous innovation.
At running clinics across the country, Mr. Galloway promoted his framework. Giving runners permission to take walking breaks while training encouraged beginners, he said, and the staggered runs could help even veteran marathoners improve their times.His charm and relentless focus on reaching novice runners set him apart from other instructors, Westin Galloway said.
“A lot of coaches were very focused on faster times and pushing people’s bodies to do the best that they could,” he said. “And he kind of looked at it from the other perspective of, running has an amazing way of changing a person’s life, and if he could get more people out there doing it, the world would be a better place.”
Mr. Galloway remained a fixture of the running community and continued to run and help organize races as he grew older. At 70, he ran the Marine Corps Marathon in Arlington in honor of a Marine killed in the 2015 Chattanooga, Tenn., shooting at a Navy operations center. He returned to running after suffering a heart attack in 2021 that kept him hospital-bound for almost a month.
In the months before his death, Mr. Galloway had been fixated on run-walking another race at the age of 80. He had planned to run the Honolulu Marathon in December but fell and broke his kneecap. That didn’t discourage him, either, he told the New York Times in December.
“Doing another marathon, to me, feels like the strongest goal I’ve ever had in my life,” Mr. Galloway said to the Times.
Mr. Galloway is survived by his wife, Barb, 72; his sons Westin and Brennan; and six grandchildren. They are all runners, and Westin manages Mr. Galloway’s organization that continues to share his training program with runners around the world.
“Jeffing” has recently seen a renewed surge of interest, Westin Galloway said, as more people have taken up running since the coronavirus pandemic. Asked whether the influx of new adherents made Mr. Galloway proud, Westin demurred.
“He was happy talking to a single individual,” Westin said. “He didn’t care about numbers. He didn’t care about getting on the news or having big stories published about him. He cared about helping one person at a time.”
If you’ve ever watched a race, you may have seen some runners whiz by, others resolutely jog forward — and a sizable group slow down to a walking pace, sometimes just a few minutes after passing the start line.
No, they don’t need your cheers to “just keep going!” Rather, it’s likely those walk breaks are calculated. It’s all part of a time-honored technique known as “Jeffing,” and runners have been using it for decades in training runs and in major races like the New York City Marathon.
While this method is pretty well known among runners, it’s not only for those looking for personal records. Rather, it can be a great way for people to add a little oomph to their walking workouts and gain even more health-promoting benefits. Here’s everything you need to know.
What is ‘Jeffing’?
Simply put, Jeffing is a technique that intersperses walk breaks with running bouts to help ward off fatigue and boost endurance. This type of cardio, or aerobic, workout goes by many different names in the running community — run-walk, run-walk-run, the Galloway method, and, of course, Jeffing.
The last two are nods to Olympian Jeff Galloway, who began using this method in 1973 while instructing a beginner running class at a university. (Galloway himself has no particular preference for which term is used. “I’m honored to be a verb,” he said.)
Galloway ran weekly with the 22 students in the program, who naturally divided into three pace groups based on their abilities. “Whenever anybody started huffing and puffing in any group, I would have everybody walk.” Galloway said.
All of the participants stuck with the program for the entire 10 weeks, and all were able to complete their final goal: finishing either a 5K or 10K race. The walk breaks, Galloway believed, played a vital role in that.
In this earliest iteration of Jeffing, there was no set timing on when to start walking and for how long to do so. But after further refining, it soon became clear to Galloway that the important part is to slot in walking breaks before you feel gassed.
“Because you’re taking those walk breaks from the beginning, before you’re tired, before you need them, it feels great,” said Chris Twiggs, the chief training officer of Galloway Training. “It really does feel like you’re cheating because you’re pushing the fatigue toward the end.” When Twiggs used the method for the first time at the 1995 Walt Disney World Marathon, he ended up with about a 15-minute personal record.
The 30-30 method — a 30-second run and 30-second walk — is one of the most popular ways to approach Jeffing, said Galloway. However, if a 30-second run is too challenging, you can scale it back: Twiggs often has walkers start with a 10-second run, 50-second walk, and then adjust from there.
“There’s an almost unlimited way to go about it,” said Kate Baird, a certified running coach and exercise physiologist at the Hospital for Special Surgery. That’s part of what makes it so beginner-friendly.
What are the benefits of the run-walk method?
First and foremost, run-walk is a type of aerobic workout that helps improve heart health, said Neel Chokshi, the medical director of the Sports Cardiology and Fitness Program at Penn Medicine. Consider it “interval training-lite,” he said. “The benefits of run-walk mirror general interval training in terms of the gains that people can get.” Specifically, alternating between high- and low-intensity efforts allows you to push hard when it’s time.
Over time, your heart will adapt to those repeated exposures to higher intensities, Chokshi said. Adaptations include being able to pump more blood with each heartbeat, a reduction in resting heart rate, and increased blood flow through the arteries.
Interval training also improves your VO2 max, or how efficiently your body uses oxygen during exercise. This results in better endurance and is also linked to longevity, said Chokshi.
Another great thing about Jeffing is that you can get all of these heart-health benefits while reducing the amount of high-impact stress you’re putting on your muscles, tendons, and ligaments. When Galloway first tried this method in the university’s beginner running course, a huge takeaway was that not one participant got injured during the program. That’s big, since beginner runners are at higher risk — they get injured at more than twice the rate as more experienced ones, according to a 2019 study out of the Netherlands.
Finally, you can’t ignore the mental benefits. If you want to scale up your cardio workouts but are daunted by the idea of running nonstop, Jeffing is a great way to overcome that mental hurdle, said Chokshi. Knowing you will have walk breaks coming can help you build the confidence that you can complete your workout — and finish it strong, said Twiggs.
Here’s how to try the run-walk method yourself
While there’s no set way to use the method, there are a few things you should keep in mind to make the most of it.
1. Get the right shoes
Because running brings a higher impact than walking, proper gear becomes even more important, said Twiggs. You might need more cushioning than a walking shoe, or some kind of motion control if your foot rolls inward or outward with each stride, he said. A running specialty store can help you pick out a pair that works for your anatomy and biomechanics.
2. Start small
While folks use run-walk in multihour marathons and training runs, these workouts don’t need to be nearly as long — and they shouldn’t be if you’re a beginner. Anywhere from 10 to 30 minutes is a great starting place, said Baird. Once you’re more comfortable with it, you can shoot for 30 to 45 minutes, Twiggs said.
3. Warm up your body
Getting your blood flowing before a workout can loosen up your muscles and gradually increase your heart rate, Chokshi said. You want to do a general, full-body warmup, since running includes pretty much every muscle in your body, including those in your lower body, upper body, and core. Moves like hamstring sweeps, lunges with thoracic rotation, and cat-cows are solid choices.
4. Choose your intervals
The 30-second run, 30-second walk tends to be the most popular utilization of the program, but “there’s no perfect run-walk ratio that everyone should be aspiring to,” said Twiggs. If you feel like you can’t catch your breath when running for 30 seconds, you can shorten that segment. If you feel strong, you can bump it up to 40 seconds, 60 seconds, or even a few minutes and see how your body reacts.
5. Slow down
Your run effort shouldn’t be a heart-pumping sprint — you want to keep it more moderate so you have the energy to do it all over again during your next interval. “A really good gauge is if you can carry on a conversation,” Twiggs said.
6. Make time for recovery
Even if you feel great after a workout, you shouldn’t do it every day. “Take one to two days between those workouts when it’s new,” Baird said. If you feel sore or tight in one particular spot, that might be your cue to give that area some extra attention during your warmup or next strength-training workout.
7. Don’t consider it a means to an end
The more you run-walk, the more you may want to play with your intervals, gradually increasing your run efforts as you gain more endurance. But it’s important to remember that you don’t have to use this method to reach a continuous running goal if that’s not what you want, said Galloway. You can stick with run-walk and still reap the benefits of running.
Every Cure, a biotech nonprofit started by a University of Pennsylvania researcher, has landed $76 million in federal funding to advance its artificial intelligence match-making tool that identifies existing drugs to treat rare diseases.
Over the next three years, Philadelphia-based Every Cure will use the funding from the Advanced Research Projects Agency for Health (ARPA-H) to pursue preclinical studies for at least 20 drugs that show promise for being repurposed for rare diseases with no other treatment options. The company will also pursue clinical trials to further test the safety and effectiveness of repurposing another 10 existing drugs.
The nonprofit was co-founded in 2022 by David Fajgenbaum, an associate professor at University of Pennsylvania, after his own experience with a rare disease.
He was diagnosed with Castleman disease as a medical student at Penn, and experimented in a campus lab with his own blood to try to find an off-label medication that could address his symptoms.
Every Cure’s AI tool expedites a drug discovery process that is otherwise often left to chance. When patients with rare diseases have few treatment options, doctors may scour medical journals or tap expert networks for leads on other drugs to try with mixed results.
The tool automates the process, using an algorithm to read massive biomedical data about diseases, medications, genes, and proteins. The tool looks for bits of data that diseases and medications may have in common that were previously unrecognized.
“This next phase will allow us to do the essential work of evaluating these potentially life-saving treatments in the lab and clinical trials, accelerating access to potential treatments for those who urgently need them,” Fajgenbaum, Every Cure’s President, said in a statement.
The new funding adds to $108 million in federal support the nonprofit has already received.
Intermittent fasting, one of America’s most popular diet trends, may be no more effective than simply cutting calories for weight loss, a new review of research shows.
Researchers found little to no difference in the amount of weight loss acrossmore than 20 studies comparing intermittent fasting, an eating pattern that cycles between periods of eating and fasting, with traditional dietary advice (which calls for restricting calories or the types of foods eaten).
The findings were published this month in the Cochrane Library, home to evidence reviews that are considered the gold standard for evaluating health evidence.
“From the results of this review, it doesn’t look like intermittent fasting is any better than regular dietary advice,” said Diane Rigassio Radler, a co-author on the study and a clinical nutrition professor at Rutgers School of Health Professions.
The data came from 22 randomized controlled trials involving nearly 2,000 participants across Europe, North America, China, Australia, and South America. Interventions ranged from four weeks to six months long, and looked at participants’ outcomes up to a year later.
In six of the trials, participants were picked at random to either practice intermittent fasting or do nothing. The difference in weight loss between the two groups was so small that it was not considered “clinically meaningful,” Radler said.
People generally need to lose 5% of their body weight to see health benefits. When the research team pooled the results of studies, they found weight loss from intermittent fasting slightly exceededthat of the group that did nothing, but remained below the 5% threshold.
“Anecdotally, people have told me that [intermittent fasting] might work for them, but the reasons for doing these systematic reviews is so that you can pull the evidence and make a stronger conclusion based on facts,” Radler said.
The studies focused on people in the overweight or obese categories as measured by BMI, a calculation of a person’s body fat based on their height and weight. The relevance of the research findings to people in the healthy weight category remains unknown. (While widely used, BMI is often not a good predictor of an individual’s health, as people’s body types can vary widely depending on race, gender, and age.)
The Inquirer spoke with Radler, who is also a registered dietitian by training, about the findings of the study and its implications, in an interview that was lightlyedited for length and clarity.
What is the theory behind intermittent fasting?
From a physiological perspective, there’s sound science in terms of why fasting might have an edge over just calorie restriction alone.
Number one, it involves calorie restriction. It’s thought to increase fat metabolism. There’s some hormonal stuff going on. It may enhance insulin sensitivity. When you’re fasting, you’re going to be breaking down fatty acids, and those can produce a significant source of energy.
But from the available studies we were able to evaluate, the findings are that intermittent fasting was not really different [in terms of weight loss].
There’s the theoretical framework, and then there’s what happens when you put it into reality.
Instead of intermittent fasting, what would you recommend?
It’s individualized. It depends on where the patient’s at and what they feel that they want to do.
The cardinal rule of thumb is you create a calorie deficit, and whether that’s with restricted eating or increased energy expenditure (such as through exercise), or a combination of both, you’re looking to achieve calorie restriction over time. Generally, you’re going to probably sustain that for at least 12 weeks, and then look at some outcomes.
We found that people who work with a registered dietitian on a weekly or every other week basis have the most success in terms of achieving weight management.
Your study found that intermittent fasting wouldn’t necessarily be effective. But would it be harmful for people to do?
You have to look at people’s baseline and their other comorbidities if they have any. But generally, we didn’t find that there were adverse effects, according to the studies that measured that as an outcome.
When you fast, there’s a risk of dehydration and risk of low blood sugar, but generally, the studies that measured the adverse effects didn’t find significant differences.
Are there any gaps in the research that you think should be looked into further?
There could be room for more research with a wider diversity of subjects, because most of the studies were in high-income countries. We have to look at some of the cultural differences.
Also, research with longer durations. We were not able to find studies that went out beyond 12 months of outcomes.